2 marks questions 1. Enlist nuclei present in hypothalamus 2.Write a short note on major salivary glands 3. When growth hormone levels are low or high, what can we expect to happen? 4. Draw a labelled diagram of sperm 5. Write a brief note on estrogen 6. Write a short note on spermatogenesis 7. What is BMR? Name the factors affecting it. 8. What is function of pineal gland and thymus
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I now have all the information needed to answer all 8 questions comprehensively. Let me compile the full answers.
2-Mark Question Answers
1. Nuclei Present in the Hypothalamus
The hypothalamus is divided from anterior to posterior into four regions, each containing distinct nuclei:
Anterior (Supraoptic) Region:
- Supraoptic nucleus (produces ADH/vasopressin)
- Paraventricular nucleus (produces ADH and oxytocin)
- Anterior nucleus (thermoregulation - heat dissipation)
- Preoptic nucleus (temperature, sexual behavior)
Middle (Tuberal/Infundibular) Region:
- Ventromedial nucleus (satiety center)
- Dorsomedial nucleus (feeding behavior, aggression)
- Arcuate nucleus (releasing hormones - GHRH, dopamine)
- Lateral hypothalamic nucleus (hunger center)
Posterior (Mammillary) Region:
- Posterior nucleus (heat conservation, consciousness)
- Mammillary nuclei - lateral and medial (relay hippocampal input via fornix to anterior thalamic nuclei; involved in memory)
- Supramammillary nucleus
The supraoptic and paraventricular nuclei are particularly important - they synthesize ADH and oxytocin, which are released from the posterior pituitary. (Guyton and Hall Textbook of Medical Physiology; Neuroanatomy through Clinical Cases 3rd Edition)
2. Major Salivary Glands
There are three pairs of major salivary glands:
1. Parotid Glands
- Largest salivary glands; located anterior to the ear, overlying the masseter muscle
- Purely serous secretion (watery, enzyme-rich saliva)
- Duct: Stensen's duct opens into the oral cavity opposite the upper 2nd molar
- Contains the facial nerve (CN VII) running through it
- Contributes ~25% of total saliva
2. Submandibular Glands
- Located in the floor of the mouth, in the submandibular triangle
- Mixed secretion (predominantly serous, some mucous)
- Duct: Wharton's duct opens at the sublingual caruncle beneath the tongue
- Contributes ~70% of total resting saliva
- CT attenuation is similar to muscle (more predictable than parotid)
3. Sublingual Glands
- Smallest of the three; lie in the floor of the mouth beneath the tongue
- Predominantly mucous secretion
- Multiple small ducts (Rivinus' ducts), some opening via a common duct (Bartholin's duct) into Wharton's duct
- Contributes ~5% of total saliva
Functions of saliva: lubrication, initial digestion of starch (amylase), antibacterial protection (IgA, lysozyme), taste, speech, and dental protection.
(Cummings Otolaryngology Head and Neck Surgery)
3. When Growth Hormone Levels Are Low or High
When GH is LOW (Deficiency):
- In childhood: Growth failure - children are of normal size at birth but progressively fall behind peers. Results in pituitary dwarfism (adult height ~1.0 m in extreme cases).
- In adulthood: Decreased lean body mass, increased body fat, possibly reduced sense of well-being and vigor.
- GH-deficient adults respond to recombinant GH replacement with improved body composition.
When GH is HIGH (Excess):
- In childhood (before epiphyseal plate closure): Excessive linear bone growth → Gigantism (adult heights exceeding 2.7 m in extreme cases).
- In adulthood (after epiphyseal plate closure): Long bone elongation is not possible; instead, Acromegaly develops:
- Progressive thickening of bones and soft tissues of the head, hands, and feet
- Growth of skin, muscle, heart, liver, and GI tract
- Causes joint deformity, hypertension, pulmonary insufficiency, and heart failure if untreated
- Shorter life expectancy
GH is produced by somatotrophs in the anterior pituitary and acts mainly via IGF-1 (insulin-like growth factor 1) produced by the liver. (Medical Physiology, Boron & Boulpaep)
4. Labelled Diagram of Sperm
Here is a labelled diagram of a mature spermatozoon from the textbook:
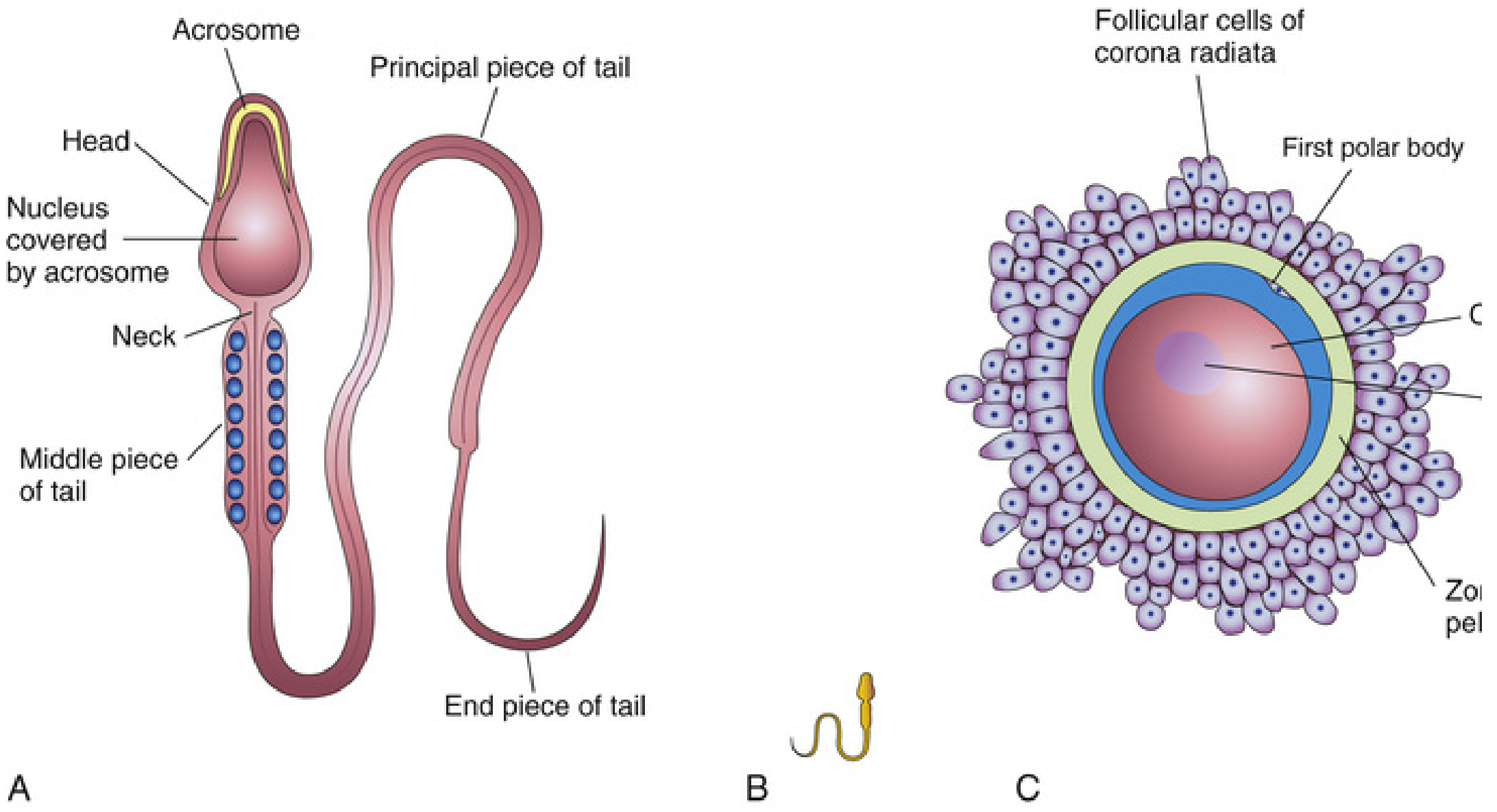
Key labels for your answer:
| Part | Details |
|---|---|
| Head | Contains the haploid nucleus; covered anteriorly by the acrosome |
| Acrosome | Cap-like saccular organelle over anterior 2/3 of head; contains hydrolytic enzymes (hyaluronidase, acrosin) that help penetrate corona radiata and zona pellucida during fertilization |
| Neck | Junction between head and tail; contains centrioles |
| Middle piece of tail | Contains mitochondria arranged in a spiral - provides ATP for flagellar movement |
| Principal piece of tail | Longest segment; contains the axoneme (9+2 microtubule arrangement) |
| End piece of tail | Short terminal segment; no fibrous sheath |
(The Developing Human: Clinically Oriented Embryology)
5. Brief Note on Estrogen
Estrogen refers to a group of steroid hormones. The three main types are estradiol (E2) (most potent, predominant in reproductive years), estriol (E3) (predominant in pregnancy), and estrone (E1) (predominant post-menopause).
Sources:
- Primarily produced by granulosa cells of ovarian follicles (via aromatization of androgens)
- Also produced by the corpus luteum, adrenal cortex, placenta (during pregnancy), and adipose tissue
- In males: small amounts from testicular Sertoli cells and peripheral aromatization
Actions:
- Reproductive tract: Development and maintenance of female secondary sex characteristics; growth of uterus, vagina, fallopian tubes, and breast tissue
- Uterus: Proliferation of endometrium (proliferative phase); increases uterine contractility
- Cervix: Increases cervical mucus production and makes it thin/watery (favors sperm entry)
- Bone: Promotes epiphyseal closure; protects against bone resorption - estrogen deficiency at menopause leads to osteoporosis
- Cardiovascular: Favorable lipid profile (raises HDL, lowers LDL)
- CNS: Affects mood, cognition, and thermoregulation (loss causes hot flushes at menopause)
- Feedback: At low levels - negative feedback on FSH/LH; at high levels (pre-ovulatory surge) - positive feedback triggering the LH surge
(Goodman & Gilman's The Pharmacological Basis of Therapeutics; Goldman-Cecil Medicine)
6. Short Note on Spermatogenesis
Spermatogenesis is the process by which spermatogonia (primordial germ cells) are transformed into mature spermatozoa. It begins at puberty, occurs in the seminiferous tubules of the testes, and is regulated by testosterone (acting via androgen receptors on Sertoli cells) and FSH.
Stages:
-
Mitotic phase: Spermatogonia undergo repeated mitotic divisions to maintain the germ cell pool. Some differentiate into primary spermatocytes (diploid, 2n), the largest cells in the seminiferous tubules.
-
First meiotic division: Each primary spermatocyte undergoes meiosis I → two secondary spermatocytes (haploid, 1n, but each chromosome still consists of 2 chromatids).
-
Second meiotic division: Each secondary spermatocyte undergoes meiosis II → four spermatids (haploid, 1n). Each primary spermatocyte ultimately yields 4 spermatids.
-
Spermiogenesis: Spermatids undergo morphological transformation into mature spermatozoa (no further division):
- Acrosome forms from the Golgi apparatus
- Flagellum develops
- Most cytoplasm is shed as residual bodies
- Nucleus condenses
Timeline: The entire process takes approximately 2 months (~64 days).
Supporting cells:
- Sertoli cells: Nurture developing germ cells; blood-testis barrier; secrete inhibin and androgen-binding protein
- Leydig (interstitial) cells: Produce testosterone (essential for spermatogenesis)
After spermiogenesis, sperms enter the seminiferous tubule lumen, then pass to the epididymis where they mature and gain motility before storage and eventual transport via the vas deferens.
(The Developing Human: Clinically Oriented Embryology; Costanzo Physiology 7th Edition)
7. BMR - Definition and Factors Affecting It
Basal Metabolic Rate (BMR) is defined as the rate of energy expenditure at complete rest, in a post-absorptive state (12-14 hours after eating), in a thermoneutral environment. It represents the minimum energy required to maintain basic vital functions - circulation, respiration, cellular maintenance, and thermoregulation. BMR is measured in kcal/day or kcal/hr/m² of body surface area.
Factors Affecting BMR:
| Factor | Effect |
|---|---|
| Body surface area / size | Larger body = higher BMR |
| Age | BMR decreases with age (loss of lean mass) |
| Sex | Males have higher BMR than females (more lean muscle mass) |
| Thyroid hormones (T3/T4) | Most powerful regulator - hyperthyroidism raises BMR; hypothyroidism lowers it |
| Body composition | More lean muscle mass = higher BMR; fat tissue is metabolically less active |
| Temperature | Fever increases BMR (~7-13% per 1°C rise); cold environment increases BMR |
| Nutritional state | Starvation and prolonged fasting lower BMR |
| Growth hormone & testosterone | Increase BMR by promoting anabolic metabolism |
| Sympathetic nervous system / catecholamines | Epinephrine/norepinephrine increase BMR |
| Pregnancy & lactation | Increase BMR |
| Disease states | Infection, burns, trauma raise BMR; malnutrition lowers it |
(Goldman-Cecil Medicine)
8. Functions of the Pineal Gland and Thymus
Pineal Gland
The pineal gland is a small neuroendocrine structure in the epithalamus (posterior diencephalon). Its principal secretory product is melatonin, synthesized from tryptophan via serotonin.
Functions:
- Circadian rhythm regulation: Melatonin production increases in darkness and is suppressed by light (via the retinohypothalamic tract → suprachiasmatic nucleus → superior cervical ganglion → pineal gland). This creates a daily rhythmic signal that helps entrain the sleep-wake cycle.
- Seasonal rhythm and reproduction: In many animals, melatonin signals day length and regulates seasonal reproductive cycles. In humans, the role is less prominent but similar mechanisms exist.
- Onset of puberty: The pineal is thought to inhibit the hypothalamic-pituitary-gonadal axis prior to puberty; declining melatonin influence may contribute to puberty initiation.
- Antioxidant: Melatonin has free-radical scavenging properties.
Pineal calcification (corpora arenacea / "brain sand") occurs commonly with age and is used as a midline reference in skull X-rays.
Thymus
The thymus is a bilobed lymphoid organ located in the anterior mediastinum, most active during childhood and involutes after puberty.
Functions:
- T-lymphocyte maturation: The primary function. Immature T-cell precursors (thymocytes) migrate from the bone marrow to the thymus, where they mature and acquire antigen specificity in the thymic cortex, then undergo positive selection (recognize self-MHC) and negative selection (eliminate self-reactive clones) in the medulla.
- Central tolerance: Medullary thymic epithelial cells express self-antigens (via AIRE gene), ensuring autoreactive T-cells are deleted - preventing autoimmunity.
- Endocrine function: Produces thymic hormones - thymosin, thymopoietin, thymulin - which promote T-cell differentiation and maturation both within and outside the thymus.
- Immunological development: Produces a pool of naive T-cells (CD4+ helper and CD8+ cytotoxic) that seed peripheral lymphoid organs for lifelong immune surveillance.
DiGeorge syndrome (22q11 deletion) results in thymic aplasia with deficient T-cell immunity, illustrating the organ's importance.
(Junqueira's Basic Histology; Histology: A Text and Atlas; Ganong's Review of Medical Physiology)
This is a shared conversation. Sign in to Orris to start your own chat.