Ocular usg and it’s uses in ed and onsd normal values
Reading File
Finding Sources
Finding Sources
Searching PubMed
ocular ultrasound optic nerve sheath diameter emergency
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the information needed for a thorough answer. Here is the complete response:
Ocular Ultrasound in the Emergency Department
Overview
Bedside ocular ultrasound (US) is a fast, non-invasive, high-yield tool that emergency physicians can reliably perform with proper training. It was first described for ED use by Blaivas et al. in 2000, and multiple subsequent studies have confirmed its accuracy and clinical impact. - Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1484
Indications (Uses in the ED)
Ocular US is used as an adjunct for the following presentations:
- Altered or sudden loss of vision
- Ocular pain or trauma
- Suspected intraocular foreign body (FB)
- Headache with suspected raised ICP
- Head injury / altered mental status
- Facial swelling preventing direct examination
Conditions reliably diagnosed include:
| Condition | Key Findings |
|---|---|
| Retinal detachment | Hyperechoic flap in posterior chamber, tethered to optic nerve, moves with eye movement |
| Vitreous hemorrhage | Echogenic material in posterior chamber; stays horizontal, does not move like retinal detachment |
| Vitreous / posterior vitreous detachment | Flap not tethered to optic nerve |
| Intraocular foreign body | Hyperechoic structure with shadowing |
| Globe rupture | Deformed globe contour, collapsed anterior chamber |
| Lens dislocation | Lens displaced from normal position |
| Elevated ICP (via ONSD) | Widened optic nerve sheath |
| Retro-orbital hemorrhage | Retrobulbar collection |
| Papilledema | Optic disc swelling visible on B-scan |
Sensitivity for retinal detachment by emergency physicians: 92%, specificity: 91.4% - Rosen's Emergency Medicine, p. 3626
The pupillary light reflex (direct and consensual) can also be assessed via US when eyelid swelling prevents direct exam.
Equipment and Technique
Probe: High-frequency linear array transducer, 7.5 - 10 MHz (or higher). Use the ocular preset on the machine to minimize thermal bioeffects.
Setup:
- Patient supine or semi-reclined. Eyes closed, gaze straight ahead.
- Cover closed eyelid with a large Tegaderm dressing to keep gel off the eye.
- Apply generous gel over the Tegaderm - enough to fill the orbital sulcus completely.
- Use the no-pressure technique: barely touch the probe to the gel surface, with the hand stabilized on the forehead/nose/maxilla.
- Scan in orthogonal planes (longitudinal and transverse) with both low and high gain.
- Adjust depth to visualize the optic nerve (~1 cm behind the globe).
Why no pressure? Globe rupture is a relative contraindication only when the exam is obviously positive on inspection. In suspected (not obvious) open globe, the no-pressure US technique is justified because benefit outweighs risk, and delay increases adverse outcomes. - Roberts and Hedges', p. 1484
Pathology Images
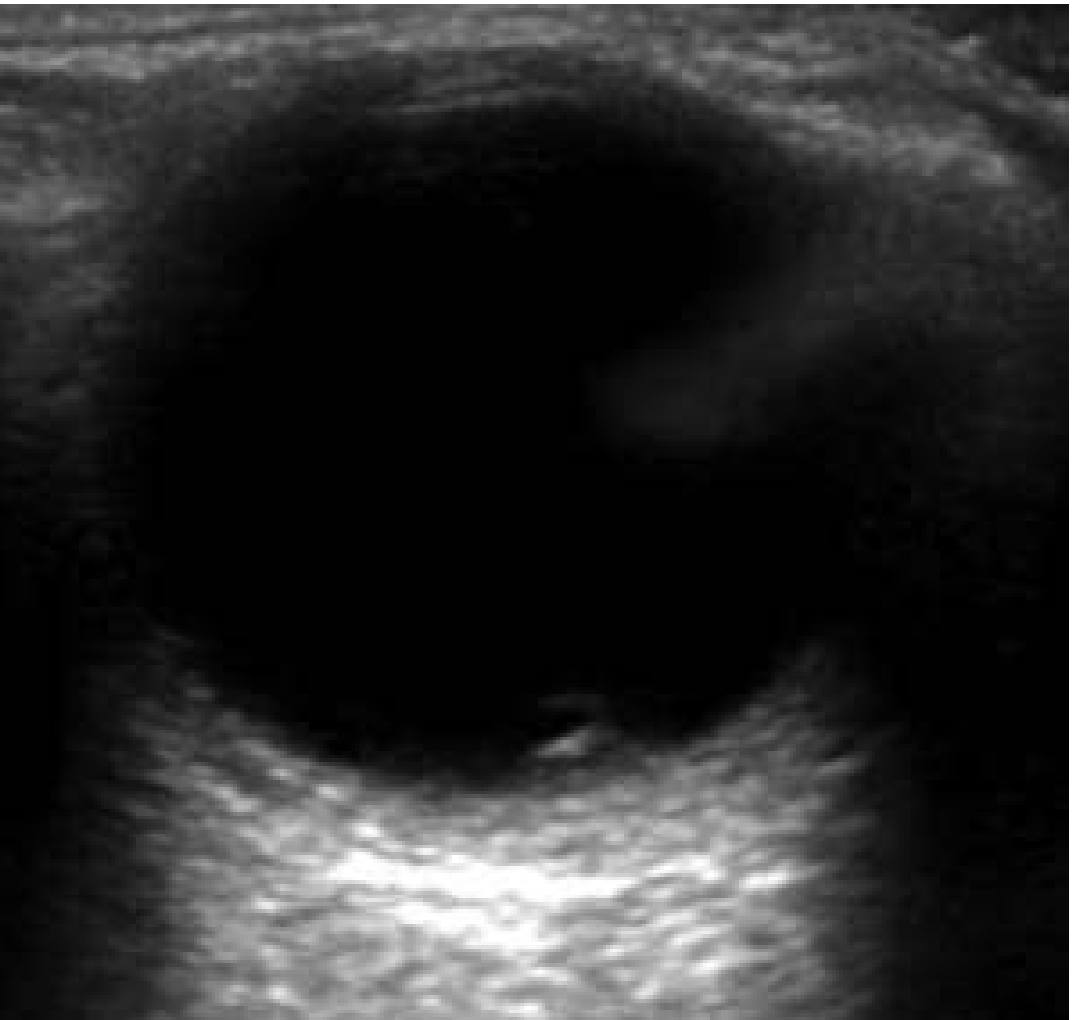
Normal eye - anterior and posterior chambers visible:

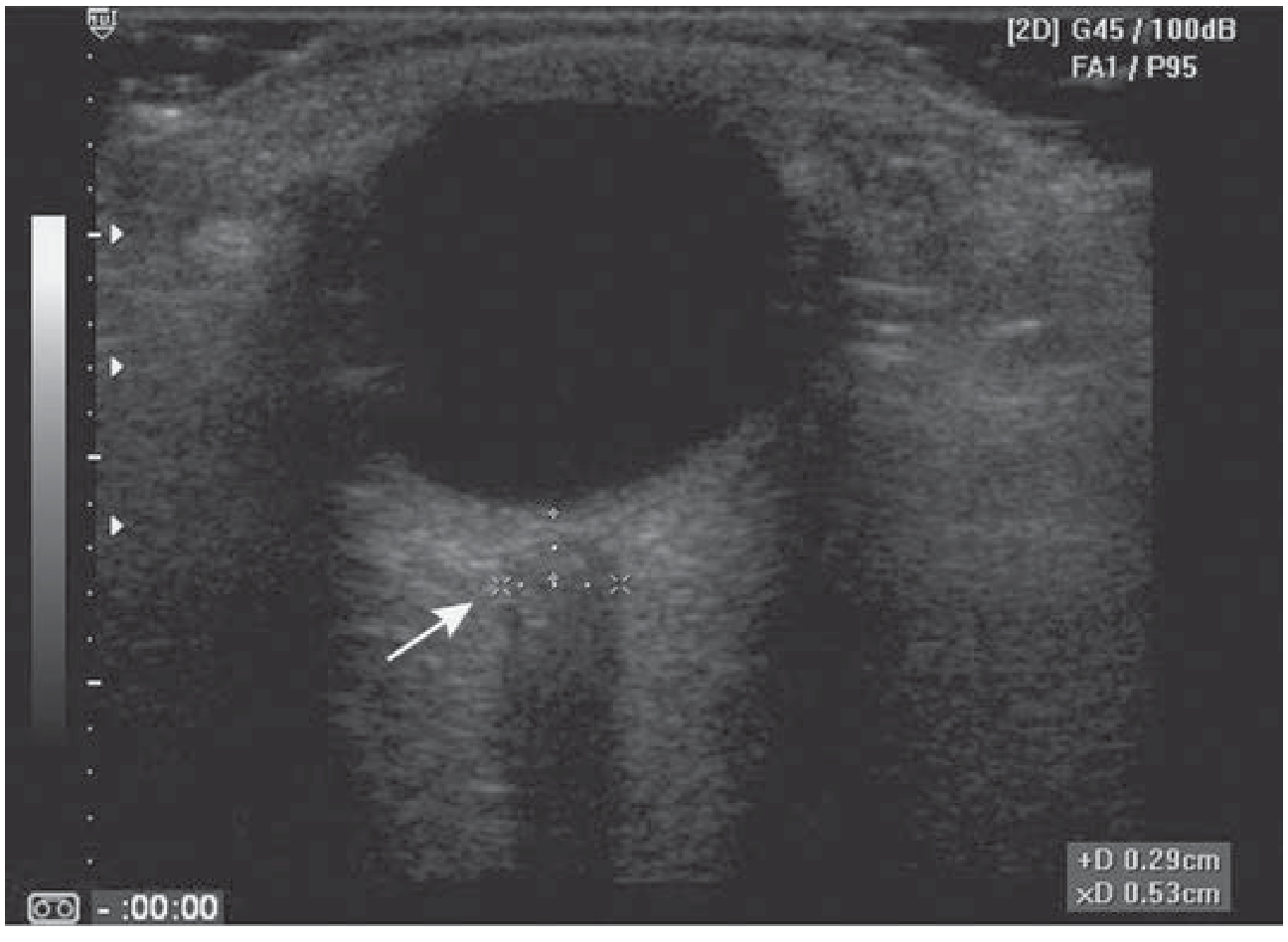
Papilledema / optic disc swelling (elevated ICP):
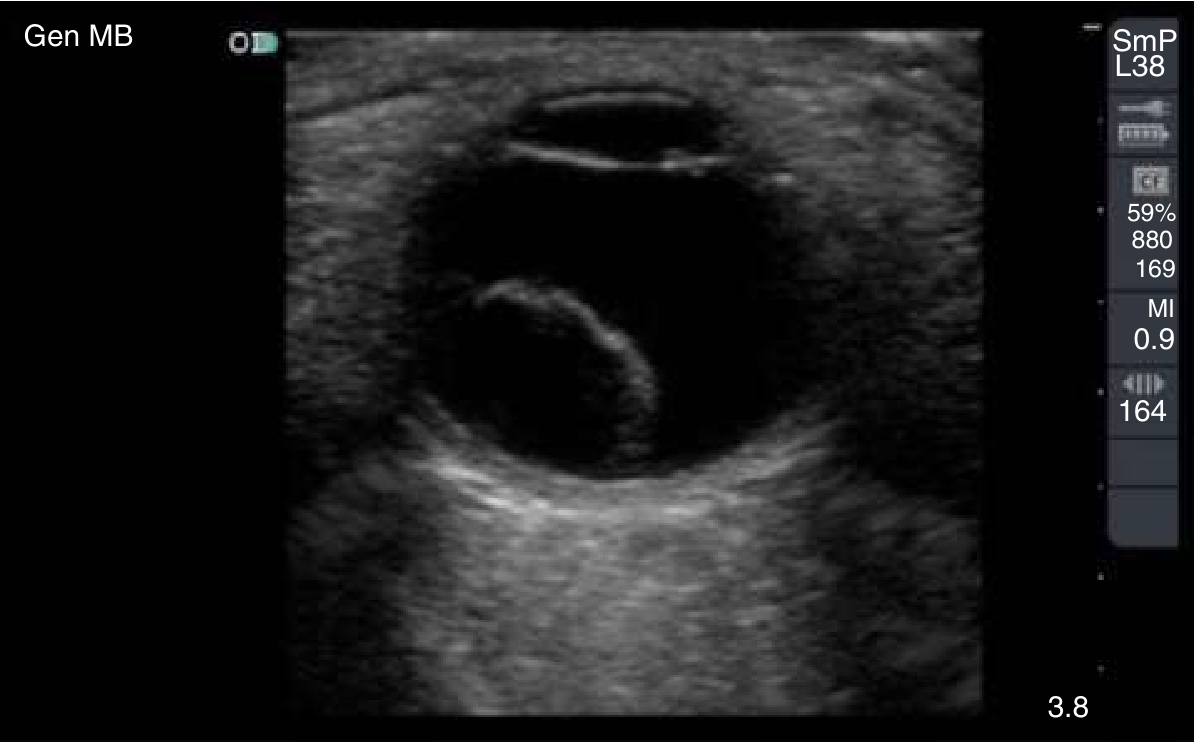
Retinal detachment - hyperechoic flap within the posterior chamber:
ONSD - Optic Nerve Sheath Diameter
Anatomy and Rationale
The optic nerve is a CNS structure surrounded by a dural sheath that is continuous with the intracranial subarachnoid space. When ICP rises, CSF is transmitted into the perineural space, causing the sheath to expand - this is detectable on ultrasound within seconds to minutes of ICP elevation.
How to Measure
- Position patient supine or at 20-30 degrees head-up tilt.
- Ask the patient to deviate the examined eye ~10 degrees laterally - this aligns the optic nerve with the US beam and prevents falsely widened measurements from oblique imaging.
- Place caliper markers 3 mm posterior to the posterior wall of the globe (this point gives the best contrast and highest reproducibility).
- Measure the width of the optic nerve sheath (outer edge to outer edge).
- Obtain at least two to three measurements and average them.
- Measure both eyes.
Why 3 mm? The optic nerve sheath distensibility is greatest at this point, making it the most sensitive and reproducible location. - Tintinalli's Emergency Medicine, p. 1601
ONSD Normal Values and Thresholds
| Population | Normal (Upper Limit) | Abnormal (Suggests Raised ICP) |
|---|---|---|
| Adults | ≤ 5.0 mm | > 5.7 - 6.0 mm |
| Children | ≤ 4.5 mm | Proportionately smaller |
| Infants | ≤ 4.0 mm | > 4.0 mm |
- A value < 5 mm is considered normal in adults.
- A value > 6 mm is considered clearly abnormal.
- The 5 - 6 mm zone is a gray area where clinical context and repeat measurement matter.
- The best accuracy cutoff for ICP > 20 mmHg is 5.7 - 6.0 mm:
- Sensitivity: 87% - 95%
- Specificity: 79% - 100%
Sources: Tintinalli's, p. 1600-1601; Rosen's, p. 4257; Roberts and Hedges', p. 1485
Differential for Widened ONSD
Not every widened ONSD equals raised ICP. Other causes:
- Anterior orbital mass
- Optic neuritis
- Orbital trauma
- Cavernous sinus mass
Clinical Application in the ED
- ONSD-US is used when ICP elevation is suspected: head trauma, altered mental status, meningitis, hypertensive emergency, space-occupying lesions.
- Rosen's explicitly recommends avoiding lumbar puncture when ONSD > 5 mm, alongside other signs of raised ICP (papilledema, mass lesion on CT). - Rosen's EM, p. 4263
- It is not a replacement for CT/MRI but provides an immediate bedside estimate in unstable patients or resource-limited settings.
Recent Evidence
A 2024 systematic review and meta-analysis (PMID 39142382) specifically examined ONSD accuracy for raised ICP in pediatric patients, confirming good diagnostic performance in children - supporting age-adjusted thresholds (≤ 4.5 mm in children, ≤ 4.0 mm in infants).
Key Contraindications / Cautions
- Known, obvious globe rupture - do not scan; risk of vitreous extrusion.
- Suspected but not obvious globe rupture - use strict no-pressure technique; benefit typically outweighs risk.
- Excessive scan time should be avoided to stay within thermal exposure limits (use ocular preset).
Summary Table
| Feature | Detail |
|---|---|
| Probe | Linear, 7.5-10 MHz |
| Preset | Ocular |
| Technique | No pressure; Tegaderm over eyelid |
| ONSD measurement site | 3 mm behind globe |
| ONSD normal (adult) | ≤ 5.0 mm |
| ONSD abnormal (adult) | > 5.7-6.0 mm |
| ONSD normal (child) | ≤ 4.5 mm |
| ONSD normal (infant) | ≤ 4.0 mm |
| Sens/Spec for ICP > 20 mmHg | 87-95% / 79-100% |
| Retinal detachment Sens/Spec | 92% / 91.4% |
This is a shared conversation. Sign in to Orris to start your own chat.