Septal perforation treatment and stages of it
Reading File
Finding Sources
Finding Sources
Searching the Web
nasal septal perforation treatment stages classification 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC9443041
Reading File
Excellent - I have very comprehensive information now. Let me compile the full answer.
Nasal Septal Perforation: Classification, Stages, and Treatment
A nasal septal perforation (NSP) is a full-thickness defect of the nasal septum involving loss of cartilage and/or bone along with their mucoperichondrium and mucoperiosteum. It converts the normal laminar airflow through the nose into turbulent airflow, leading to the characteristic symptoms.
Causes
| Category | Examples |
|---|---|
| Trauma/Iatrogenic | Septoplasty/SMR, nose-picking, septal haematoma, bilateral cauterization |
| Drugs/Toxins | Cocaine abuse, overuse of nasal decongestants or steroid sprays, chrome salts |
| Infection | Syphilis, tuberculosis, fungi |
| Vasculitis/Autoimmune | Granulomatosis with polyangiitis (Wegener's), SLE, relapsing polychondritis, dermatomyositis |
| Tumour | Sinonasal malignancy |
| Idiopathic | ~20% of cases |
Prevalence after submucous resection (SMR): 17-25%; after septoplasty: 1.4-5%. - Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1
Symptoms
- Nasal obstruction (turbulent airflow sensation)
- Crusting (drying of mucosa at the perforation edge)
- Epistaxis (from the raw perforation edges)
- Whistling on nasal breathing (especially anterior perforations)
- Malodorous discharge
- Empty nose sensation
- Long-term untreated perforations can cause saddle-nose deformity and tip ptosis from loss of septal support, and chronic osteitis of the bony septum - Cummings Otolaryngology
More than half of perforations are asymptomatic and require no treatment. The more anterior the perforation, the more symptomatic it tends to be. - Scott-Brown's
Classification / Stages
1. By Size (Traditional)
| Grade | Size |
|---|---|
| Small | < 1 cm |
| Medium | 1-2 cm |
| Large | > 2 cm |
2. By Location
| Location | Description |
|---|---|
| Anterior | Anterior nose to the head of middle turbinate (most common - ~75% of all perforations) |
| Posterior | From head of middle turbinate to the choana (usually asymptomatic) |
| Low | Close to the nasal floor |
| High | Close to the nasal dorsum |
3. Sapmaz Classification (2018) - Ratio-Based, 4 Groups
A newer, surgically practical classification based on the ratio of perforation vertical length to total vertical septal length:
| Group | Definition | Clinical Label |
|---|---|---|
| Group 1 | < 1/4 of total vertical septal length | Small |
| Group 2 | 1/4 to 1/2 of total vertical septal length | Medium |
| Group 3 | 1/2 to 3/4 of total vertical septal length | Large |
| Group 4 | > 3/4 of total vertical septal length | Very large |
This classification helps surgeons select the appropriate technique and predict surgical success rates. (Sapmaz et al., 2018, PMC9443041)
Management
Scott-Brown's divides management into three main groups: - Scott-Brown's Vol 1, p.1200
Group 1 - Prevention
- Correct nasal spray technique (use opposite hand to avoid jet impact on the septum)
- Stop causative agents (cocaine, decongestants, steroid sprays)
- Any ulceration after starting steroid sprays: withdraw medication immediately
- Intraoperative: close any fenestrations immediately during septoplasty; maintain the correct subperichondrial plane
Group 2 - Conservative (Medical) Management
For asymptomatic or mildly symptomatic perforations:
- Saline nasal irrigation and moisturizing sprays/ointments - keeps mucosa moist, reduces crusting and bleeding
- Topical antibiotics for crusting management
- Avoidance of nose picking and nose blowing
- Silastic biflanged septal button prosthesis - a non-surgical occlusive device that relieves whistling, obstruction, and bleeding; first-line for patients unwilling or unfit for surgery (see diagram below)
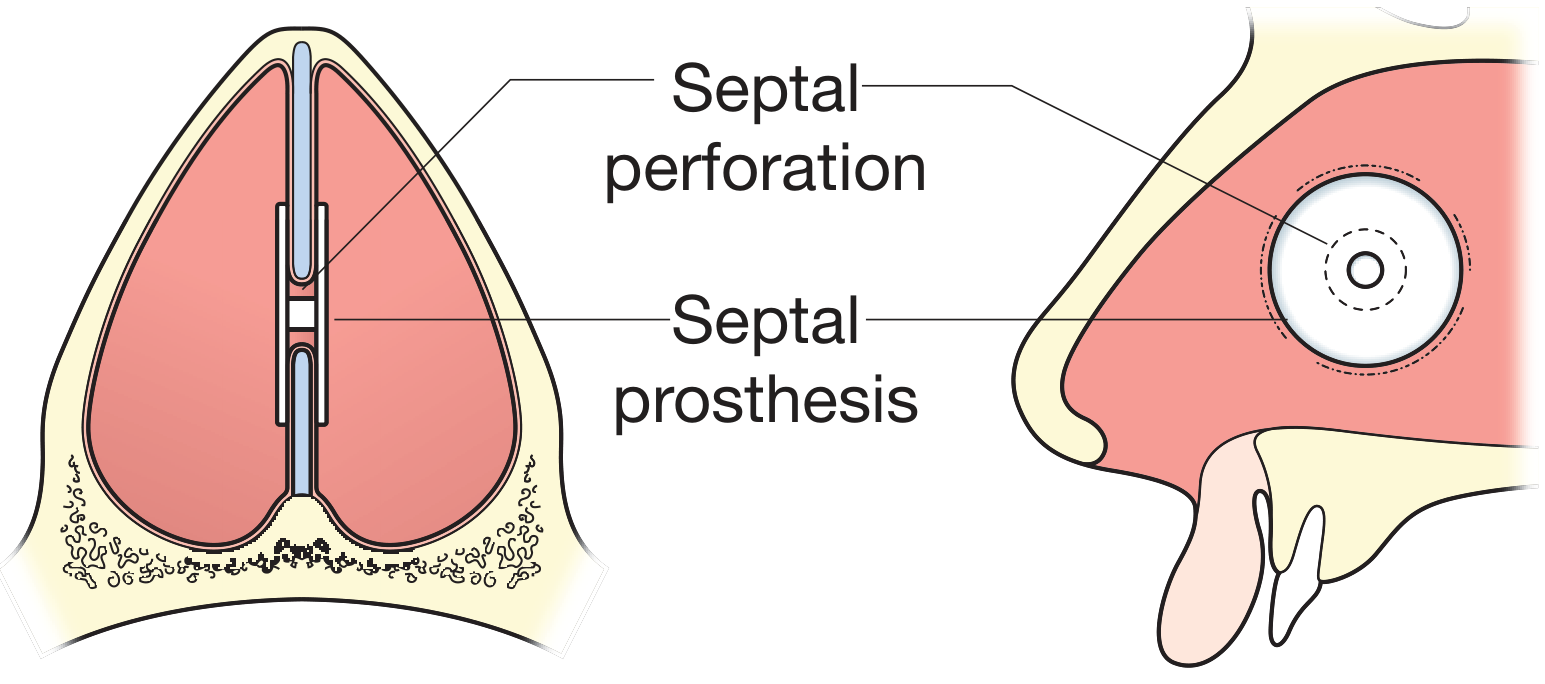
Anterior cross-section showing the septal button spanning the perforation, and a lateral view showing its position. - Bailey & Love's, Fig. 51.42
Group 3 - Surgical Repair
Indicated for symptomatic patients who fail conservative measures. Seldom heal spontaneously.
General surgical principles:
- Bilateral mucoperichondrial flap mobilization with individual layer closure
- Interposition connective tissue graft (sandwich technique)
- Three-layer repair concept: bilateral mucosa + middle graft layer
Preferred technique (Cummings/Kridel):
- External rhinoplasty (open) approach - provides superior exposure, especially for large perforations
- Nasal floor advancement flaps bilaterally
- Interposition graft: temporalis fascia, acellular human dermis (AlloDerm), costal perichondrium, or other fascia
Specific surgical options by size:
| Perforation Size | Surgical Approach |
|---|---|
| Small-Medium | Endonasal mucoperichondrial rotation/advancement flaps + interposition graft |
| Large | External rhinoplasty approach + nasal floor advancement flaps + fascia interposition |
| Very Large / Failed repair | Fascia lata graft, PDS absorbable plate for stabilization (novel techniques) |
Alternative/adjunct options:
- Inferior turbinate flap for perforation repair
- Anterior ethmoid artery septal flap
- Cartilage or synthetic material grafts with local flap cover
- Enlargement of the perforation with mucosal folding around the posterior edge - paradoxically used in cases with significant posterior edge whistling/bleeding to stabilize it
Key point from Cummings: "Almost all current literature supports septal perforation closure with intranasal flaps and connective tissue interposition grafts." - Cummings Otolaryngology, p.580
Workup Before Treatment
When etiology is unclear or inflammatory signs are present:
- Full blood count, ESR, urea & electrolytes, urinalysis
- c-ANCA (Wegener's/GPA)
- Treponemal serology (syphilis)
- ACE titres (sarcoidosis)
- Chest X-ray
- Nasal swab
- Biopsy - only if unexplained etiology, persistent inflammation, or irregular margin (to exclude malignancy, vasculitis, mycobacteria, fungi). Biopsy can convert an inactive perforation to an active state and cause enlargement, so it is not done routinely.
Outcome Assessment
The Nasal Septal Perforation Questionnaire (Scott-Brown's) assesses four key symptom domains on a 0-10 scale:
- Crusts/scabs
- Nosebleeds
- Whistling
- Nasal discomfort
- Empty nose sensation
- Ability to clear secretions
Summary: Posterior perforations rarely need treatment. Anterior, symptomatic perforations are managed stepwise - stop the cause, then saline/moisture care, then a septal button if conservative care fails, then surgical repair using bilateral mucosal advancement flaps with an interposition fascia graft via an open rhinoplasty approach for the best outcomes.
This is a shared conversation. Sign in to Orris to start your own chat.