Cyanocobalamin vs methylcobalamin
Reading File
Finding Sources
Searching PubMed
cyanocobalamin methylcobalamin comparison vitamin B12
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a full comparison of cyanocobalamin vs. methylcobalamin based on authoritative pharmacology and biochemistry textbooks:
Cyanocobalamin vs. Methylcobalamin
1. Chemical Nature
| Feature | Cyanocobalamin | Methylcobalamin |
|---|---|---|
| Ligand on cobalt | Cyanide (CN⁻) | Methyl group (CH₃) |
| Origin | Synthetic / commercial form | Active physiologic coenzyme |
| Stability | High - forms dark red crystals | Less stable, light-sensitive |
| Color | Deep red | Yellow-orange |
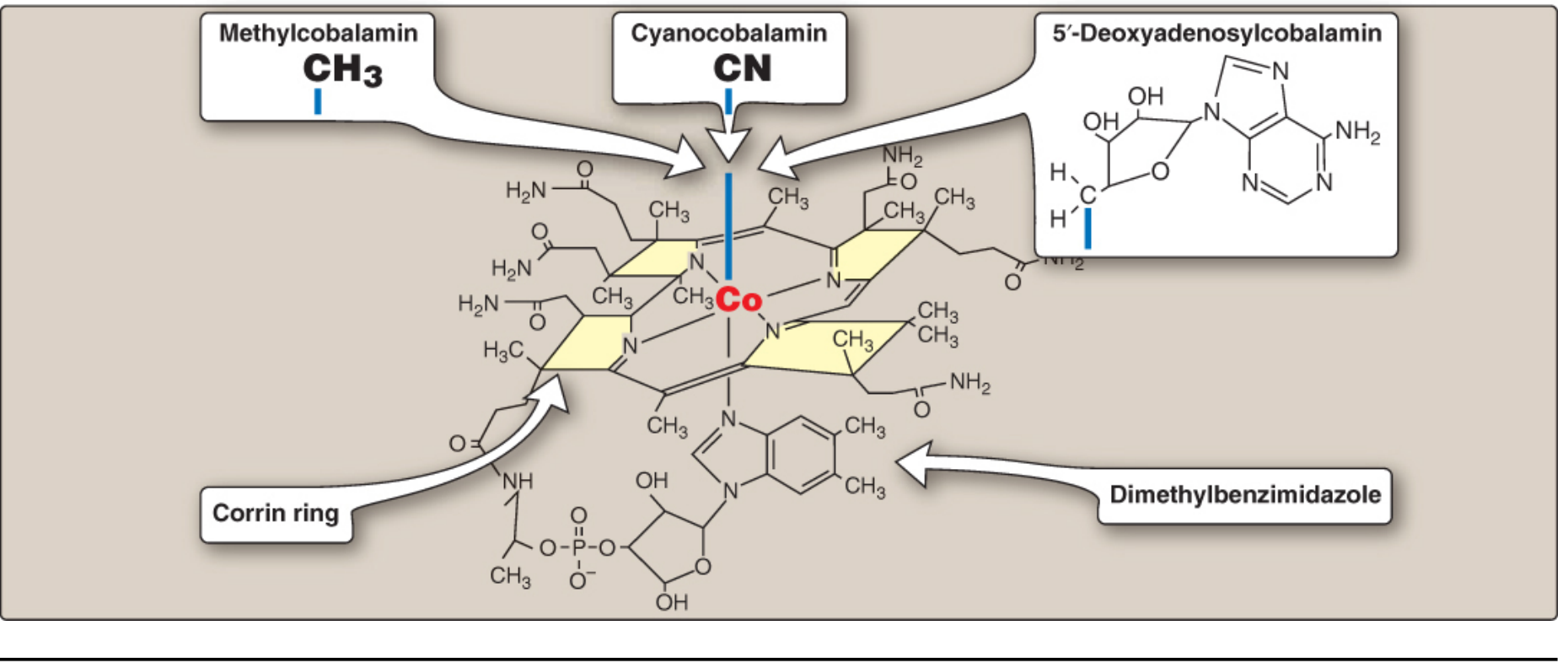
All cobalamins share the same corrin ring with a central cobalt atom. The only difference is the group bound at the 6th coordination site of cobalt. Cyanocobalamin is the synthetic, pharmaceutical-grade form; methylcobalamin is one of the two active coenzyme forms found in human cells (the other being 5'-deoxyadenosylcobalamin). - Biochemistry 8th ed., Lippincott, p. 1054
2. Metabolic Activation
- Cyanocobalamin is a pro-vitamin. After absorption, the cyanide is removed and it must be converted to either methylcobalamin or 5'-deoxyadenosylcobalamin to become biologically active. This conversion occurs in the cytosol and mitochondria respectively. - Katzung's Basic & Clinical Pharmacology, 16th ed.
- Methylcobalamin is already in the active coenzyme form and can participate directly in enzymatic reactions without requiring conversion.
3. Biochemical Roles
Both ultimately provide the same coenzyme functions:
Methylcobalamin (cytosolic):
- Cofactor for methionine synthase - transfers a methyl group from N⁵-methyltetrahydrofolate to homocysteine, converting it to methionine
- This reaction is essential for regenerating tetrahydrofolate (THF) for DNA synthesis (purines + dTMP)
- Also maintains S-adenosylmethionine (SAM) levels for methylation reactions
- Goodman & Gilman's, p. 638
5'-Deoxyadenosylcobalamin (mitochondrial):
- Cofactor for methylmalonyl-CoA mutase - converts methylmalonyl-CoA to succinyl-CoA
- Deficiency causes accumulation of unusual odd-chain and branched fatty acids, which incorporate into neuronal cell membranes - this is thought to underlie the neurological damage of B12 deficiency
4. Absorption and Pharmacokinetics
Both forms require intrinsic factor (IF) for intestinal absorption when taken orally at physiologic doses, though high-dose oral supplementation (~1000 mcg/day) allows some passive absorption even without IF.
- Average daily requirement: ~2 mcg
- Total body stores: 3,000-5,000 mcg (mainly liver)
- At doses >100 mcg, excess is rapidly cleared by the kidneys
- Transport in blood is bound to transcobalamins I, II, and III
- Katzung's Basic & Clinical Pharmacology, 16th ed.
5. Clinical Use and Therapeutic Preference
| Aspect | Cyanocobalamin | Methylcobalamin |
|---|---|---|
| Route | IM/SC injection, oral | Oral, sublingual, IM |
| Standard treatment | Yes - first-line for deficiency | Used, especially in Japan/Asia |
| Pernicious anemia | IM injection standard of care | Less common in Western practice |
| Neurological deficiency | IM cyanocobalamin preferred | Some evidence for preferential neural uptake |
| Cost | Cheaper, very stable | More expensive |
| Conversion needed | Yes | No |
Goodman & Gilman's states: "The treatment of choice for vitamin B12 deficiency is cyanocobalamin administered by intramuscular or subcutaneous injection" for serious deficiency with hematological or neurological manifestations.
Katzung notes: hydroxocobalamin is actually preferred over cyanocobalamin for injection because it is more protein-bound and remains longer in circulation.
For hereditary cobalamin deficiency (inborn errors of cobalamin metabolism), injected cyanocobalamin is the standard treatment, with about 10% retention per injection. - Yamada's Gastroenterology, 7th ed.
6. Safety - the Cyanide Question
Cyanocobalamin contains a cyanide moiety, which is released when it is metabolized. The amount is pharmacologically trivial at therapeutic doses and poses no toxicity risk in healthy individuals. However, it is theoretically better to avoid cyanocobalamin in patients with tobacco amblyopia (optic neuropathy from chronic cyanide exposure in heavy smokers) or Leber's hereditary optic neuropathy, where cyanide handling is already impaired. Hydroxocobalamin or methylcobalamin are preferred in these patients.
7. Practical Summary
- Cyanocobalamin: cheapest, most stable, gold-standard injectable form for treating deficiency; requires metabolic conversion; suitable for most patients
- Methylcobalamin: bioactive form requiring no conversion; preferred in some neurological contexts (diabetic neuropathy, peripheral neuropathy - particularly popular in Asian clinical practice) and in patients with cyanide metabolism concerns; less stable, higher cost
- For dietary supplementation in otherwise healthy individuals, either form is effective
- For severe deficiency (megaloblastic anemia, subacute combined degeneration of the spinal cord), parenteral therapy is mandatory - oral supplementation alone is unreliable
Sources: Biochemistry 8th ed. Lippincott Illustrated Reviews, p. 1054 | Katzung's Basic & Clinical Pharmacology 16th ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics | Yamada's Textbook of Gastroenterology 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.