Appendicitis
Reading File
Finding Sources
Searching PubMed
appendicitis diagnosis management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks plus recent PubMed evidence. Here is the full, organized answer:
Appendicitis
Epidemiology
Appendicitis is the most common intra-abdominal surgical emergency, affecting approximately 1 in 1,000 adults annually worldwide. Lifetime prevalence is 8.7% in men and 6.9% in women. The peak incidence is between ages 9-12 years, though it can occur at any age. It is uncommon in children under 5, but when it does occur in that age group, perforation rates exceed 50% at presentation. - Goldman-Cecil Medicine, 22e
Pathophysiology
The appendix is a blind-ended pouch arising from the cecum. Obstruction of the appendiceal lumen - most commonly by a fecalith (appendicolith), but also by lymphoid hyperplasia or tumors (e.g., carcinoid) - triggers a cascade:
- Luminal distension and mucosal ischemia
- Bacterial overgrowth and invasion
- Edema, vasocongestion, inflammation
- Infarction and necrosis
- Perforation
There is growing evidence that uncomplicated and complicated (gangrenous/perforated) appendicitis are distinct pathophysiologic entities rather than a simple continuum - Sabiston Textbook of Surgery, 21e
Clinical Features
Classic Presentation
- Abdominal pain - begins as vague, crampy, periumbilical pain, then migrates to the right lower quadrant (RLQ) over 24 hours as parietal peritoneum becomes involved
- Anorexia (almost universal)
- Nausea and vomiting (typically follow pain onset)
- Low-grade fever (usually later in the course)
Physical Examination
| Finding | Description | Sensitivity / Specificity |
|---|---|---|
| McBurney point tenderness | Maximal tenderness 2/3 from umbilicus to anterior superior iliac spine | Classic finding |
| Rovsing sign | RLQ pain on palpation of the LLQ | Sens 7-68%, Spec 58-96% |
| Psoas sign | Pain with passive right hip extension (patient on left side) | Sens 13-42%, Spec 79-95% |
| Obturator sign | RLQ pain with internal/external rotation of flexed right hip | Sens 8%, Spec 94% |
| Rebound tenderness | Pain on sudden release of RLQ pressure | LR+ 1.1-6.3 |
Note: Abdominal rigidity and diffuse peritonitis suggest perforation. The classic signs have low sensitivity individually; it is the combined clinical picture that drives diagnosis. - Rosen's Emergency Medicine, 10e
Laboratory Studies
- WBC: Leukocytosis (>10,000/µL) present in ~90% of cases; normal WBC in 10% - does not exclude appendicitis
- CRP / Procalcitonin: CRP is the most sensitive biomarker but lacks specificity
- Urinalysis: Mild sterile pyuria (<5-10 WBC/hpf) occurs due to proximity to the ureter - does not indicate UTI
- Pregnancy test: Mandatory in all females of childbearing age to exclude ectopic pregnancy
No single lab test is sufficient to diagnose or exclude appendicitis. - Sabiston Textbook of Surgery
Clinical Scoring Systems
Three validated scoring tools stratify patients into low, moderate, and high probability:
| Criterion | Alvarado Score | Pediatric Appendicitis Score (PAS) | AIR Score |
|---|---|---|---|
| Migration of pain to RLQ | 1 | 1 | - |
| Anorexia | 1 | 1 | - |
| Nausea/vomiting | 1 | 1 | - |
| RLQ tenderness | 2 | 2 | 1-2 |
| Rebound tenderness | 1 | 1 | 1-3 |
| Elevated temperature | 1 | 1 | - |
| Leukocytosis | 2 | 2 | 1-2 |
| Left shift (bands) | - | - | 1 |
| CRP elevation | - | - | 1-2 |
| Max Score | 10 | 10 | 12 |
- Score ≤3: Low probability; consider discharge with return precautions
- Score 4-6: Moderate probability; imaging recommended
- Score ≥7: High probability; surgical consultation
Current consensus guidelines recommend the AIR or Adult Appendicitis Score (AAS) over the Alvarado score, as the Alvarado is better at ruling out appendicitis than ruling it in. - Sabiston Textbook of Surgery
Imaging
Ultrasound (US)
- First-line in children and pregnant women (no ionizing radiation)
- Graded compression technique: sensitivity 74-94%, specificity 85-93%
- US findings of appendicitis: non-compressible tubular structure >6mm in diameter, increased periappendiceal echogenicity (fat stranding), appendicolith (echogenic focus with shadowing)
- Key limitation: the appendix is frequently not visualized (non-diagnostic study) due to body habitus, bowel gas, or atypical position
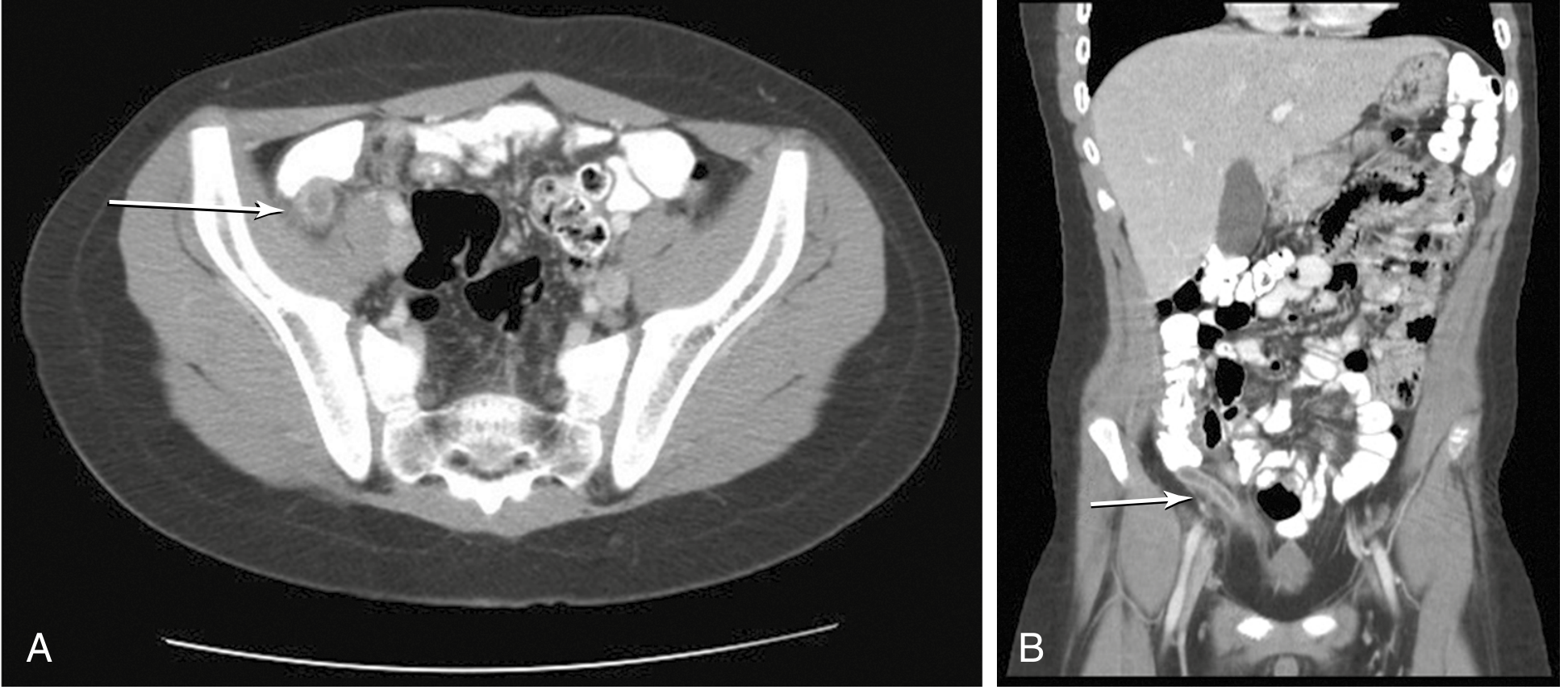
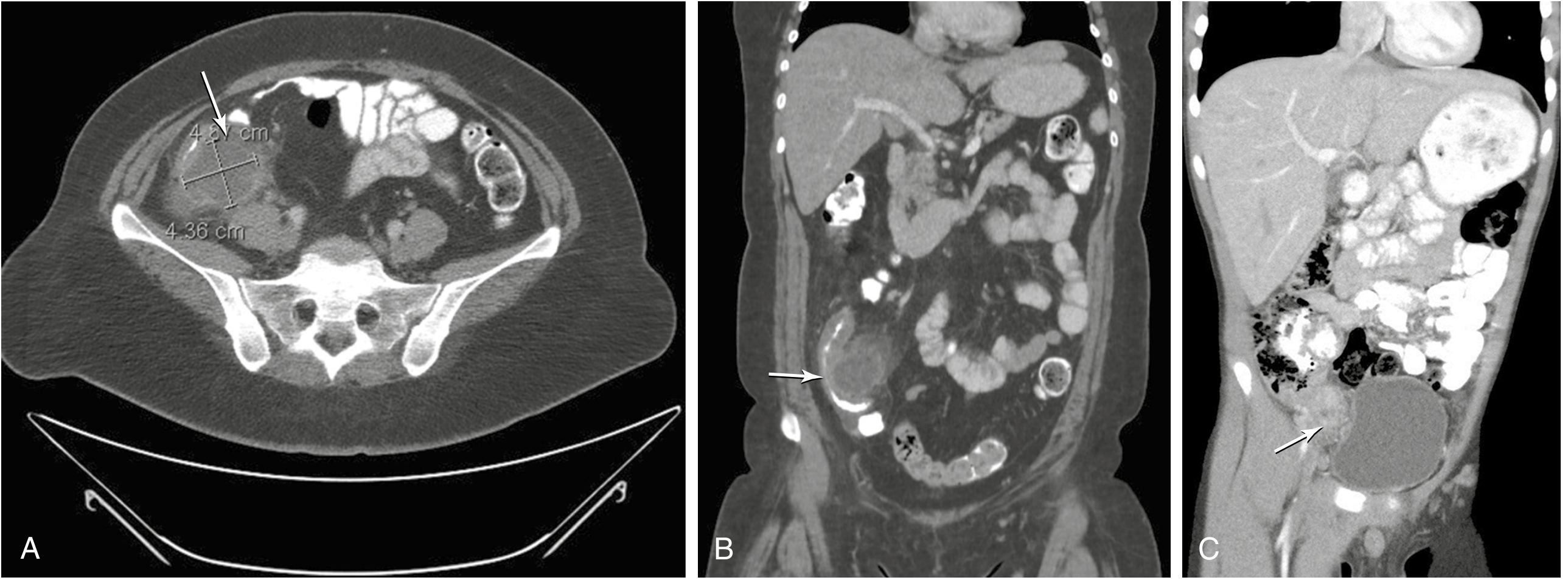
CT Abdomen/Pelvis (with or without contrast)
- Preferred modality in adults - sensitivity/specificity ≥94%
- Findings: dilated appendix (>6mm), appendiceal wall thickening, periappendiceal fat stranding, appendicolith, pericecal fluid
- Low-dose CT (2 mSv) is comparable in accuracy to standard-dose CT
- Reduces negative appendectomy rate from ~12% to ~6%
MRI
- Accuracy comparable to CT, but more expensive and time-consuming
- Preferred in pregnancy when US is non-diagnostic (avoids radiation)
Differential Diagnosis
Surgical causes: mesenteric adenitis, Meckel's diverticulitis, Crohn's ileitis, intestinal obstruction, perforated peptic ulcer, cholecystitis, diverticulitis
Gynecologic causes: ectopic pregnancy, ovarian torsion, ruptured ovarian cyst, pelvic inflammatory disease (PID), endometriosis - these account for 48-73% of cases where laparoscopy reveals a normal appendix in women
Medical causes: right-sided renal colic, urinary tract infection, psoas abscess, Yersinia/Campylobacter enteritis
Treatment
Uncomplicated Appendicitis
Surgery (standard of care): Appendectomy - laparoscopic preferred over open.
- Laparoscopic: fewer wound infections (50% lower), shorter hospital stay (~1.1 days), less postoperative pain, faster return to activity
- Open appendectomy: preferred when there is evidence of perforation or when laparoscopy is not feasible
Preoperative antibiotics reduce wound infection rates. Regimens include:
- Cefotetan 2 g IV, OR
- Cefoxitin 2 g IV (followed by 3 postoperative doses), OR
- Ticarcillin-clavulanic acid
Nonoperative management (antibiotics alone):
- IV antibiotics can resolve symptoms in the majority of patients in the short term
- However, a meta-analysis of 5 RCTs found a 40% treatment failure rate, mostly due to recurrent appendicitis
- Cannot currently identify "self-limiting" cases prospectively
- Waiting risks perforation, which increases mortality from 0.0002% to 3% and morbidity from 3% to 47%
- Current practice in the USA: surgery remains the initial treatment of choice
Complicated Appendicitis (Perforated / Abscess / Phlegmon)
- Early perforation: appendectomy is still the treatment
- Well-formed abscess/phlegmon (symptoms >5 days): percutaneous drain placement (IR-guided) + IV antibiotics, followed by interval appendectomy in 6-8 weeks
- Broad-spectrum antibiotics required; duration based on clinical response
Special Populations
Pediatric
- Laparoscopic appendectomy is the standard of care
- Ultrasound and MRI are preferred over CT to avoid long-term radiation risks
- Nonoperative management with antibiotics is viable in uncomplicated cases (80-90% symptom resolution in 24-48h), but recurrence rates may reach 40% at medium-term follow-up
- Most pediatric surgeons still prefer operative management within 12-24h of diagnosis - Current Surgical Therapy, 14e
- A 2026 JAMA Pediatrics meta-analysis re-evaluated nonoperative management for pediatric uncomplicated appendicitis
Pregnancy
- Appendicitis is the most common surgical emergency in pregnancy (incidence same as non-pregnant)
- Delays in diagnosis contribute to increased perforation rates and fetal mortality
- The appendix is displaced in less than 25% of pregnant patients even in the 3rd trimester - atypical pain location is possible
- Physiologic leukocytosis in pregnancy can confuse the picture
- Imaging: US first; if non-diagnostic, MRI is the preferred follow-up (not CT)
Complications
| Complication | Notes |
|---|---|
| Perforation | ~1/3 of patients have luminal obstruction; perforation risk rises with symptom duration; increases mortality 0.0002% → 3% |
| Abscess/phlegmon | May be managed with drainage + interval appendectomy |
| Peritonitis | Diffuse spread more likely in children (undeveloped omentum) |
| Sepsis | Risk significantly higher in perforated disease |
| Bowel obstruction | Post-inflammatory adhesion |
Key Pearls
- A normal WBC does not exclude appendicitis (10% of confirmed cases have normal WBC)
- Right lower quadrant pain is the single best predictor (LR+ 7.3-8.5 in adults)
- Use the AIR or AAS score rather than Alvarado for modern risk stratification
- In women of childbearing age, always order a pregnancy test and consider pelvic pathology
- Appendicitis is a surgical urgency, not an emergency - brief preoperative optimization is appropriate; prolonged delay increases perforation risk
- The negative appendectomy rate with imaging is ~3.7% in children and ~6% in adults (vs. 12-13.5% without imaging)
Sources: Rosen's Emergency Medicine 10e | Sabiston Textbook of Surgery 21e | Goldman-Cecil Medicine 26e | Sleisenger & Fordtran's GI & Liver Disease | Current Surgical Therapy 14e
Recent evidence note: A 2026 JAMA Pediatrics systematic review and meta-analysis (PMID 41046476) re-evaluates nonoperative management for pediatric uncomplicated appendicitis - this may update current practice guidance for the pediatric population.
This is a shared conversation. Sign in to Orris to start your own chat.