Why methemoglobinemia causes spo2 of 85%
Reading File
Finding Sources
Finding Sources
Searching the Web
methemoglobinemia pulse oximeter SpO2 85% mechanism explanation
Reading File
Reading File
Reading File
Loading Image
Now I have everything needed for a complete, well-sourced answer.
Why Methemoglobinemia Causes a SpO2 of 85%
This is one of the classic "pulse oximetry trap" questions in medicine. The explanation is rooted in the physics of how pulse oximeters work and the unique optical behavior of methemoglobin.
How a Pulse Oximeter Works
A standard pulse oximeter uses two wavelengths of light:
- 660 nm (red light)
- 940 nm (infrared light)
It shines these through a tissue bed (finger, ear) and measures how much of each wavelength is absorbed. The key insight is that oxyhemoglobin (HbO2) and deoxyhemoglobin (Hb) absorb these two wavelengths differently:
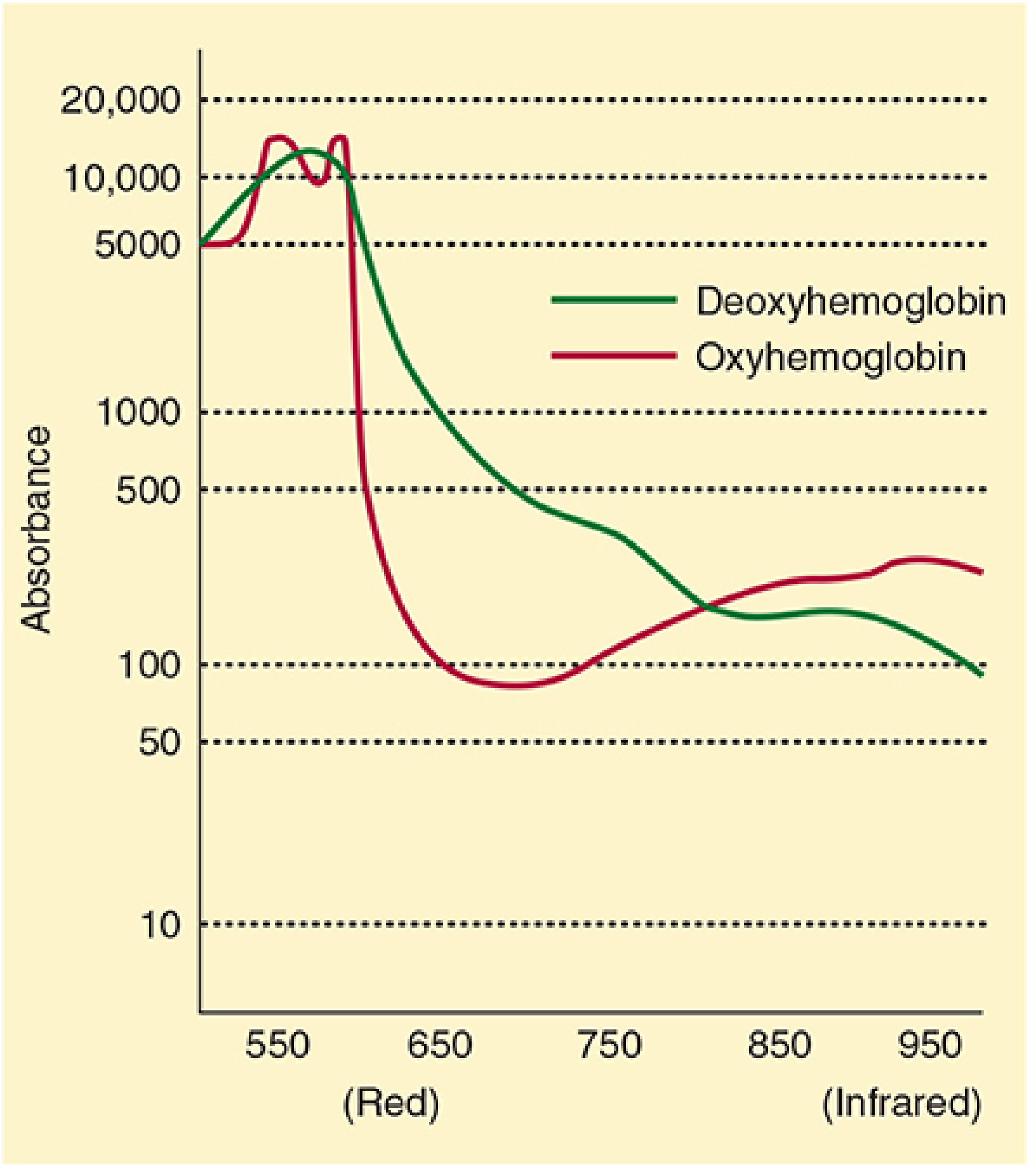
The device computes the ratio R = (Abs 660 nm) / (Abs 940 nm) and uses a built-in calibration curve to convert this ratio into SpO2:
| R ratio | SpO2 reading |
|---|---|
| ~0.4 | ~100% |
| ~1.0 | ~85% |
| ~2.0 | ~0% |
The Key Problem: MetHb Absorbs Equally at Both Wavelengths
Methemoglobin is formed when the iron in hemoglobin is oxidized from Fe²+ to Fe³+. This ferric form cannot carry oxygen. More importantly for pulse oximetry:
Methemoglobin has the same absorption coefficient at both 660 nm and 940 nm.
This means MetHb absorbs red and infrared light equally, producing an absorption ratio (R) of 1:1.
Looking at the calibration curve, a ratio of 1.0 corresponds to exactly 85% SpO2. This is not a coincidence - it is a fixed mathematical consequence of how the oximeter's calibration curve was constructed.
- Morgan & Mikhail's Clinical Anesthesiology, p. 224: "Methemoglobin has the same absorption coefficient at both red and infrared wavelengths. The resulting 1:1 absorption ratio corresponds to a saturation reading of 85%."
The Clinical Consequence: SpO2 Plateaus at ~85%
As MetHb levels rise, the pulse oximeter reading is dragged toward this 85% "attractor value":
- If the true SaO2 > 85% (patient is not critically hypoxic), SpO2 reads falsely low (~85%) - the reading is lower than reality.
- If the true SaO2 < 85% (patient is severely hypoxic), SpO2 reads falsely high (~85%) - dangerously misleading!
- Once MetHb exceeds ~30-35%, the reading plateaus and stays stuck near 85% regardless of how hypoxic the patient actually is.
As noted in Roberts & Hedges' Clinical Procedures in Emergency Medicine: "Large quantities of methemoglobin (>10%) can result in a stable pulse oximetry reading of 85% regardless of the actual SaO2."
Key Diagnostic Clues
| Finding | Explanation |
|---|---|
| SpO2 ~85%, unresponsive to O2 | MetHb acts as optical "noise" fixed at 85% |
| "Saturation gap" (SpO2 ≠ SaO2 from ABG) | ABG calculates saturation from PaO2, ignoring MetHb |
| Normal PaO2 on ABG | Dissolved O2 in plasma is fine; it's hemoglobin that can't carry O2 |
| Chocolate-brown blood | Classic appearance of methemoglobin |
| Cyanosis not responding to supplemental O2 | O2 cannot displace Fe³+ back to Fe²+ |
Rosen's Emergency Medicine: "Consider the diagnosis of methemoglobinemia in any cyanotic patient whose pulse oximetry displays a saturation of 85% to 88% that is unresponsive to oxygen therapy and whose arterial blood appears 'chocolate brown' in color."
Why Standard ABG Can Miss It Too
A standard blood gas analyzer calculates SaO2 from the measured PaO2 using a formula - it assumes all hemoglobin is either oxy or deoxy. It doesn't "see" MetHb. So it may give a falsely normal or near-normal SaO2, creating the saturation gap.
The only accurate test is co-oximetry, which measures four wavelengths (or more) and directly quantifies oxyhemoglobin, deoxyhemoglobin, carboxyhemoglobin, and methemoglobin separately.
Treatment
- Remove the offending agent (dapsone, benzocaine, nitrites, phenazopyridine, etc.)
- Methylene blue 1-2 mg/kg IV - activates NADPH-methemoglobin reductase, which reduces MetHb back to normal Hb. Contraindicated in G6PD deficiency.
- Exchange transfusion for G6PD-deficient patients or those failing methylene blue.
This is a shared conversation. Sign in to Orris to start your own chat.