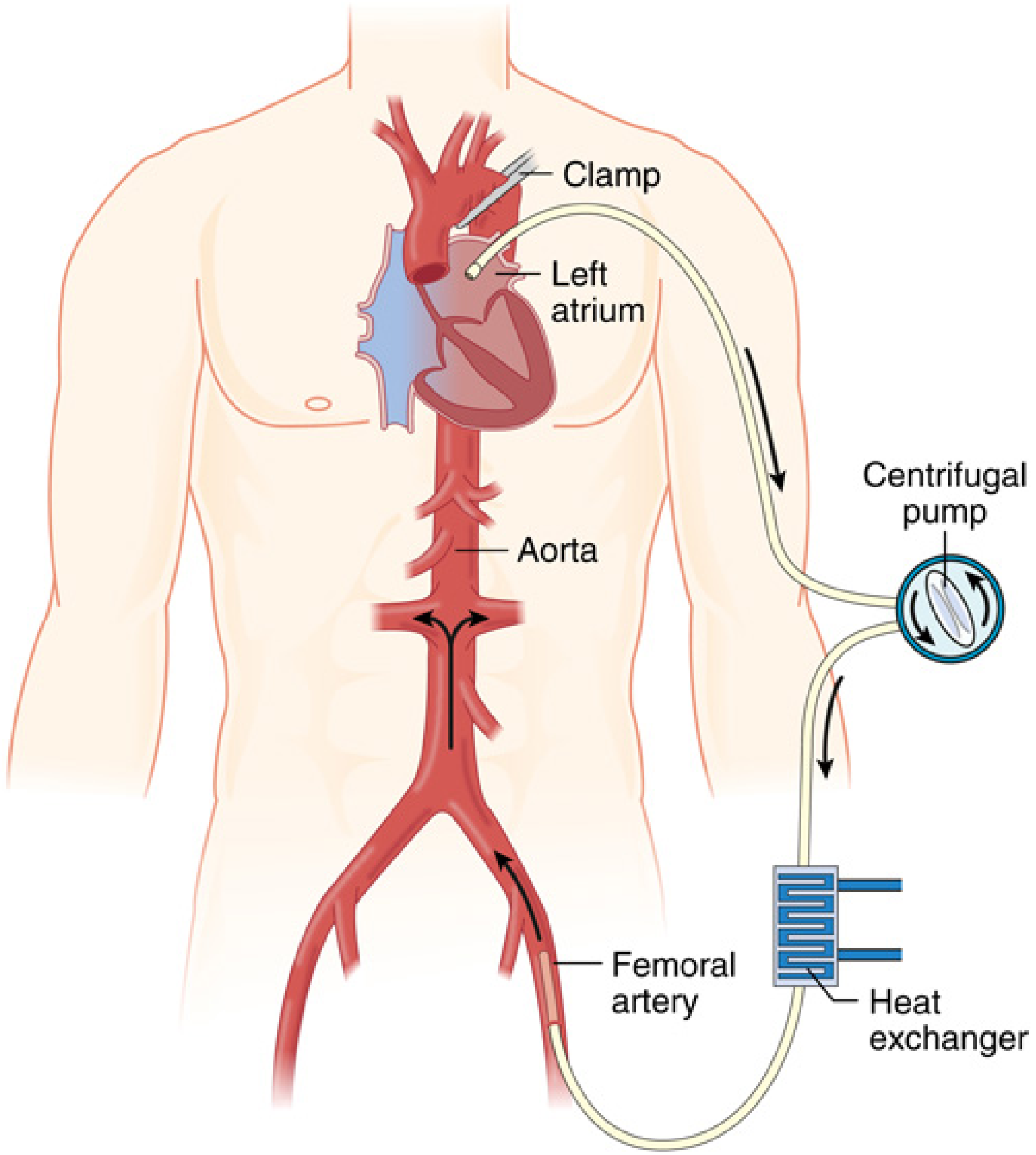
Principles of left heart bypass (left aorta femoral bypass)
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the textbook content and diagrams needed for a comprehensive answer.
Left Heart Bypass (Left Atrio-Femoral Bypass)
Left heart bypass (LHB), also called partial bypass or left atrial-to-femoral bypass, is a form of partial extracorporeal circulatory support used during open repair of the descending thoracic and thoracoabdominal aorta. It is not full cardiopulmonary bypass - the right heart and lungs continue to function normally.
Why It Is Needed
When a vascular clamp is applied to the descending thoracic aorta, two major problems arise simultaneously:
- Proximal hypertension / increased LV afterload - the left ventricle suddenly ejects against a closed circuit, dramatically increasing wall stress and myocardial oxygen demand.
- Distal ischemia - all organs below the clamp (spinal cord, kidneys, viscera, lower limbs) are cut off from perfusion.
LHB solves both problems at once by diverting blood from the left side of the heart around the clamped segment and returning it to the distal aorta.
- Miller's Anesthesia, 10e - "The application of vascular clamps to this major vessel acutely increases the afterload of the heart and produces global ischemia in all parts of the body distal to the clamp."
Circuit Anatomy and Flow Direction
The basic circuit is: Left atrium → centrifugal pump → femoral artery
| Component | Role |
|---|---|
| Left atrial cannula (venous inflow) | Drains oxygenated pulmonary venous return from the left atrium |
| Centrifugal pump (Biomedicus) | Active, flow-adjustable pump - not gravity dependent |
| Heat exchanger (optional in simple circuit) | Maintains normothermia or induces mild hypothermia |
| Femoral artery cannula (arterial return) | Delivers blood to distal aorta, perfusing viscera, spinal cord, and lower limbs |
Since only the left side of the heart is bypassed, pulmonary gas exchange is still occurring - no oxygenator is required in the basic circuit.
Simple vs. Complete LHB Circuit
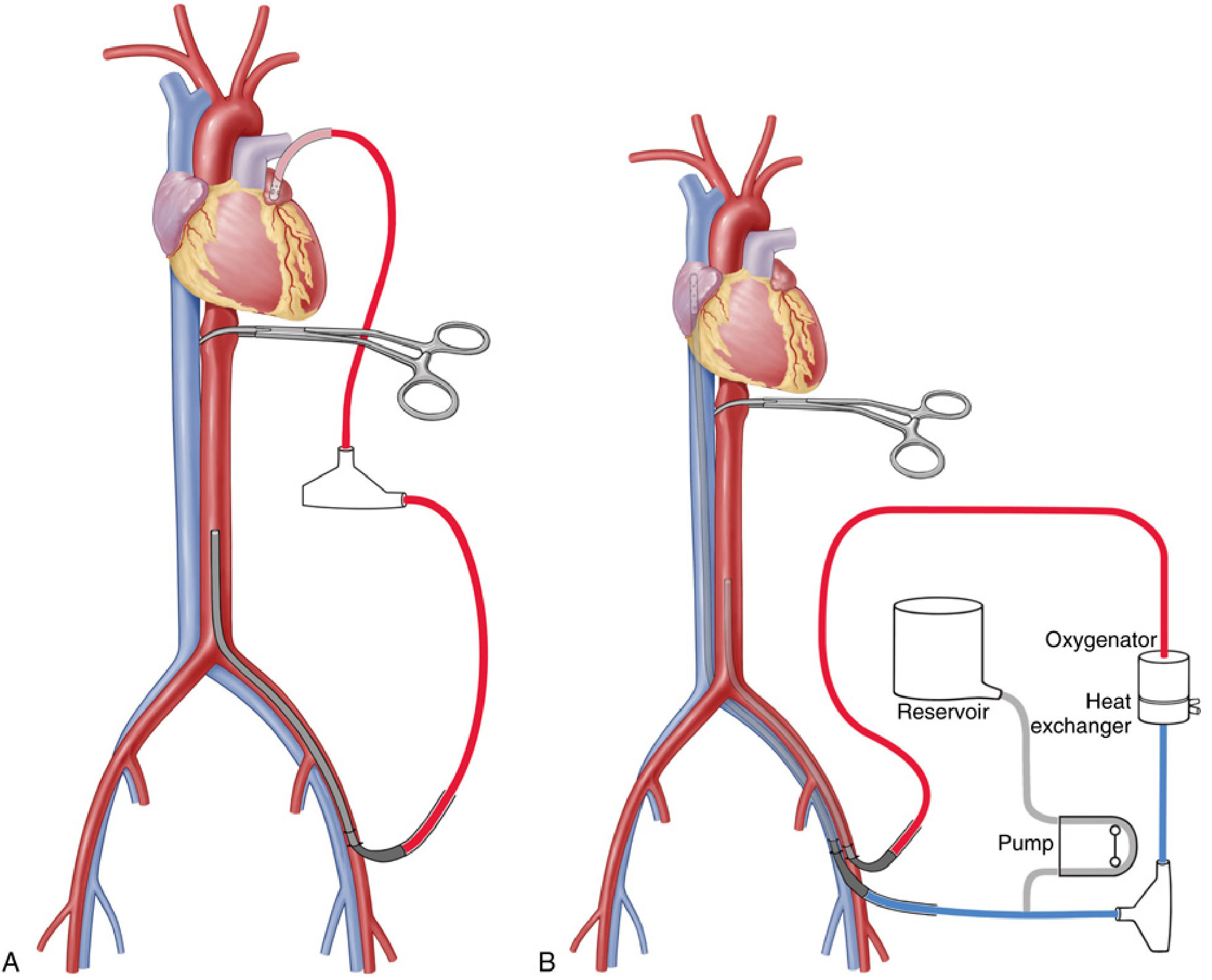
Simple circuit:
- Left atrium → centrifugal pump → femoral artery
- No oxygenator needed (lungs still functioning)
- Reduced extracorporeal surface area = less contact activation, less heparin required
Complete (complex) circuit:
- Adds an oxygenator (for patients with single-lung ventilation-related hypoxia or respiratory compromise)
- Adds a reservoir (for rapid fluid/blood product administration in haemorrhage)
- Adds a heat exchanger (active temperature control)
- Required for patients with pre-existing lung dysfunction or traumatic lung injury
The key difference from full CPB: the reservoir is not in the primary blood pathway. This reduces blood-surface contact, attenuating clotting activation.
- Miller's Anesthesia, 10e - "The major difference between a complete LHB circuit and the standard CPB circuit is the position of the reservoir in the circuit... With the reservoir out of the pathway of the blood, the effective surface area of the ECC is reduced; this reduction attenuates contact activation of the blood and minimizes the need for high-dose heparinization."
Anticoagulation
Full-dose systemic heparin (300-400 units/kg targeting ACT >400s) is not needed because:
- The circuit uses heparin-coated tubing
- Reduced extracorporeal surface area minimises thrombus risk
Typical dose: 100 units/kg (partial heparinisation), maintaining ACT of 180-250 seconds.
Variations of the Inflow Cannulation Site
While the left atrium is the standard inflow, alternatives exist:
| Inflow site | Haemodynamic effect |
|---|---|
| Left atrium (standard) | Reduces LV preload - cardiac output is reduced; LV is unloaded from the filling side |
| Aortic arch / proximal descending thoracic aorta | Reduces LV afterload - the ventricle pumps but against a lower resistance |
Either way, proximal hypertension is controlled, ventricular work is reduced, and distal perfusion is maintained.
- Miller's Anesthesia, 10e - "With left atrial cannulation, the left ventricle is relieved of preload and cardiac output is reduced. Either way, proximal hypertension is controlled, the work of the ventricle is decreased, and perfusion is provided to the distal aorta."
Haemodynamic Management Goals
The core management target is to maintain arterial blood pressure above 60 mmHg both proximal and distal to the aortic cross-clamp throughout the procedure.
- Initial pump flow is typically set to ~50% of the patient's cardiac output at the time of proximal clamp application
- Flow is then titrated continuously to hit target proximal and distal pressures
- Vasodilators are rarely required at initiation
- Communication between surgeon, anaesthesiologist, and perfusionist is mandatory
During reimplantation of visceral and renal arteries, pump flow is deliberately reduced so distal perfusion goes primarily to the lower limbs only, while the visceral vessels are being sewn in.
Key Physiological Benefits
| Benefit | Mechanism |
|---|---|
| Spinal cord protection | Continuous perfusion of intercostal and lumbar arteries (including artery of Adamkiewicz) during cross-clamping |
| Visceral/renal protection | Delivery of oxygenated blood below the clamp; balloon perfusion cannulas can selectively perfuse celiac and SMA directly |
| Reduced LV work | Unloading of preload (left atrial cannulation) or afterload (arch cannulation) |
| Reduced risk of paraplegia | Avoids prolonged ischaemia; combined with CSF drainage, reduces risk significantly |
| Haemorrhage management | Complete circuit reservoir allows rapid volume replacement |
Organ Protection Adjuncts Used Alongside LHB
LHB is rarely used alone. The complete neuroprotection strategy for Crawford extent I/II thoracoabdominal repairs includes:
- Cerebrospinal fluid (CSF) drainage - reduces intraspinal pressure, improving spinal cord perfusion pressure (Class I, Level B in current guidelines; RCT showed paraplegia reduction from 13% to 2.6%)
- LHB during proximal anastomosis - ensures distal perfusion while the aorta is clamped proximally
- Selective visceral perfusion - balloon catheters from the LHB circuit directed into celiac and SMA orifices
- Cold renal perfusion (4°C crystalloid, ± methylprednisolone) - reduces renal ischaemic injury
- Mild permissive hypothermia (32-34°C nasopharyngeal) - slows metabolic rate of vulnerable organs
- Motor evoked potential (MEP) monitoring - guides decision to reimplant intercostal arteries (T8-L1 most important)
- Sequential aortic clamping - clamp moved progressively distally as each anastomosis is completed, restoring flow segment by segment
Surgical Approach
- Left thoracotomy provides the operative exposure; the left lung is deflated using a double-lumen endotracheal tube or bronchial blocker to expose the left atrium and thoracic aorta
- The left inferior pulmonary vein or left atrial appendage is the usual cannulation site for inflow
- The left femoral artery is exposed for return cannulation
- Moderate hypothermia (32°C) is maintained throughout bypass
- After distal anastomosis completion, pump flow is increased and the patient actively warmed to 37°C before weaning
LHB vs. Full CPB vs. Clamp-and-Sew
| Feature | Clamp-and-sew | LHB | Full CPB |
|---|---|---|---|
| Distal perfusion | None | Yes | Yes |
| Oxygenator needed | No | No (simple) / Yes (complex) | Yes |
| Heparin requirement | Minimal | Partial (100 U/kg) | Full (300-400 U/kg) |
| Spinal cord protection | Poor for long cross-clamp times | Good | Good |
| Complexity | Lowest | Moderate | Highest |
| LV unloading | No | Yes | Yes |
| Suitable for | Short, simple DTAA | Most DTAA and TAAA | Complex arch involvement, DHCA needed |
- Current Surgical Therapy, 14e - "Two surgical techniques that are commonly utilized to repair DTAA and TAAAs are the 'clamp-and-sew' technique versus the use of distal aortic perfusion through a left heart bypass circuit. Each technique has been found to be efficacious and is often surgeon- and centre-dependent."
Clinical Notes and Complications
- Atrial fibrillation - occurs in ~15% of patients when hypothermia (30°C) is combined with left atrial cannulation; most revert to sinus rhythm on rewarming, but cardioversion may be required
- Single-lung ventilation hazards - patients with pre-existing lung disease or traumatic injury may desaturate; the complete LHB circuit (with oxygenator) is then preferred
- Blood loss - these are high-risk cases for haemorrhage; the complete circuit reservoir allows rapid resuscitation
- Hypothermia - large left thoracotomy exposure over prolonged procedures promotes heat loss; active warming via circuit heat exchanger is important
- Endovascular era - widespread adoption of TEVAR (thoracic endovascular aortic repair) has significantly reduced the use of open LHB procedures in contemporary practice
Sources:
- Miller's Anesthesia, 10e, Chapters 50 and 52 (Left Heart Bypass; Descending TAA repair)
- Schwartz's Principles of Surgery, 11e, Chapter on thoracoabdominal aortic aneurysms (Current strategy for spinal cord and visceral protection)
- Current Surgical Therapy, 14e, Strategies for thoracic and thoracoabdominal aortic reconstruction
This is a shared conversation. Sign in to Orris to start your own chat.