explain me 10 common heart disease with ecg changes and ecg images of those disease
Reading File
Finding Sources
Searching Images
ECG changes myocardial infarction ST elevation
Finding Sources
Searching Images
atrial fibrillation ECG irregular rhythm absent P waves
Searching Images
complete heart block third degree AV block ECG
Searching Images
ventricular tachycardia ECG wide complex regular tachycardia
Searching Images
left ventricular hypertrophy ECG voltage criteria Sokolow
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain
Searching Images
pericarditis ECG saddle shaped ST elevation diffuse PR depression
Searching Images
Wolff-Parkinson-White syndrome ECG delta wave short PR interval
Searching Images
hyperkalemia ECG peaked T waves wide QRS sine wave
Searching Images
long QT syndrome ECG prolonged QT interval torsades de pointes
Searching the Web
10 common heart diseases ECG changes electrocardiogram findings clinical cardiology
Here is a comprehensive guide to 10 common heart diseases and their ECG changes, with real ECG images for each.
10 Common Heart Diseases: ECG Changes & Images
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
What it is
Complete occlusion of a coronary artery causing transmural (full-thickness) myocardial infarction. A true cardiac emergency requiring immediate reperfusion.
ECG Changes
| Finding | Detail |
|---|---|
| ST elevation | ≥1 mm in ≥2 contiguous limb leads; ≥2 mm in precordial leads |
| Hyperacute T-waves | Tall, peaked T-waves in the early (minutes) phase |
| Reciprocal ST depression | Mirror-image changes in opposing leads |
| Pathological Q-waves | Develop >6 hours after onset (>40 ms wide, >1/4 R height) |
| T-wave inversion | Late phase, indicating reperfusion or evolving infarction |
Localization:
- Anterior (LAD): V1–V4 elevation
- Inferior (RCA/LCx): II, III, aVF elevation
- Lateral (LCx): I, aVL, V5–V6 elevation
- Posterior (RCA/LCx): V1–V3 ST depression + tall R waves
ECG Image — Anterior STEMI (LAD Occlusion)

Convex "tombstone" ST elevation in V1–V6, hyperacute T-waves in V2–V4, reciprocal ST depression in II, III, aVF. Classic proximal LAD occlusion.
ECG Image — Inferior STEMI with Posterior Extension
ST elevation in II, III, aVF (inferior); prominent R waves and ST depression V1–V3 (posterior wall); reciprocal depression in I, aVL.
2. 🫀 Atrial Fibrillation (AF)
What it is
Chaotic, disorganized atrial electrical activity causing an irregularly irregular ventricular response. Most common sustained cardiac arrhythmia.
ECG Changes
| Finding | Detail |
|---|---|
| Absent P waves | Replaced by irregular fibrillatory (f) waves, best seen in V1 |
| Irregularly irregular R-R intervals | No pattern to QRS spacing |
| Narrow QRS | Unless aberrant conduction or pre-excitation |
| Variable ventricular rate | 60–180+ bpm depending on AV nodal conduction |
| Fibrillatory baseline | Undulating 350–600 Hz baseline activity |
ECG Image — Atrial Fibrillation with Rapid Ventricular Response
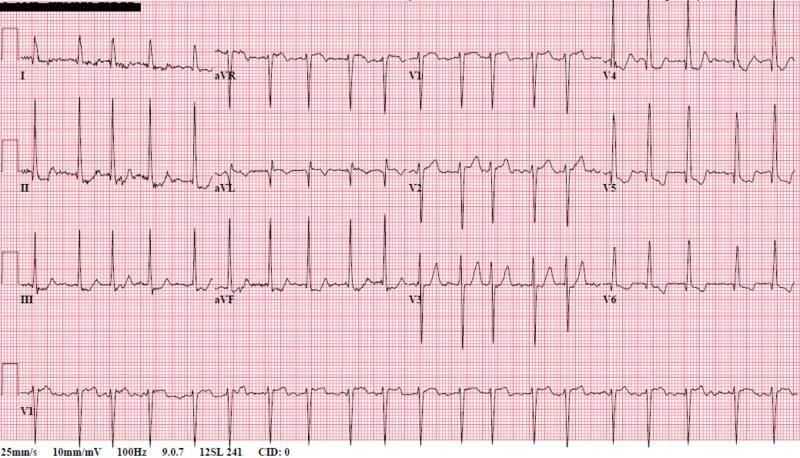
Classic AF: absent P waves replaced by fibrillatory baseline, completely irregularly irregular QRS complexes, rapid ventricular response.
3. 🫀 Complete (Third-Degree) AV Block
What it is
Total failure of conduction through the AV node — atria and ventricles beat completely independently. Life-threatening; requires permanent pacemaker.
ECG Changes
| Finding | Detail |
|---|---|
| AV dissociation | P waves and QRS have no fixed relationship |
| Regular P waves | Normal atrial rate (60–100 bpm) |
| Slow escape rhythm | Ventricular rate 20–40 bpm (infra-Hisian) or 40–60 bpm (junctional) |
| Wide QRS | If ventricular escape (>120 ms); narrow if junctional escape |
| Bradycardia | Ventricular rate independently slow |
ECG Image — Third-Degree AV Block
Complete AV dissociation: P waves "march through" QRS complexes with no fixed PR interval. Wide QRS escape rhythm at ~55 bpm — infra-nodal origin.
4. 🫀 Ventricular Tachycardia (VT)
What it is
Three or more consecutive ventricular beats at >100 bpm, originating below the bundle of His. Can degenerate into ventricular fibrillation.
ECG Changes
| Finding | Detail |
|---|---|
| Wide QRS tachycardia | QRS >120 ms (often >140–160 ms) |
| Rate 100–250 bpm | Regular monomorphic VT most common |
| AV dissociation | P waves independent of QRS (diagnostic when seen) |
| Fusion/capture beats | Pathognomonic of VT |
| Concordance | All V1–V6 positive or all negative |
| Northwest axis | Extremely negative QRS axis |
ECG Image — Monomorphic Ventricular Tachycardia
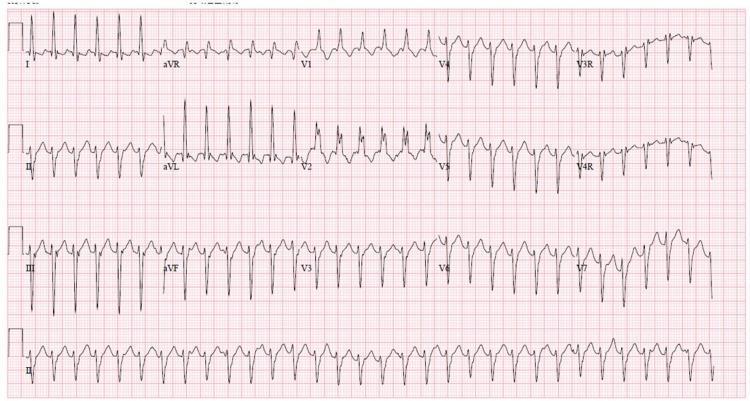
Wide QRS regular tachycardia at ~180 bpm. RBBB morphology with left axis deviation — classic fascicular VT. No visible P waves.
5. 🫀 Acute Pericarditis
What it is
Inflammation of the pericardial sac, usually viral. Causes sharp pleuritic chest pain, worse lying down, better sitting forward.
ECG Changes
| Finding | Detail |
|---|---|
| Diffuse saddle-shaped ST elevation | Concave (not convex) elevation in nearly ALL leads |
| PR segment depression | In most leads — highly specific for pericarditis |
| PR elevation in aVR | Reciprocal to PR depression elsewhere |
| ST depression only in aVR (±V1) | Unlike STEMI which is localized |
| Spodick's sign | Downsloping TP segment |
| No reciprocal ST depression | Distinguishes from STEMI |
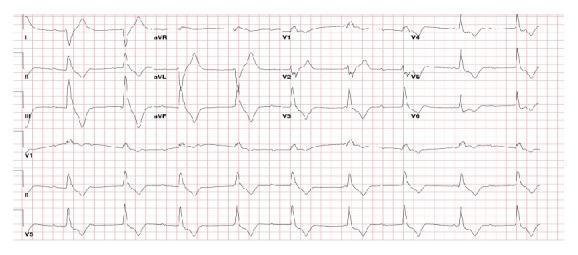
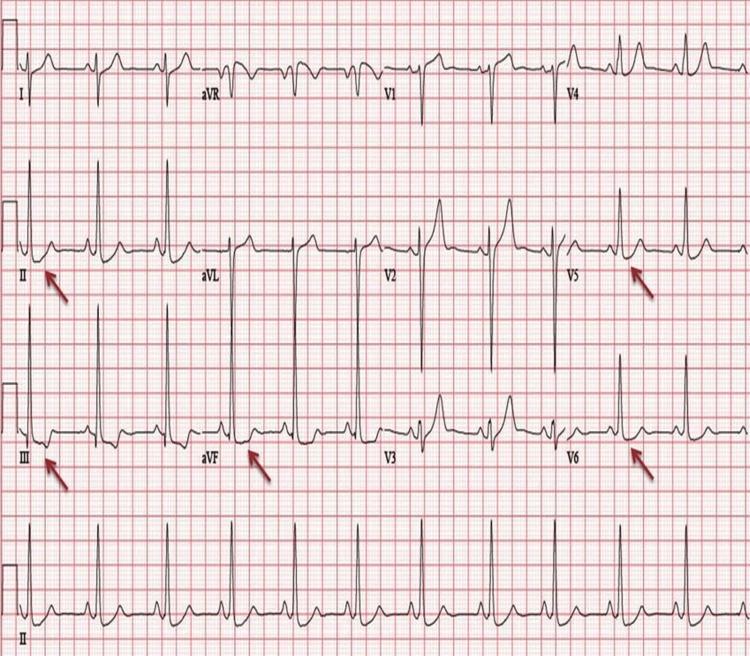
ECG Image — Acute Pericarditis

Diffuse concave "saddle-shaped" ST elevation in I, II, III, aVF, V2–V6. PR depression in lead II (arrowed). ST depression and PR elevation in aVR. Classic pericarditis.
6. 🫀 Pulmonary Embolism (PE)
What it is
Thrombotic occlusion of pulmonary arteries causing acute right ventricular pressure overload. ECG changes reflect acute cor pulmonale.
ECG Changes
| Finding | Detail |
|---|---|
| Sinus tachycardia | Most common (>90% of cases) |
| S1Q3T3 pattern | Deep S in I, Q wave in III, inverted T in III |
| Right axis deviation | New rightward shift |
| RBBB | Complete or incomplete (right ventricular strain) |
| T-wave inversions V1–V4 | Right ventricular strain pattern |
| P pulmonale | Peaked P waves if severe |
ECG Image — Pulmonary Embolism (S1Q3T3 + Right Heart Strain)

Sinus tachycardia 116 bpm. S1Q3T3 pattern visible. T-wave inversions V1–V3 with incomplete RBBB — classic acute right heart strain from PE.
7. 🫀 Left Ventricular Hypertrophy (LVH)
What it is
Pathological increase in left ventricular muscle mass, most commonly from chronic hypertension, aortic stenosis, or hypertrophic cardiomyopathy.
ECG Changes
| Finding | Detail |
|---|---|
| High QRS voltage | Sokolow-Lyon: SV1 + RV5/V6 ≥35 mm |
| Cornell criteria | RaVL + SV3 >28 mm (men), >20 mm (women) |
| Left axis deviation | QRS axis −30° or more leftward |
| LV strain pattern | ST depression + T-wave inversion in V5–V6, I, aVL |
| Left atrial enlargement | Wide notched P wave (P mitrale) |
| Poor R-wave progression | Secondary finding |
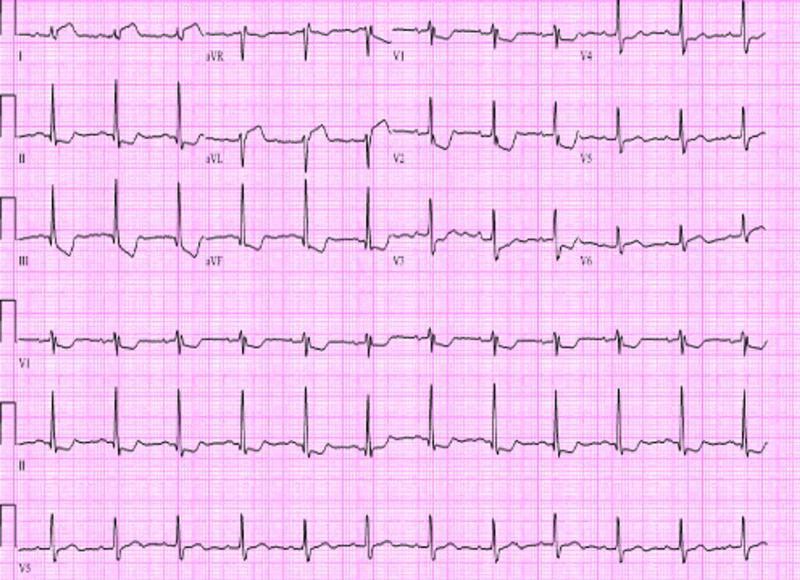
ECG Image — LVH with Strain Pattern
High QRS voltage meeting Sokolow-Lyon criteria. ST depression and T-wave inversions in II, III, aVF, V5, V6 — classic "strain pattern" indicating severe hypertrophy.
8. 🫀 Wolff-Parkinson-White (WPW) Syndrome
What it is
Pre-excitation syndrome caused by an accessory conduction pathway (Bundle of Kent) that bypasses the AV node, allowing early ventricular activation.
ECG Changes
| Finding | Detail |
|---|---|
| Short PR interval | <120 ms (bypasses AV nodal delay) |
| Delta wave | Slurred initial upstroke of QRS |
| Wide QRS | ≥120 ms (fusion of delta wave + normal conduction) |
| Secondary ST-T changes | Discordant T-waves due to abnormal depolarization |
| Pseudo-infarction | Negative delta waves mimic Q waves |
| Risk of AF → VF | Rapid conduction via accessory pathway is dangerous |
ECG Image — WPW Syndrome

Sinus rhythm with classically short PR interval (<120 ms). Prominent delta waves slurring QRS onset in II, III, aVF, V2–V6. Widened QRS duration — classic WPW triad.
9. 🫀 Long QT Syndrome (LQTS)
What it is
Congenital or acquired disorder of cardiac repolarization causing a prolonged QT interval, predisposing to Torsades de Pointes (TdP) — a potentially fatal polymorphic VT.
ECG Changes
| Finding | Detail |
|---|---|
| Prolonged QTc | >440 ms (men), >460 ms (women); dangerous >500 ms |
| Corrected QT (QTc) | QT ÷ √RR (Bazett's formula) |
| T-wave morphology | Notched, biphasic, or broad T-waves depending on LQTS subtype |
| T-wave alternans | Beat-to-beat variation in T-wave amplitude — high-risk sign |
| Torsades de Pointes | Polymorphic VT with twisting QRS around isoelectric line |
| "R on T" phenomenon | Triggers TdP — PVC landing on T-wave |
ECG Image — Long QT with Torsades de Pointes
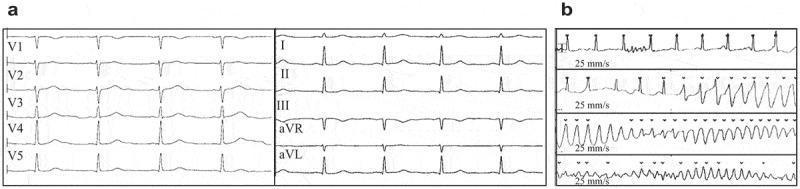
Panel (a): Baseline sinus rhythm with markedly prolonged QTc = 478 ms. Panel (b): Onset of Torsades de Pointes — polymorphic VT with characteristic "twisting" of QRS complexes around the isoelectric line.
10. 🫀 Hyperkalemia (Electrolyte Cardiac Emergency)
What it is
Elevated serum potassium (>5.5 mmol/L) causing progressive ECG changes that can lead to fatal arrhythmias if untreated. Common in renal failure, Addison's disease, acidosis.
ECG Changes (Progressive with Rising K⁺)
| K⁺ Level | ECG Change |
|---|---|
| 5.5–6.5 mmol/L | Peaked ("tented") T-waves — narrow base, tall amplitude |
| 6.5–7.0 mmol/L | PR prolongation, flattened/absent P waves |
| 7.0–8.0 mmol/L | Wide QRS (>120 ms), intraventricular conduction delay |
| >8.0 mmol/L | Sine-wave pattern — QRS merges with T-wave |
| >10 mmol/L | Ventricular fibrillation or asystole |
ECG Image — Severe Hyperkalemia
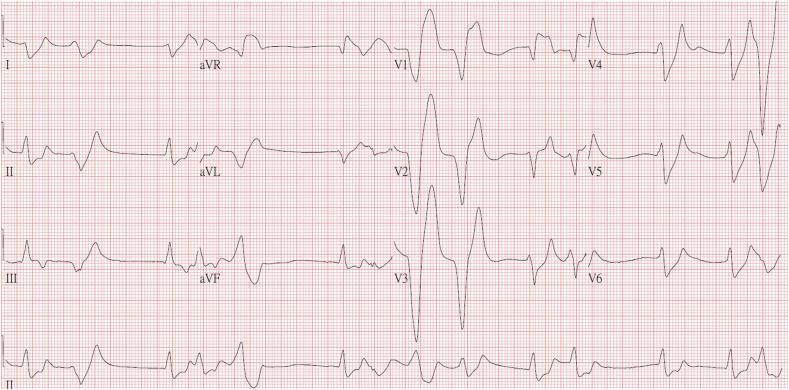
Severe hyperkalemia (K⁺ = 9.2 mmol/L): absent P waves (atrial standstill), massively widened QRS complexes, tall peaked T-waves with sine-wave appearance in precordial leads. Critical emergency.
Quick Reference Summary
| # | Condition | Key ECG Feature |
|---|---|---|
| 1 | STEMI | Convex ST elevation in contiguous leads + reciprocal changes |
| 2 | Atrial Fibrillation | Absent P waves + irregularly irregular rhythm |
| 3 | Complete Heart Block | AV dissociation + slow escape rhythm |
| 4 | Ventricular Tachycardia | Wide QRS tachycardia >100 bpm + AV dissociation |
| 5 | Acute Pericarditis | Diffuse saddle-shaped ST elevation + PR depression |
| 6 | Pulmonary Embolism | Sinus tachycardia + S1Q3T3 + RV strain |
| 7 | LV Hypertrophy | High QRS voltage + lateral strain pattern |
| 8 | WPW Syndrome | Short PR + delta wave + widened QRS |
| 9 | Long QT Syndrome | QTc >500 ms + T-wave alternans → Torsades |
| 10 | Hyperkalemia | Peaked T-waves → wide QRS → sine wave |
Clinical Pearl: Always interpret the ECG in clinical context. The same ECG change (e.g., ST elevation) can appear in STEMI, pericarditis, Brugada syndrome, or LV aneurysm — history and troponins are essential for accurate diagnosis.
This is a shared conversation. Sign in to Orris to start your own chat.