Short note on 1. Fornix 2. Medial medullary syndrome 3. Pia mater of spinal cord 4. Sensory and motor speech area
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed. Here are the four short notes:
1. Fornix
The fornix (Latin: "arch") is a C-shaped white matter bundle that forms the major output pathway of the hippocampal formation, curving through the ventricular system from the hippocampus to the diencephalon and septal area. - Neuroanatomy through Clinical Cases, 3rd Ed.
Parts
- Alveus - a thin white matter sheet on the ventricular surface of the hippocampus where output fibers begin
- Fimbria - fibers sweeping medially to form a discrete bundle
- Crus (Crura) - the fimbria continues as the crus, curving under the corpus callosum
- Hippocampal commissure - connects crura of both sides on the undersurface of the corpus callosum
- Body - both crura join in the midline to form the body, running forward beneath the corpus callosum
- Columns - the body divides anteriorly and downward into two columns, which split further into:
- Postcommissural fornix (majority, from subiculum) - descends behind the anterior commissure to the mammillary nuclei of the hypothalamus
- Precommissural fornix (from subiculum + hippocampus) - passes anterior to anterior commissure to reach the lateral septal nucleus
- Some fibers project to the anterior thalamic nucleus
Papez Circuit
The fornix is the first limb of the Papez circuit:
Subiculum → Fornix → Mammillary nuclei → Mammillothalamic tract → Anterior thalamus → Cingulate gyrus → Cingulum → Parahippocampal gyrus → Entorhinal cortex → Hippocampus
Clinical Significance
- Bilateral fornix lesions cause anterograde amnesia (diencephalic memory loss)
- Cholinergic projections travel back through the fornix from the medial septal nuclei to the hippocampal formation, modulating memory function
2. Medial Medullary Syndrome (Dejerine Anterior Bulbar Syndrome)
Cause: Occlusion of the anterior spinal artery (or vertebral artery/lower basilar artery), causing infarction of the paramedian medulla. Less common causes include vertebrobasilar dissection, embolism, dolichoectasia, and meningovascular syphilis.
Structures Damaged
The anterior spinal artery supplies:
- The ipsilateral pyramid (corticospinal tract)
- The medial lemniscus
- The hypoglossal nerve and nucleus (CN XII)
Clinical Features
| Structure | Sign |
|---|---|
| Pyramid (corticospinal tract) | Contralateral hemiplegia of arm and leg, sparing the face |
| Medial lemniscus | Contralateral loss of position sense and vibration (spinothalamic/pain-temperature largely spared) |
| CN XII (hypoglossal) | Ipsilateral LMN tongue paralysis - tongue deviates toward the lesion on protrusion; atrophy and fasciculations (Note: CN XII may occasionally be spared) |
| MLF involvement (if extended) | Upbeat nystagmus |
Bilateral Medial Medullary Syndrome
Results in flaccid quadriplegia (facial sparing), bilateral LMN tongue lesions, complete loss of position and vibration sense in all four limbs, and potentially respiratory failure.
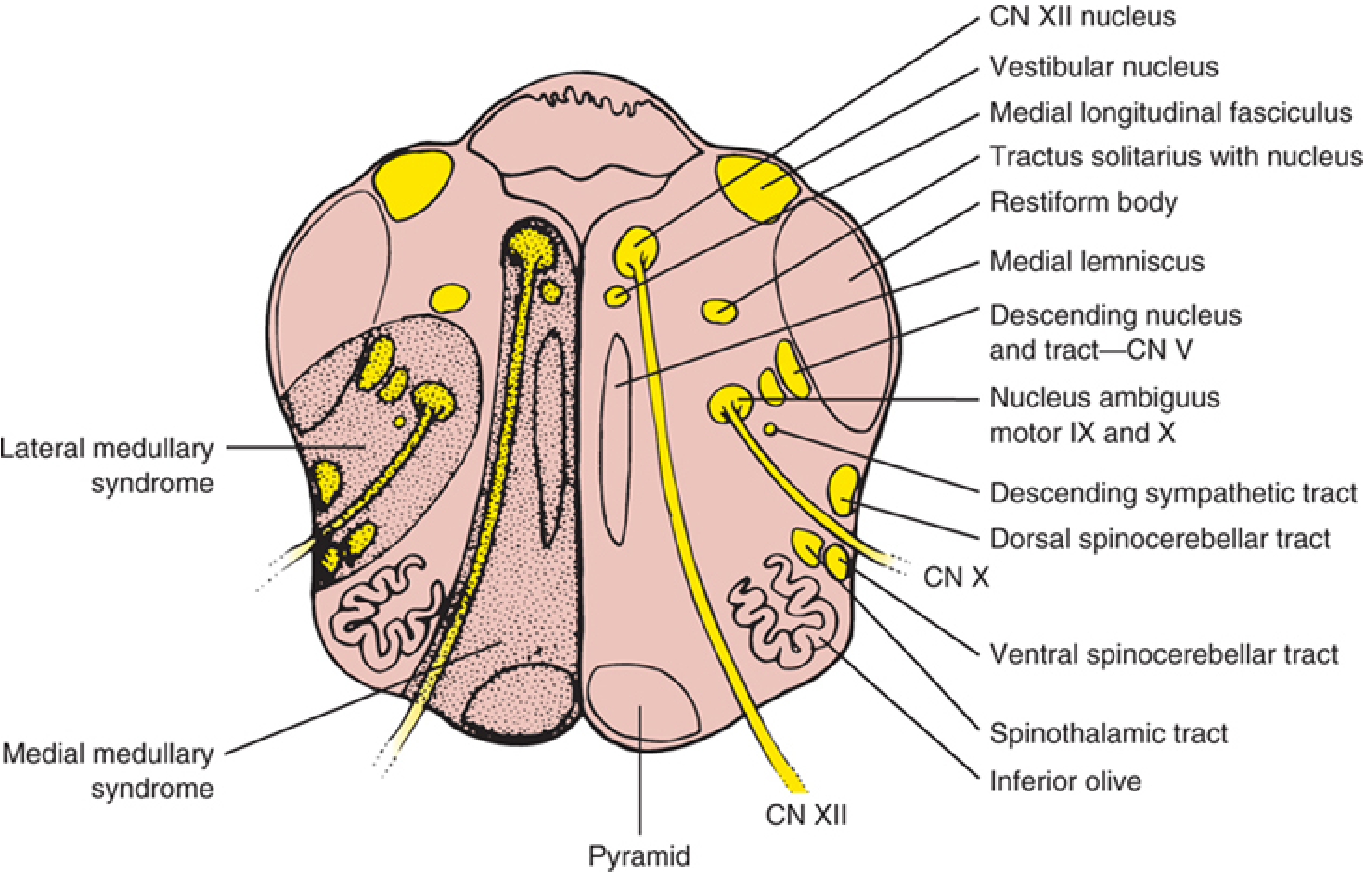
Cross-section of medulla oblongata showing structures involved - Localization in Clinical Neurology, 8e
3. Pia Mater of the Spinal Cord
The pia mater (Latin: "tender mother") is the innermost, highly vascular meningeal layer. It is a delicate connective tissue membrane that firmly adheres directly to the surface of the spinal cord, following all its contours. - Gray's Anatomy for Students
Key Features
Structure:
- Extends into the anterior median fissure of the spinal cord
- Reflects as sleeve-like coatings around posterior and anterior rootlets and roots as they cross the subarachnoid space
- Continuous with the perivascular connective tissue sheath of blood vessels of the brain and spinal cord
- Both surfaces of the pia are covered with a thin squamous epithelial layer
- Fuses with the arachnoid mater around openings for cranial and spinal nerves
Denticulate Ligament:
- A flat, continuous sheet of pia mater forming a longitudinally oriented band on each side of the spinal cord
- Runs between the posterior and anterior rootlets
- Extends laterally from the cord toward the arachnoid and dura mater
- Forms a series of triangular tooth-like extensions along its free border, each apex anchoring through the arachnoid to the dura mater (approximately 21 pairs)
- Function: Anchors and positions the spinal cord in the center of the subarachnoid space, preventing excessive lateral or rotational movement
Clinical Note
- The subarachnoid space (between arachnoid and pia) contains CSF and larger blood vessels
- The pia extends inferiorly as the filum terminale internum below the conus medullaris (L1-L2), blending with connective tissue to anchor the cord
4. Sensory and Motor Speech Areas
Speech involves a distributed network primarily in the dominant (usually left) hemisphere, with two major cortical areas:
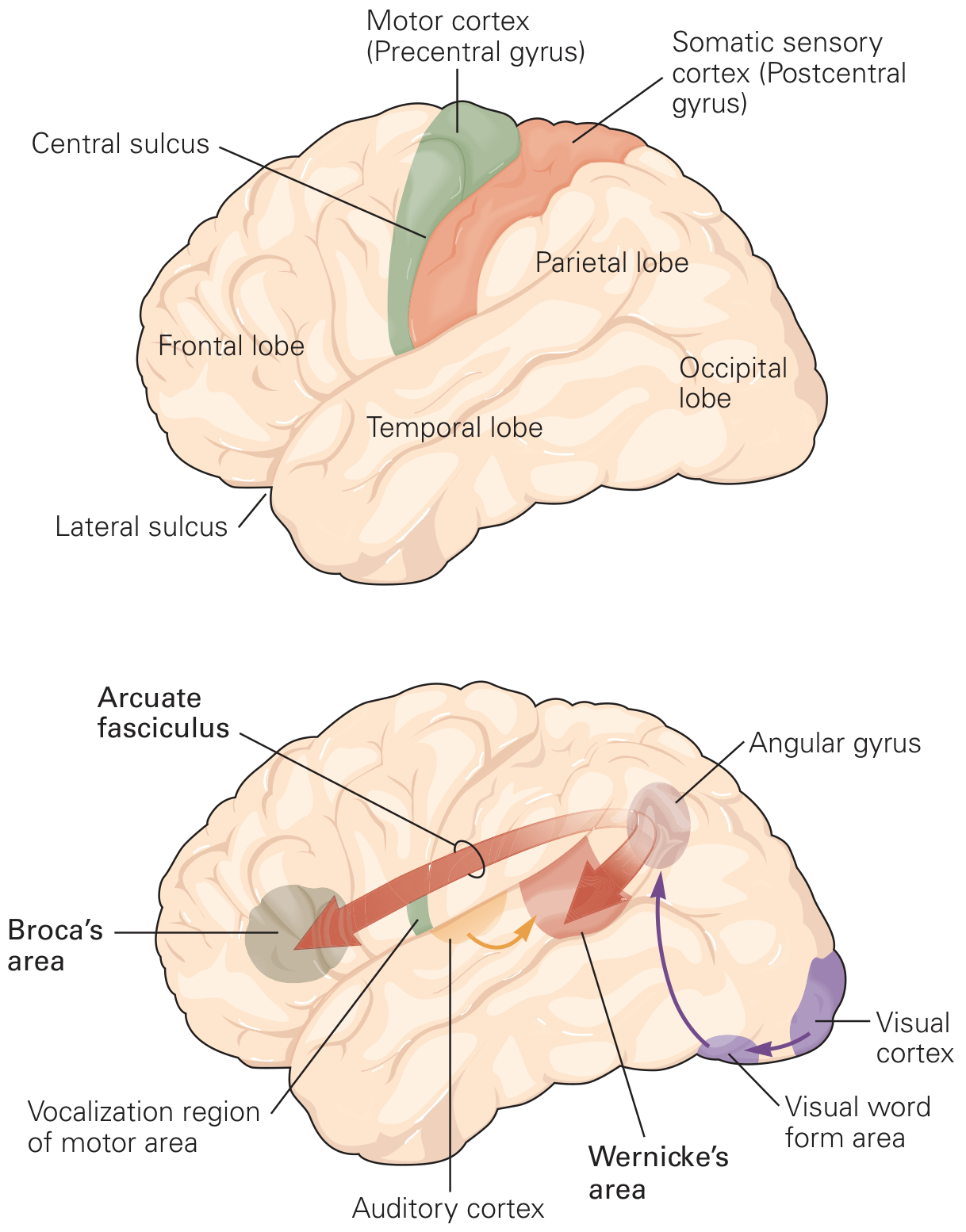
Language processing areas of the left cerebral hemisphere - Principles of Neural Science, 6th Ed.
Motor Speech Area - Broca's Area (Area 44, 45)
- Location: Inferior frontal gyrus (pars triangularis and pars opercularis) of the dominant frontal lobe, immediately anterior to the region of the motor cortex controlling the mouth, tongue, palate, and vocal cords
- Function: Contains the motor program for speech - coordinates mouth and tongue movements needed to form words; governs the production and articulation of speech
- Lesion: Broca's aphasia (expressive aphasia) - non-fluent, broken speech with effortful output; comprehension is relatively preserved; patient understands but cannot speak coherently
Sensory Speech Area - Wernicke's Area (Area 22)
- Location: Posterior part of the superior temporal gyrus in the dominant hemisphere, where the temporal lobe meets the parietal lobe, adjacent to the primary auditory cortex and the angular gyrus
- Function: Processes auditory input for language; governs comprehension and perception of spoken words (the "sensory program" for language)
- Lesion: Wernicke's aphasia (receptive aphasia) - fluent, grammatical but meaningless speech (paraphasias, neologisms); severely impaired comprehension and repetition
Connection Between the Two Areas
Broca's and Wernicke's areas are connected bidirectionally via the arcuate fasciculus (part of the superior longitudinal fasciculus). Damage to this connection causes conduction aphasia - fluent speech with poor repetition but intact comprehension.
Additional Language-Related Areas
- Angular gyrus (area 39): Integrates auditory and visual information; represents words in a polymodal sensory context - lesion causes alexia with agraphia
- Visual word form area: More ventral occipito-temporal cortex; important for reading
- Supplementary motor area: Involved in speech initiation
Sources: Principles of Neural Science 6th Ed., Neuroanatomy through Clinical Cases 3rd Ed., Localization in Clinical Neurology 8th Ed., Gray's Anatomy for Students, Histology: A Text and Atlas, Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.