midgut rotation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a detailed overview of midgut rotation based on authoritative embryology and surgery textbooks.
Midgut Rotation
Overview
The midgut gives rise to most of the small intestine (distal duodenum to mid-transverse colon) and is supplied entirely by the superior mesenteric artery (SMA). As the midgut elongates rapidly in early development, the abdominal cavity is temporarily too small to contain it, and a physiologic herniation occurs. Rotation is the process by which the gut assumes its normal adult position.
Stages
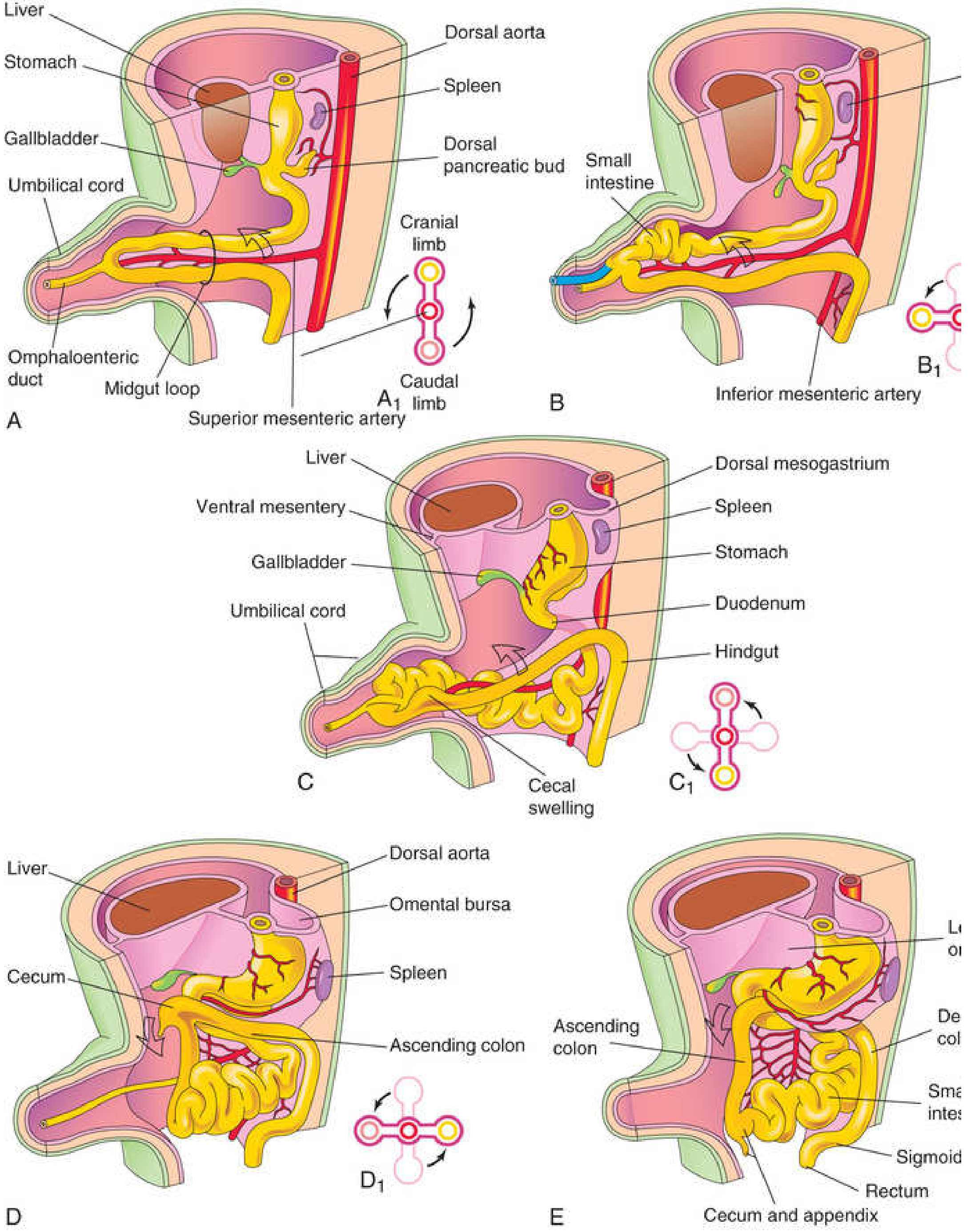
Stage 1 - Physiologic Herniation (~week 6)
- The rapidly elongating midgut forms a U-shaped loop that herniates through the umbilical ring into the proximal umbilical cord.
- The loop has two limbs:
- Cranial limb - gives rise to the jejunum and ileum (elongates rapidly into small intestinal coils)
- Caudal limb - gives rise to the cecum, ascending colon, and proximal transverse colon (develops a small cecal swelling/diverticulum, the primordium of the cecum and appendix)
- The apex of the loop is attached to the omphaloenteric (vitelline) duct.
Stage 2 - Rotation during herniation (~week 6-10)
- While still outside the abdomen, the midgut loop rotates 90° counterclockwise around the axis of the SMA (viewed from the front).
- This carries the cranial limb to the right and the caudal limb to the left.
- Total rotation during this phase: 90°
Stage 3 - Return to abdomen (~week 10)
- The intestines return to the abdominal cavity during the 10th week, driven partly by:
- Enlargement of the abdominal cavity
- Regression of the mesonephric kidney
- Relative decrease in liver size
- The small intestine re-enters first, passing posterior to the SMA, and occupies the central abdomen.
- As the large intestine returns, it undergoes a further 180° counterclockwise rotation.
- Total rotation = 270° counterclockwise around the SMA.
Stage 4 - Fixation
- The cecum temporarily lies in the right upper quadrant (subhepatic), then descends to the right iliac fossa, establishing the ascending colon on the right.
- As the colon presses structures against the posterior abdominal wall:
- The duodenum (except its first part) becomes retroperitoneal
- The ascending colon and descending colon mesenteries fuse with the posterior parietal peritoneum and disappear (both become retroperitoneal)
- The head of the pancreas becomes retroperitoneal
- During cecal descent, the appendix forms from the narrowing distal end of the cecal bud; in ~50% of cases it ends up retrocecal or retrocolic.
Summary of 270° Rotation
| Phase | Rotation | Event |
|---|---|---|
| During herniation (in umbilical cord) | 90° CCW | Cranial limb swings right |
| During return to abdomen | 180° CCW | Large intestine completes rotation |
| Total | 270° CCW | Around the SMA axis |
Anomalies of Midgut Rotation
1. Nonrotation (most common)
- The intestine fails to rotate on returning to the abdomen.
- The small intestine lies entirely on the right, the large intestine on the left.
- The cecum lies just inferior to the pylorus (subhepatic cecum).
- Only two points are attached to the posterior wall (duodenum + proximal colon), leaving the midgut suspended on a narrow SMA stalk.
2. Malrotation / Incomplete rotation
- Rotation stops before completing the full 270°.
- Ladd bands (peritoneal bands) from the cecum to the posterior wall cross and compress the duodenum, causing obstruction.
- The narrow mesenteric stalk predisposes to midgut volvulus.
3. Midgut Volvulus - Surgical Emergency
- The midgut twists around the SMA stalk, obstructing the SMA itself.
- Results in intestinal ischemia, infarction, and gangrene of the entire midgut.
- Classic presentation: bilious emesis in a neonate/infant - an ominous sign that mandates urgent investigation.
- Distended abdomen and metabolic acidosis are late signs indicating life-threatening ischemia.
- Diagnosis: upper GI contrast series (duodenal C-loop fails to cross midline; small bowel on right side); ultrasound may show reversal of the normal SMA/SMV relationship (vein normally lies to the right of artery).
- Treatment: open laparotomy, detorsion of volvulus, Ladd's procedure (lysis of Ladd bands, widening of mesentery, appendectomy).
4. Reversed Rotation (rare)
- The midgut loop rotates clockwise instead of counterclockwise.
- Duodenum lies anterior to the SMA (normally passes posterior).
- Transverse colon may be obstructed by the SMA.
5. Subhepatic Cecum and Appendix
- Failure to complete the final 90° of rotation; cecum arrests below the liver.
Key Facts
- Incidence of rotational anomalies: ~2-5 in 1,000 live births (autopsy); clinically apparent: ~1 in 6,000 live births.
- Up to 90% present before 12 months of age, but up to 1% can first present in adults.
- Malrotation is frequently associated with other anomalies occurring during weeks 4-12 of gestation: diaphragmatic hernia, gastroschisis, omphalocele.
- The SMA is the anatomic axis of rotation throughout the entire process.
Sources: The Developing Human: Clinically Oriented Embryology (Moore et al.), pp. 632-646; Langman's Medical Embryology, p. 266-267; Sabiston Textbook of Surgery, pp. 3286-3292
development of interstitial septum
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.