osteology and muscle attachment of hip bone and its introduction. clinicals if present too, same for the femur bone. for ms1 level, so if mnemonics present do share
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Excellent! I now have all the content I need. Let me compile a comprehensive, MS1-level response.
Hip Bone and Femur - Osteology, Muscle Attachments & Clinicals
Sources: Gray's Anatomy for Students; THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
PART 1: THE HIP BONE (Os Coxae / Innominate Bone)
Introduction
The hip bone (os coxae) is a large, irregular flat bone that forms the lateral wall of the pelvis. It is made of three components that fuse together around puberty:
| Component | Position |
|---|---|
| Ilium | Superior (largest part) |
| Ischium | Posteroinferior |
| Pubis | Anteroinferior |
All three meet at the acetabulum - the cup-shaped socket for the femoral head.
- Ilium = 2/5 of acetabulum
- Ischium = 2/5 of acetabulum
- Pubis = 1/5 of acetabulum
Mnemonic for acetabulum contributions: "2-2-1" - Ilium Ischium Pubis (IIP)
Fusion occurs at the triradiate (Y-shaped) cartilage, completing between ages 14-16.
The two hip bones articulate:
- Anteriorly with each other at the pubic symphysis (fibrocartilaginous)
- Posteriorly with the sacrum at the sacroiliac joints
This creates the pelvic ring.
Medial & Lateral Views of the Hip Bone
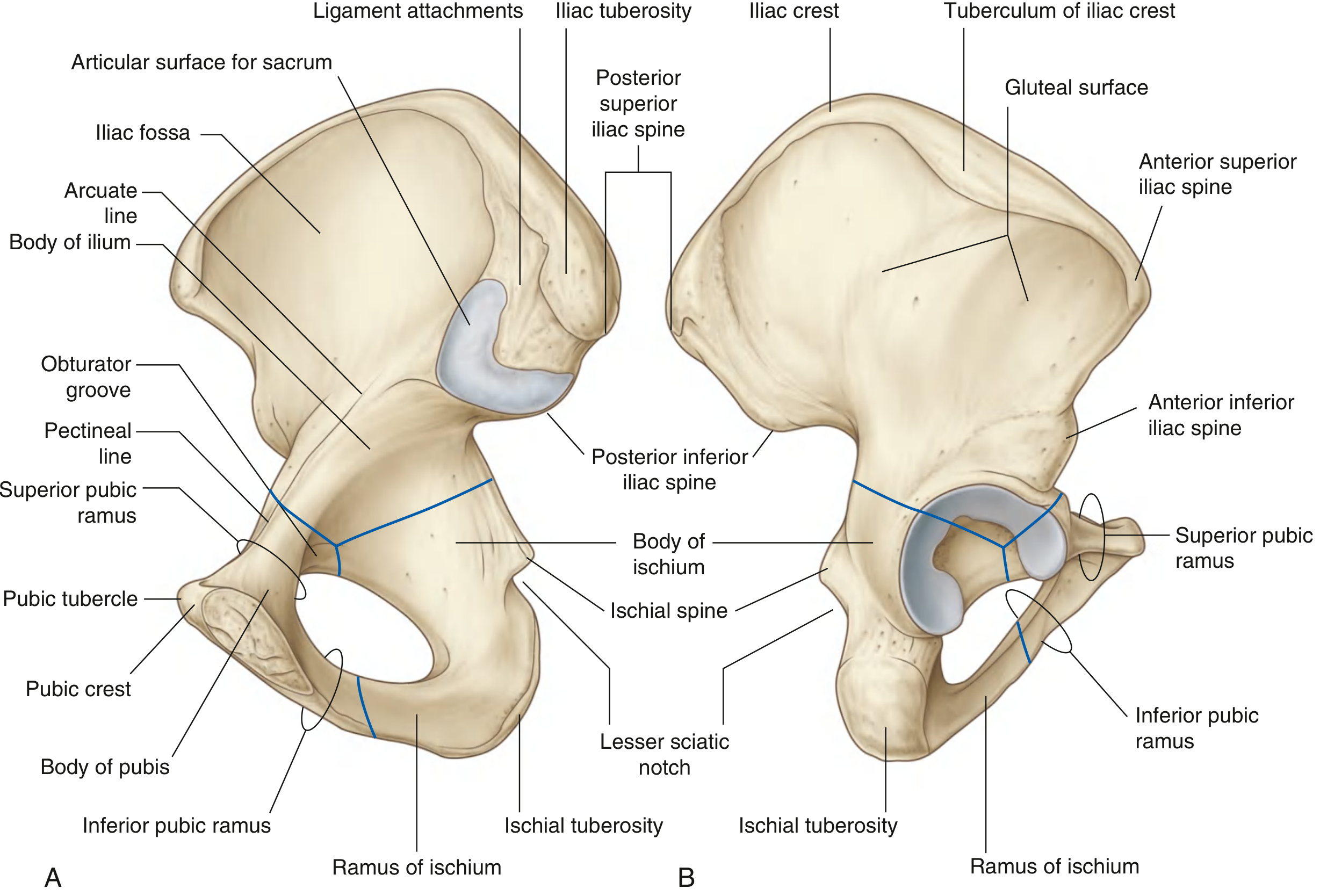
1. ILIUM
Osteology
The ilium is the most superior component. It is divided into:
Upper part (Ala/Wing): flat, fan-shaped - provides muscle attachment and forms the false pelvis
Lower part (Body): contributes to the acetabulum and true pelvis
These two parts are separated by the arcuate line (medially), which forms part of the linea terminalis and pelvic brim.
Key Features:
| Feature | Description |
|---|---|
| Iliac crest | Entire superior thickened border; runs ASIS → PSIS |
| ASIS (Anterior Superior Iliac Spine) | Anterior end of crest |
| AIIS (Anterior Inferior Iliac Spine) | Below ASIS on anterior margin |
| PSIS (Posterior Superior Iliac Spine) | Posterior end of crest |
| PIIS (Posterior Inferior Iliac Spine) | Below PSIS; above greater sciatic notch |
| Iliac fossa | Concave anteromedial surface; lodges iliacus muscle |
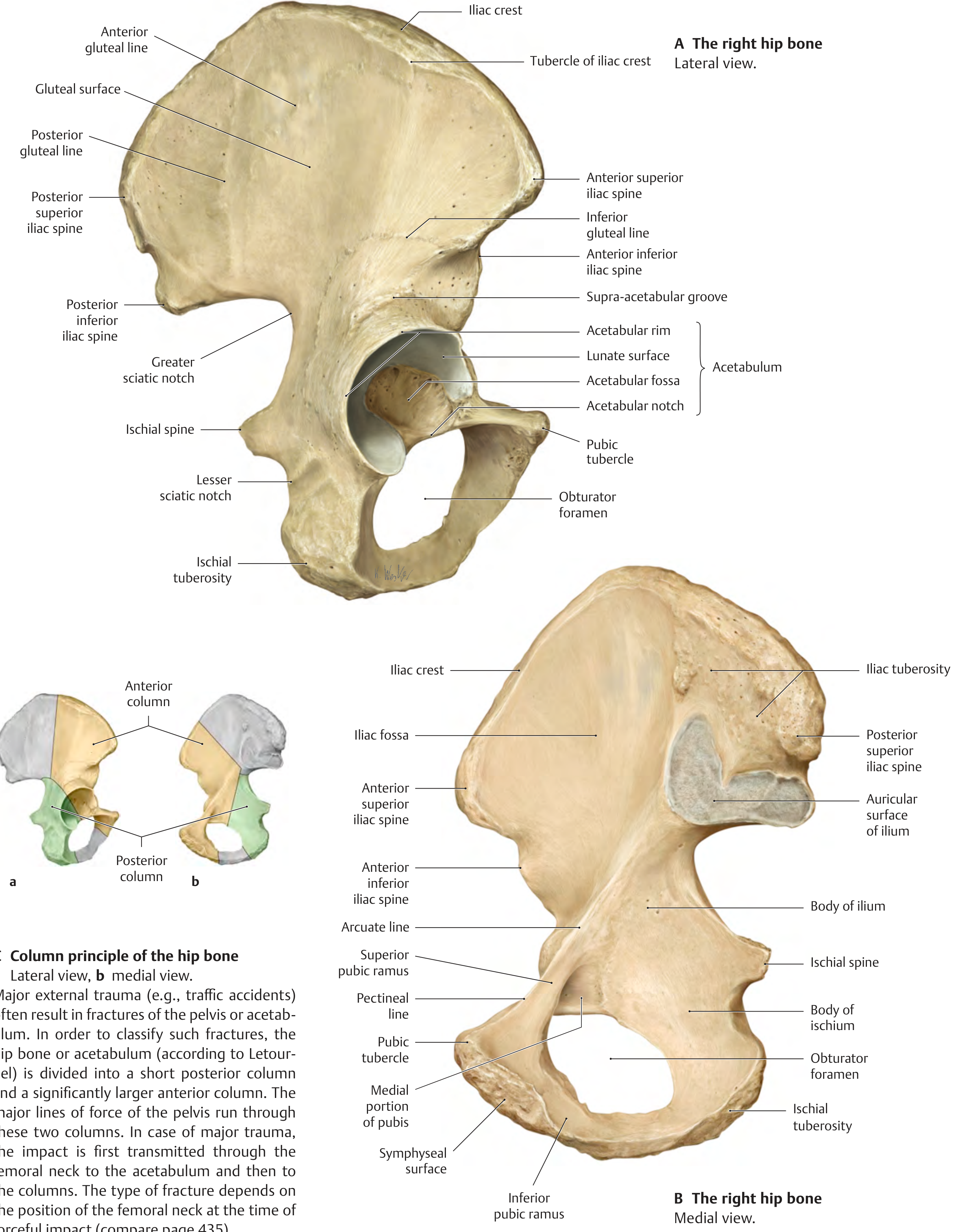
| Gluteal surface | External/lateral surface marked by 3 gluteal lines |
| Auricular surface | Ear-shaped facet for sacroiliac joint |
| Iliac tuberosity | Rough area posterior to auricular surface for SI ligaments |
| Tuberculum of iliac crest | Prominent projection ~5 cm behind ASIS |
Three Gluteal Lines (on gluteal surface - lateral view):
Mnemonic: "PAI" from above downward - Posterior, Anterior, Inferior gluteal lines
| Gluteal Line | Position | Between the lines |
|---|---|---|
| Posterior gluteal line | Most posterior | Above = no muscle |
| Anterior gluteal line | Middle | Gluteus medius attaches |
| Inferior gluteal line | Most inferior (near acetabulum) | Gluteus minimus attaches |
Muscle Attachments on Ilium
| Site | Muscle/Structure |
|---|---|
| Iliac fossa | Iliacus (origin) |
| Iliac crest | External oblique, Internal oblique, Transversus abdominis, Latissimus dorsi, Quadratus lumborum |
| ASIS | Sartorius (origin), Tensor fasciae latae (origin), Inguinal ligament |
| AIIS | Rectus femoris - straight head (origin), Iliofemoral ligament |
| Between gluteal lines | Gluteus maximus (posterior to posterior gluteal line), Gluteus medius (between posterior and anterior lines), Gluteus minimus (between anterior and inferior lines) |
2. ISCHIUM
Osteology
The ischium is posteroinferior. It has:
- Body: projects superiorly; joins ilium and superior pubic ramus at acetabulum
- Ramus: projects anteriorly to meet inferior pubic ramus (together = ischiopubic ramus)
| Feature | Description |
|---|---|
| Ischial spine | Pointed projection on posterior border; separates greater and lesser sciatic notches |
| Ischial tuberosity | Large roughened area inferoposteriorly - "sit bone"; weight-bearing when seated |
| Greater sciatic notch | Above ischial spine; converted to greater sciatic foramen by sacrospinous ligament |
| Lesser sciatic notch | Below ischial spine; converted to lesser sciatic foramen |
| Obturator foramen | Large foramen formed between ischium and pubis |
Muscle Attachments on Ischium
| Site | Muscle |
|---|---|
| Ischial tuberosity | Hamstrings origin: Semitendinosus, Semimembranosus, Long head of Biceps femoris; also Adductor magnus (posterior part) |
| Ischial spine | Gemellus superior (origin); Coccygeus and levator ani (insertion) |
| Ramus of ischium | Obturator externus, Adductor magnus (anterior fibers), Gracilis, Adductor brevis, Gemellus inferior (from ischial tuberosity) |
Mnemonic for hamstrings origin at ischial tuberosity: "Semi-Semi-Bi" (Semitendinosus, Semimembranosus, Biceps femoris long head)
3. PUBIS
Osteology
The pubis is anteroinferior. It has:
- Body: flattened, articulates with contralateral pubis at pubic symphysis
- Superior pubic ramus: projects posterolaterally to acetabulum
- Inferior pubic ramus: joins ramus of ischium
| Feature | Description |
|---|---|
| Pubic crest | Rounded ridge on superior surface of body; ends as pubic tubercle |
| Pubic tubercle | Prominent protuberance at lateral end of pubic crest - key landmark |
| Pecten pubis (pectineal line) | Sharp superior edge of superior ramus; part of linea terminalis |
| Obturator groove | On inferior surface of superior ramus; forms upper margin of obturator canal |
| Symphyseal surface | Medial surface articulating at pubic symphysis |
Muscle Attachments on Pubis
| Site | Muscle |
|---|---|
| Pubic crest and symphysis | Rectus abdominis (origin) |
| Pectineal line (pecten pubis) | Pectineus (origin) |
| Body of pubis | Adductor longus, Gracilis (origin) |
| Inferior pubic ramus | Adductor brevis, Adductor magnus (anterior fibers), Gracilis, Obturator externus |
ACETABULUM
- Cup-shaped socket on lateral surface of hip bone for femoral head
- Articular surface = lunate surface (horseshoe-shaped, covered with hyaline cartilage)
- Non-articular center = acetabular fossa (contains fat pad and ligamentum teres)
- Acetabular notch: gap at inferior aspect; completed by transverse acetabular ligament
CLINICAL NOTES - HIP BONE
1. Bone Marrow Biopsy
The iliac crest is the standard site for bone marrow biopsy (posterior superior iliac spine region). It is superficial, easily palpable, and contains abundant red marrow. Used in leukemia staging, aplastic anemia assessment, and myeloma diagnosis.
2. Avulsion Fractures
Common in young athletes (before fusion of apophyses):
- ASIS avulsion - from sudden sartorius or TFL pull (sprinting)
- AIIS avulsion - from sudden rectus femoris pull (kicking)
- Ischial tuberosity avulsion - hamstring pull (hurdlers, gymnasts)
Mnemonic: ASIS = Sartorius, AIIS = rectus femoris (remembers as "A before I" = sartorius before rectus)
3. Pelvic Fractures
The hip bone is divided into anterior column (iliopubic) and posterior column (ilioischial). Major trauma (e.g., RTA) transmits force through femoral neck to acetabulum then to these columns. Classification: Letournel system.
4. Sciatic Nerve in Greater Sciatic Foramen
The piriformis muscle divides the greater sciatic foramen:
- Above piriformis: superior gluteal nerve and vessels
- Below piriformis: sciatic nerve, inferior gluteal nerve and vessels, pudendal nerve, posterior femoral cutaneous nerve, nerve to obturator internus, nerve to quadratus femoris
Mnemonic for structures below piriformis: "2 Ischial Nerves Painfully Pass Quite Often" (Inferior gluteal, Sciatic, Nerve to obturator internus, Posterior femoral cutaneous, Pudendal, Quadratus femoris nerve, Obturator internus nerve)
5. Sacroiliac Joint Disease
HLA-B27-associated conditions (seronegative spondyloarthropathies) target the SI joints: ankylosing spondylitis, psoriatic arthritis, reactive arthritis, IBD-associated arthritis. Also undergo degenerative changes with aging.
6. Sex Differences of the Pelvis (Important for MS1 exams)
| Feature | Female | Male |
|---|---|---|
| Pelvic inlet shape | Circular/oval | Heart-shaped |
| Pubic arch angle | 80-85° (wider) | 50-60° (narrower) |
| Ischial spines | Less projected medially | More projected medially |
| Overall build | Wider, shallower | Narrower, deeper |
Mnemonic: Female = "wide and round" for childbirth; Male = "narrow and heart-shaped"
PART 2: THE FEMUR
Introduction
The femur is the longest, strongest, and heaviest bone in the human body. It is the bone of the thigh, articulating:
- Proximally with the hip bone at the hip joint (ball-and-socket)
- Distally with the tibia and patella at the knee joint
Full Femur Diagram (Anterior and Posterior)
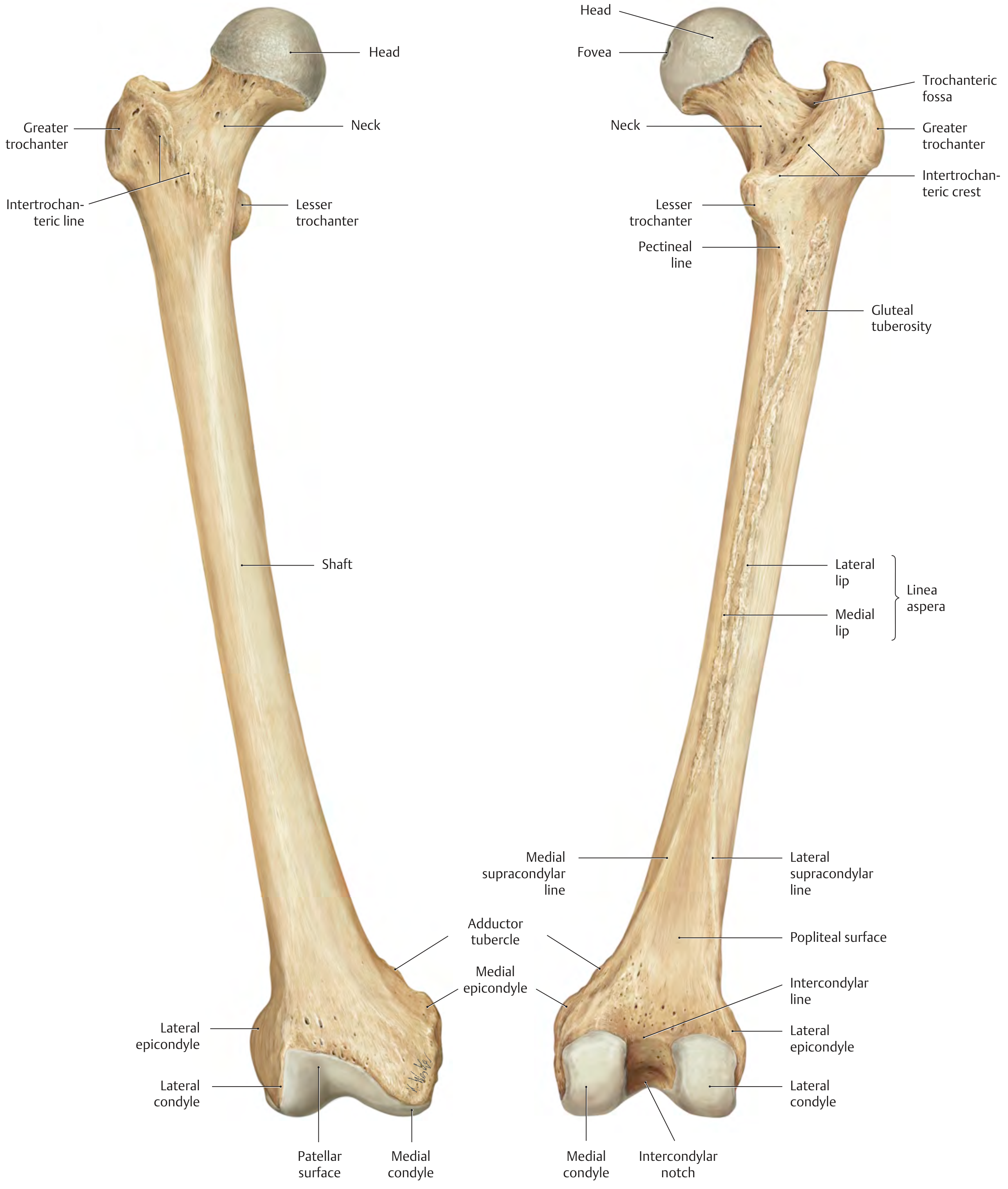
Osteology of the Femur
Proximal End
| Feature | Description |
|---|---|
| Head | 2/3 of a sphere; covered with hyaline cartilage (except fovea) |
| Fovea capitis | Small pit on head; attachment of ligamentum teres (carries artery to head) |
| Neck | Connects head to shaft at ~126° (femoral neck angle/CCD angle) in adults; ~150° at birth |
| Greater trochanter | Large lateral projection at junction of neck and shaft; palpable |
| Lesser trochanter | Small medial projection below neck |
| Intertrochanteric line | Ridge on anterior surface connecting the two trochanters |
| Intertrochanteric crest | Prominent ridge on posterior surface connecting trochanters |
| Trochanteric fossa | Depression on medial surface of greater trochanter |
| Quadrate tubercle | On intertrochanteric crest |
| Pectineal line | Short ridge below lesser trochanter posteriorly |
Shaft (Diaphysis)
| Feature | Description |
|---|---|
| Linea aspera | Prominent vertical ridge on posterior surface of shaft; has medial and lateral lips |
| Gluteal tuberosity | Superolateral extension of lateral lip of linea aspera |
| Pectineal line of femur | Superoposterior continuation of medial lip |
| Medial supracondylar line | Distal extension of medial lip |
| Lateral supracondylar line | Distal extension of lateral lip |
| Popliteal surface | Triangular flat area between supracondylar lines posteriorly (floor of popliteal fossa) |
Distal End
| Feature | Description |
|---|---|
| Medial condyle | Larger, projects more inferiorly |
| Lateral condyle | Slightly smaller |
| Intercondylar notch (fossa) | Deep groove between condyles posteriorly; contains cruciate ligaments |
| Patellar surface (trochlea) | Anterior smooth groove between condyles; articulates with patella |
| Medial epicondyle | Bony prominence above medial condyle |
| Lateral epicondyle | Bony prominence above lateral condyle |
| Adductor tubercle | Small projection just above medial epicondyle; attachment of adductor magnus |
| Intercondylar line | Ridge at top of intercondylar notch posteriorly |
Femoral Angles - Very Commonly Tested
1. Neck-Shaft Angle (CCD / Inclination angle)
- Normal adult: 126°
- Newborn: ~150° (decreases through childhood)
- Coxa valga: angle > 135° (long leg appearance)
- Coxa vara: angle < 120° (shortened leg, limping gait)
2. Angle of Anteversion (Torsion angle)
- Normal adult: 12° (neck angled forward relative to condylar axis)
- Newborn: 30-40°, decreases to adult value by end of 2nd decade
- Increased anteversion (coxa anteverta): toeing-in gait, limited external rotation
- Decreased/retroversion (coxa retroverta): toeing-out gait
Mnemonic: "126 and 12" - neck-shaft angle = 126°, anteversion = 12°
Muscle Attachments on Femur
Proximal Femur
| Site | Muscle | Action |
|---|---|---|
| Greater trochanter (lateral surface) | Gluteus medius and minimus (insertion) | Abduction |
| Trochanteric fossa (medial) | Obturator internus + both gemelli (insertion) | Lateral rotation |
| Intertrochanteric line (anterior) | Iliofemoral ligament (attachment) | - |
| Lesser trochanter | Iliopsoas = iliacus + psoas major (insertion) | Flexion |
| Quadrate tubercle (intertrochanteric crest) | Quadratus femoris (insertion) | Lateral rotation |
| Below greater trochanter (posterior) | Gluteus maximus upper fibers → iliotibial tract; lower fibers → gluteal tuberosity | Extension |
| Pectineal line of femur | Pectineus (insertion) | Adduction + flexion |
Shaft - Linea Aspera
| Lip / Site | Muscle (Insertion unless stated) |
|---|---|
| Medial lip (entire length) | Adductor longus, Adductor brevis, Adductor magnus (middle fibers) |
| Lateral lip | Vastus lateralis (origin), Short head of Biceps femoris (origin) |
| Between medial and lateral lips | Vastus intermedius (origin), Vastus medialis (origin along medial lip) |
| Lateral lip superiorly | Vastus lateralis and Gluteus maximus (via IT band/gluteal tuberosity) |
Mnemonic for linea aspera attachments: "VAB" - Vasti (origins), Adductors (insertions), Biceps femoris short head (origin)
Distal Femur
| Site | Muscle/Structure |
|---|---|
| Adductor tubercle | Adductor magnus - tendinous/vertical fibers (insertion) |
| Medial epicondyle | Medial collateral ligament, Medial head of gastrocnemius (origin) |
| Lateral epicondyle | Lateral collateral ligament, Lateral head of gastrocnemius (origin), Popliteus (origin) |
| Intercondylar notch | ACL (from lateral condyle), PCL (from medial condyle) |
CLINICAL NOTES - FEMUR
1. Femoral Neck Fractures (Hip Fractures)
- Very common in elderly osteoporotic women (after fall)
- Subcapital fractures cut off blood supply to femoral head → avascular necrosis (AVN)
- Blood supply to femoral head: medial circumflex femoral artery (main) → retinacular vessels ascending along neck; artery of ligamentum teres (minor contribution, mainly in children)
- Intertrochanteric fractures: extracapsular, better blood supply, treated with nail-plate fixation
- Subcapital/intracapsular: treated with hemiarthroplasty or total hip replacement
Mnemonic: "Young people get fixed (ORIF), Old people get replaced (hemiarthroplasty)"
2. Coxa Vara vs Coxa Valga
| Coxa Vara | Coxa Valga | |
|---|---|---|
| Neck-shaft angle | <120° | >135° |
| Leg length | Shortened | Lengthened |
| Gait | Trendelenburg/limping | - |
| Common cause | Rickets, Paget's disease, fracture | Cerebral palsy, non-weight-bearing |
3. Femoral Anteversion Abnormalities
- Increased anteversion: toeing-in gait ("pigeon-toed") - common in children (often resolves)
- Retroversion: toeing-out gait - associated with slipped capital femoral epiphysis (SCFE)
4. Slipped Capital Femoral Epiphysis (SCFE)
- Occurs in obese adolescents; the femoral head slips posteriorly/inferiorly off the neck
- Results in retroversion appearance
- Bilateral in 25% of cases
5. Perthes Disease (Legg-Calvé-Perthes)
- AVN of femoral head in children (ages 4-8, boys more than girls)
- Results in coxa vara deformity
6. Linea Aspera and Thigh Muscles
The linea aspera is the main "muscle highway" of the posterior femoral shaft. All three adductors insert here; the vastus group originates here. This ridge is often tested in the context of adductor compartment surgery and femoral fracture patterns.
7. Intercondylar Notch and Ligaments
The ACL originates from the posterior aspect of the medial surface of the lateral femoral condyle. The PCL originates from the anterior aspect of the lateral surface of the medial femoral condyle. Remembering this is essential for knee injury MCQs.
Mnemonic: ACL = "Lateral condyle to Anterior tibial spine"; PCL = "Medial condyle to Posterior tibial spine" → Both cross: L→A and M→P
Summary Mnemonics Sheet
| Topic | Mnemonic |
|---|---|
| Acetabulum contributions (2-2-1) | "IIP: Ilium Ischium Pubis" |
| Gluteal lines order (top to bottom) | "PAI" - Posterior, Anterior, Inferior |
| ASIS attachment | Sartorius + TFL + Inguinal ligament |
| AIIS attachment | Rectus femoris straight head |
| Ischial tuberosity (hamstrings) | "Semi-Semi-Bi" |
| Below piriformis structures | "2 Ischial Nerves Painfully Pass Quite Often" |
| Femoral angles | "126 and 12" (neck-shaft and anteversion) |
| Linea aspera | "VAB" (Vasti, Adductors, Biceps short head) |
| Hip fracture management | "Young = Fixed, Old = Replaced" |
| Female vs Male pelvis | Female = "Wide and Round" |
Gray's Anatomy for Students, Chapter 5 (Lower Limb) | THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System, 1.3-1.5
This is a shared conversation. Sign in to Orris to start your own chat.