Write 8 Eustachian tube function test names. (6 Marks) (VALMED)*** *Draw labelled diagram of Middle ear cleft and enumerate function of Eustachian tube. (6 Marks) (GMC)
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have all the information needed. Let me compile a comprehensive answer.
Part 1: Eustachian Tube Function Tests (8 Tests)
The following are the recognized tests for assessing Eustachian tube (ET) function, sourced from standard ENT texts:
| # | Test Name | Brief Description |
|---|---|---|
| 1 | Valsalva Maneuver | Patient forcibly exhales against a closed nose and mouth; positive pressure generated (~20-40 mm Hg) forces air up the ET into the middle ear. Observed by outward movement of the TM on otoscopy. |
| 2 | Toynbee Test | Patient swallows with the nose and mouth closed; this creates negative nasopharyngeal pressure. Observed by inward movement of the TM. Used to assess ET function under negative pressure. |
| 3 | Politzer Test (Politzerization) | A Politzer bag is placed in one nostril while the patient swallows or says "K." Positive pressure delivered into the nasopharynx opens the ET. Movement of the TM is observed with a pneumatic otoscope. |
| 4 | Eustachian Tube Catheterization | A metal catheter is passed along the floor of the nose into the nasopharyngeal orifice of the ET; air or fluid is insufflated and a stethoscope placed over the ear to detect air passage. One of the oldest tests (18th century). |
| 5 | Forced Response Test | Used in patients with a TM perforation or patent grommet. A tympanometry probe + air pump is placed in the ear canal; increasing pressure is applied until the ET is forced open. Measures opening pressure and resistance. |
| 6 | Inflation-Deflation Test | Uses a tympanometry probe placed in the ear canal to record pressure changes while the patient swallows. Both inflation (positive) and deflation (negative) phases can be assessed sequentially to evaluate ET opening. |
| 7 | Tubomanometry | A pressure probe is placed in the nasopharynx; gradually increasing pressure is applied while the patient swallows with the mouth closed. The pressure at which the ET opens (abrupt change in ear canal pressure) is recorded as the "opening pressure." |
| 8 | Sonotubometry | A sound probe plays a tone inside the nasal cavity; a microphone in the external auditory canal detects any increase in sound amplitude when the ET opens. A non-invasive, objective method of assessing ET patency. |
Additional tests sometimes listed: nine-step inflation-deflation test, pressure chamber tests, tympanometry (indirect assessment via Type C curve), and Eustachian tube endoscopy.
Sources: Cummings Otolaryngology HNS, Chapter 131 (ET Function Tests section); Scott-Brown's Otorhinolaryngology Vol 2, Chapter 86 (Best Clinical Practice)
Part 2: Middle Ear Cleft - Labelled Diagram + Functions of Eustachian Tube
Middle Ear Cleft - Diagram
Here is a labelled anatomical diagram of the middle ear cleft compartments from Scott-Brown's Otorhinolaryngology (attic view showing ossicles, folds, and spaces):
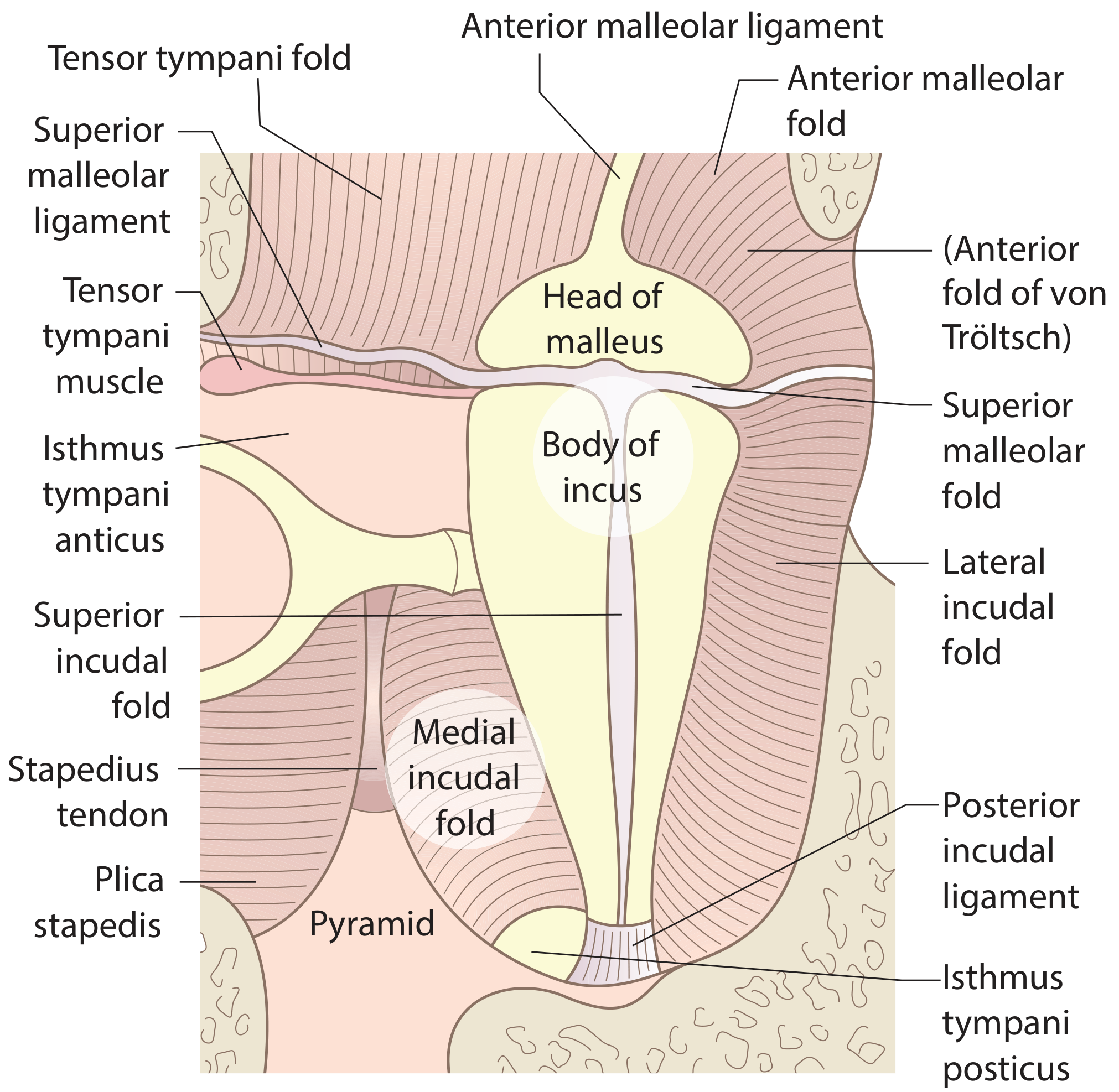
Figure: The attic folds and compartments of the middle ear, showing head of malleus, body of incus, tensor tympani muscle, stapedius tendon, pyramid, Prussak's space components, and folds (anterior fold of von Tröltsch, tensor tympani fold, superior/lateral/medial/posterior incudal folds, plica stapedis). (Scott-Brown's Otorhinolaryngology Vol 2)
Components of the Middle Ear Cleft
The middle ear cleft consists of three communicating air-containing spaces:
- Tympanic cavity - an irregular air-filled space within the temporal bone, bounded laterally by the tympanic membrane and medially by the osseous labyrinth. Contains the ossicular chain (malleus, incus, stapes), middle ear muscles (tensor tympani, stapedius), facial nerve (tympanic segment), and chorda tympani.
- Eustachian tube - connects the tympanic cavity to the nasopharynx (35 mm in adults; 1/3 bony, 2/3 cartilaginous).
- Mastoid air cell system - communicates posteriorly with the tympanic cavity via the aditus ad antrum.
Functions of the Eustachian Tube (6 key functions)
| # | Function | Mechanism |
|---|---|---|
| 1 | Pressure Equalization (Ventilation) | Intermittent opening of the ET during swallowing and yawning allows equilibration of middle ear pressure with ambient atmospheric pressure. This is essential for efficient sound conduction. A pressure of -30 mm Hg sustained for 15 min can produce a middle ear transudate. |
| 2 | Mucociliary Clearance / Drainage | The pseudostratified columnar ciliated epithelium lining the ET drains secretions from the middle ear into the nasopharynx by mucociliary action and gravity. |
| 3 | Protection from Nasopharyngeal Reflux | The ET is normally closed at rest (at the nasopharyngeal end) by the elastic cartilage and mucosal folds, acting as a valve. This prevents ascent of nasopharyngeal secretions, pathogens, and sounds into the middle ear (prevents autophonia). |
| 4 | Protection from Loud Sounds | The resting closed state of the ET prevents transmission of loud sounds directly from the nasopharynx to the middle ear. |
| 5 | Gas Exchange | Bidirectional gas exchange across the ET and middle ear mucosa maintains the partial pressures of O₂, CO₂, and N₂ within the middle ear cleft, preventing progressive negative pressure build-up. |
| 6 | Immunological Defense | The lymphoid tissue within the ET (tonsil of Gerlach) and the mucosa contribute to local immune defense. The mucous layer traps pathogens. |
Opening Mechanism of the ET
- The ET opens actively via the tensor veli palatini (V3 innervation) - the primary dilator muscle acting synergistically with the levator veli palatini (vagus innervation).
- In children, the ET is more horizontal, shorter (17-18 mm at birth vs. 35 mm in adults), and the levator veli palatini is functionally separated, making children more prone to ET dysfunction and otitis media.
- A pressure differential >90 mm Hg "locks" the ET (critical pressure difference), preventing it from opening even with muscle contraction.
Sources: Cummings Otolaryngology HNS (Chapter 131, Physiology section); K.J. Lee's Essential Otolaryngology, Chapter 13; Scott-Brown's Otorhinolaryngology Vol 2, Chapter 46 & 86
This is a shared conversation. Sign in to Orris to start your own chat.