Entrohepatic circulation mbbs short essay
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile a well-structured MBBS short essay answer.
Enterohepatic Circulation
Definition
Enterohepatic circulation (EHC) refers to the cyclical process by which bile acids (and certain other substances) are secreted by the liver into the bile, pass through the biliary tract and small intestine, are reabsorbed - primarily in the terminal ileum - and returned to the liver via the portal vein, from where they are re-secreted into bile. It is essentially a recycling loop between the intestine and the liver.
The anatomical components include: the liver, biliary tract, gallbladder, small intestine (especially the terminal ileum), portal venous circulation, and to a lesser extent the colon and systemic circulation.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1204
Bile Acid Synthesis (Starting Point)
In the liver, primary bile acids - cholic acid and chenodeoxycholic acid - are synthesized from cholesterol. The rate-limiting enzyme is cholesterol 7α-hydroxylase (CYP7A1). These primary bile acids are then conjugated with glycine or taurine in the hepatocyte to form primary bile salts, which are more water-soluble and amphipathic.
- Lippincott Illustrated Reviews: Biochemistry, 8th ed, p. 633
- Sabiston Textbook of Surgery, p. 1873
Steps of the Cycle
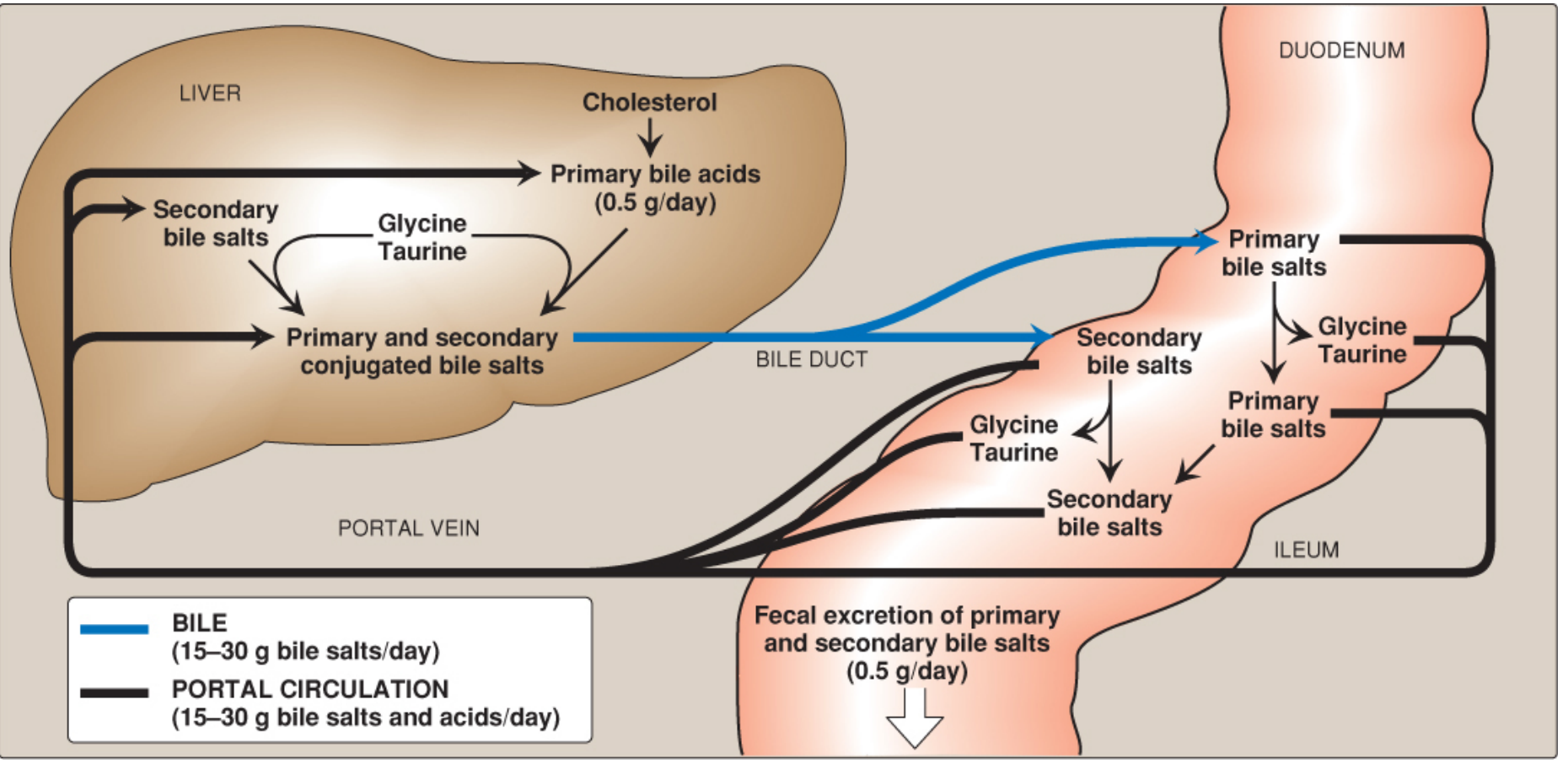
1. Hepatic secretion: The liver actively secretes conjugated (primary + secondary) bile salts via the bile salt export pump (BSEP/ABCB11) into bile canaliculi, and bile flows into the bile duct.
2. Gallbladder storage: During fasting, bile is concentrated ~10-fold in the gallbladder. With ingestion of a meal, cholecystokinin (CCK) released from the duodenal mucosa causes gallbladder contraction and relaxation of the sphincter of Oddi, releasing a concentrated bolus of mixed micelles into the duodenum. The intraluminal bile acid concentration in the small intestine rises to 5-10 mmol/L, well above the critical micellar concentration (~1.5 mmol/L).
3. Intestinal transit and micelle formation: Bile salts emulsify dietary fats, form mixed micelles with fatty acids, monoglycerides, and cholesterol, and facilitate their absorption across the intestinal mucosa. They also enhance pancreatic lipase activity.
4. Bacterial modification (secondary bile acids): In the terminal ileum and colon, intestinal bacteria deconjugate (remove glycine/taurine) and dehydroxylate (remove the C-7 hydroxyl group) primary bile acids, forming secondary bile acids - deoxycholic acid (from cholic acid) and lithocholic acid (from chenodeoxycholic acid). Lithocholic acid is only poorly reabsorbed.
5. Ileal reabsorption: Conjugated bile salts are actively reabsorbed in the terminal ileum (the dominant mechanism) via the apical sodium-bile acid transporter (ASBT/SLC10A2). Unconjugated bile acids can also be passively absorbed along the entire small intestine. The reabsorbed bile acids are transported across the enterocyte basolateral membrane by the organic solute transporter (OST-α/β) into the portal blood, where they are transported bound to albumin.
6. Portal return to the liver: The portal vein carries reabsorbed bile salts to the liver. Hepatocytes extract them efficiently (up to 90% first-pass extraction) via the Na⁺-taurocholate cotransporting polypeptide (NTCP/SLC10A1) and organic anion transporting polypeptides (OATPs). They are reconjugated and resecreted into bile, completing the cycle.
- Costanzo Physiology, 7th ed, p. 378
- Harrison's Principles of Internal Medicine, 22e, p. 2771
- Sleisenger and Fordtran's, p. 1204
Quantitative Facts (Important for Exams)
| Parameter | Value |
|---|---|
| Total bile acid pool | 2-4 g |
| Daily bile secretion into intestine | 15-30 g/day |
| Efficiency of ileal reabsorption | ~95% |
| Daily fecal loss | 0.2-0.6 g/day |
| Daily hepatic synthesis to replace loss | ~0.5 g/day |
| Number of cycles per day | 5-10 times |
The liver replenishes exactly the amount lost in feces. Synthesis is regulated by negative feedback: bile acids returning to the liver inhibit CYP7A1. Additionally, bile acids in the ileum stimulate release of fibroblast growth factor 19 (FGF19), which travels to the liver and further suppresses CYP7A1, coordinating the feedback loop.
- Harrison's 22e, p. 2771; Costanzo Physiology, p. 378
Enterohepatic Circulation of Bilirubin
EHC does not apply only to bile acids. Bilirubin also undergoes a form of EHC:
- Conjugated bilirubin secreted in bile passes into the intestine without reabsorption by the gallbladder or intestinal mucosa.
- Intestinal bacteria convert conjugated bilirubin to urobilinogens (colorless compounds) in the ileum and colon.
- Urobilinogen is reabsorbed and returned to the liver via the portal vein, where it is re-excreted in bile (EHC of urobilinogen).
- A small amount escapes hepatic extraction, enters the systemic circulation, and is cleared by the kidneys - this is the source of urinary urobilinogen (normal: ≤4 mg/day).
- Oxidized urobilinogen gives stercobilin (brown color of stool) and urobilin (yellow color of urine).
Clinical relevance: In hemolysis, more bilirubin enters the gut → more urobilinogen formed and reabsorbed → raised urinary urobilinogen. In obstructive jaundice or with antibiotics killing gut bacteria, urobilinogen formation is reduced → urinary urobilinogen is absent/reduced and stool becomes pale.
- Goldman-Cecil Medicine, p. 780; Sabiston Textbook of Surgery, p. 1873
Functions of Enterohepatic Circulation
- Conservation of bile acids - prevents loss of these metabolically expensive molecules; >95% are recycled.
- Fat digestion and absorption - bile acids form micelles to solubilize fat and fat-soluble vitamins (A, D, E, K) and lipophilic drugs.
- Cholesterol homeostasis - cholesterol is consumed in bile acid synthesis and excreted in feces via micelles; EHC is the primary mechanism for eliminating excess cholesterol from the body.
- Water regulation - bile salts regulate water movement from hepatocytes into bile and water absorption through the small bowel.
- Biliary secretion (choleretic effect) - recirculated bile salts stimulate hepatic bile secretion.
- Sabiston Textbook of Surgery, p. 1873
Clinical Significance / Disorders
| Condition | Mechanism | Effect |
|---|---|---|
| Ileal resection/Crohn's disease (terminal ileum) | Interruption of active reabsorption site | Loss of bile acids in feces, reduced bile acid pool, steatorrhea, fat-soluble vitamin deficiency |
| Bile acid malabsorption (Type 3) | Primary ASBT defect | Bile acids reach colon → secretory diarrhea (cholerheic enteropathy) |
| Cholesterol gallstones | Reduced bile acid pool → cholesterol supersaturation in bile | Cholelithiasis |
| Cholestyramine (bile acid sequestrant) | Binds bile acids in gut, prevents reabsorption | Lowers LDL cholesterol (forces hepatic synthesis from cholesterol); used in hypercholesterolemia; also interrupts EHC of drugs like digoxin, warfarin |
| Obstructive jaundice | Bile cannot enter gut | No urobilinogen in urine, pale stools |
| Drug interactions | Drugs with EHC (e.g., digoxin, oral contraceptives, diazepam) have prolonged action; cholestyramine can shorten their effect | Pharmacokinetic implications |
Summary
Enterohepatic circulation is a highly efficient conservation mechanism whereby bile acids (and other substances like bilirubin/urobilinogen) cycle between the liver and intestine 5-10 times daily. The terminal ileum is the key reabsorption site. The pool size (2-4 g) is maintained by compensatory hepatic synthesis (~0.5 g/day) regulated by CYP7A1 under feedback inhibition by bile acids and FGF19. Disruption of EHC - as in ileal disease or resection - leads to steatorrhea, bile acid diarrhea, fat-soluble vitamin deficiency, and gallstone formation.
This is a shared conversation. Sign in to Orris to start your own chat.