Hip dislocations and displacements fractures related to hip
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content from the textbooks. Let me compile the complete, well-organized answer.
Hip Dislocations and Displaced Fractures of the Hip
PART 1 - HIP DISLOCATIONS
Overview
Native hip dislocations result from high-energy trauma, and up to 95% of patients have associated injuries. Motor vehicle collisions (particularly dashboard injuries) are the most common mechanism. Dislocations of prosthetic hips can occur with minimal trauma.
- Posterior dislocations: >90% of all hip dislocations
- Anterior dislocations: ~10% (superior/pubic or inferior/obturator)
Hip dislocation is an orthopaedic emergency. Reduction should occur within 6 hours. AVN risk rises from <10% at <10 hours to ~25% when delay extends to 15 hours.

Posterior hip dislocation - schematic view (Tintinalli's Emergency Medicine)
Anatomy of Dislocation
For any hip to dislocate, the ligamentum teres and at least part of the capsule must be disrupted. Labral tears/avulsions and muscular injury are common.
- Posterior dislocations: Capsule torn posteriorly or inferoposteriorly. The Y ligament (iliofemoral) is generally intact but stripped from its acetabular attachment.
- Anterior dislocations: The psoas acts as a fulcrum; capsule is disrupted anteroinferiorly. Femoral vessel injury, though rare, can occur in high-energy injuries.
1A. Posterior Hip Dislocation
Mechanism: Posterior force on a flexed knee - the classic "dashboard injury."
Clinical presentation:
- Limb shortened, adducted, and internally rotated (key distinguishing feature from femoral neck fracture, which is externally rotated)
- Associated injuries: acetabular fracture, femoral neck fracture, femoral shaft fracture, knee ligament injury
- Sciatic nerve injury in ~10% of cases
Imaging:
- AP + lateral pelvis radiograph
- CT of acetabulum and femur after identification

AP pelvis X-ray: right-sided posterior hip dislocation with acetabular fracture (Tintinalli's)
Reduction techniques (closed, with procedural sedation):
- Allis maneuver (most common): In-line traction with simultaneous hip flexion and internal rotation
- Multiple techniques described; EM physician should be proficient in more than one
- Anterior dislocations require OR reduction
Classification of Posterior Hip Dislocations
Thompson and Epstein Classification:
| Type | Description |
|---|---|
| I | Dislocation with or without minor fracture |
| II | Dislocation with single large fragment of posterior acetabular rim |
| III | Dislocation with comminuted rim fracture |
| IV | Dislocation with fracture of the acetabular floor |
| V | Dislocation with fracture of the femoral head |
Stewart and Milford Classification (addresses postreduction stability):
| Type | Description |
|---|---|
| I | Simple dislocation without fracture |
| II | One or more rim fragments; socket sufficient for stability after reduction |
| III | Rim fracture producing gross instability |
| IV | Dislocation with fracture of the head or neck of femur |
Pipkin Classification (for Type V Thompson/Epstein - femoral head fracture):
| Type | Description |
|---|---|
| I | Posterior dislocation with femoral head fracture caudad to the fovea |
| II | Posterior dislocation with femoral head fracture cephalad to the fovea |
| III | Femoral head fracture with associated femoral neck fracture |
| IV | Types I or II combined with acetabular fracture |
Brumback Classification (comprehensive, includes anterior and central):
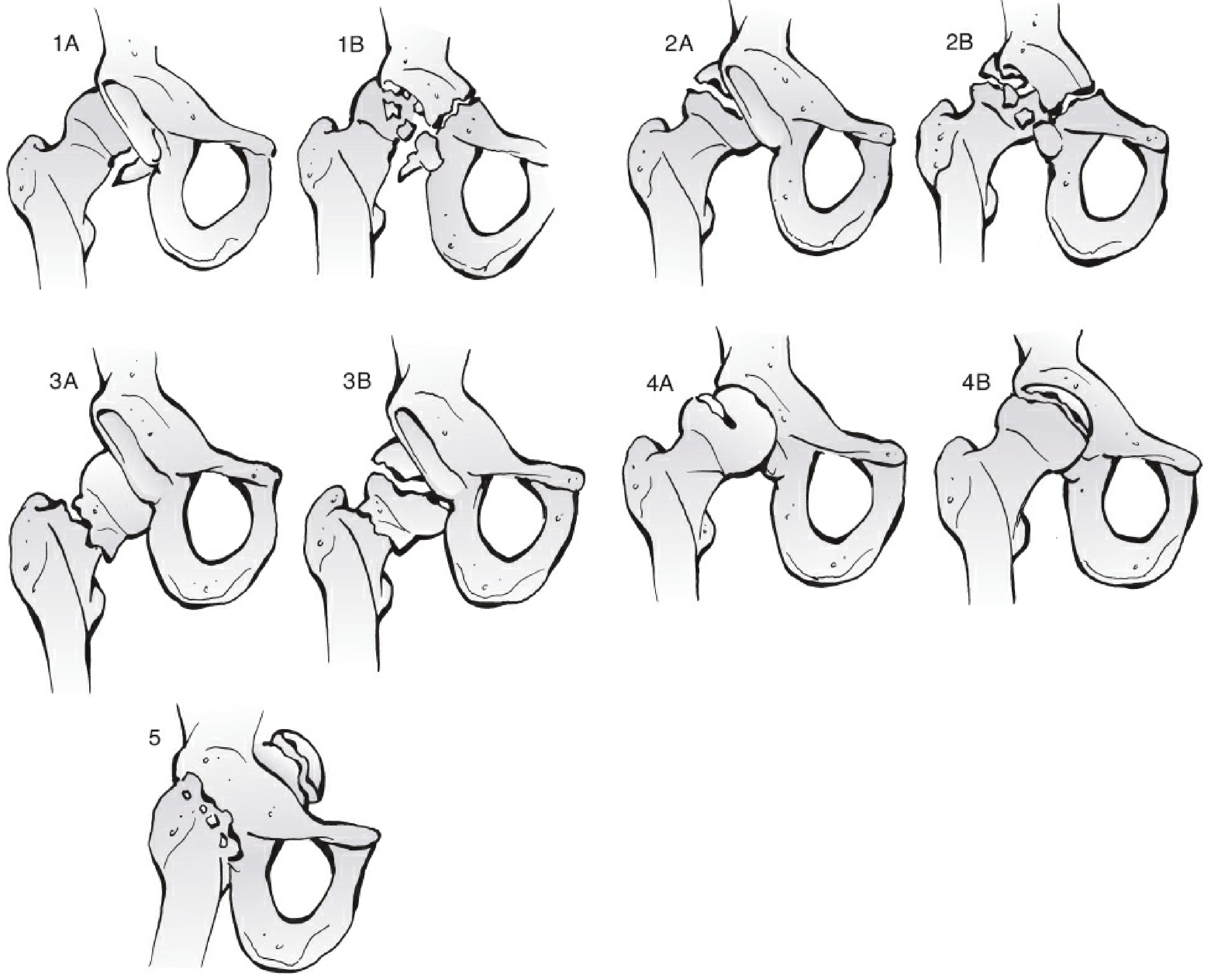
Brumback classification of hip dislocations with femoral head fractures (Rockwood & Green's, 10th Ed.)
| Type | Description |
|---|---|
| 1A | Posterior dislocation + inferomedial femoral head fracture, minimum acetabular rim fracture, stable after reduction |
| 1B | Same with significant acetabular rim fracture |
| 2A | Posterior dislocation + superomedial femoral head fracture, stable |
| 2B | Same with significant acetabular fracture and instability |
| 3A/3B | Dislocation (any direction) + femoral neck fracture, without/with femoral head fracture |
| 4A | Anterior dislocation, indentation type (superolateral depression) |
| 4B | Anterior dislocation, transchondral shear fracture |
| 5 | Central fracture-dislocation with femoral head fracture |
1B. Anterior Hip Dislocation
Mechanism: Forced abduction levers the femoral head anteriorly through a capsular tear.
- Superior (pubic/subspinous): Hip extended at time of injury
- Inferior (obturator): Hip flexed at time of injury
Clinical presentation:
- Limb in abduction and external rotation (opposite of posterior)
- Femoral artery or nerve injury possible - full neurovascular exam required
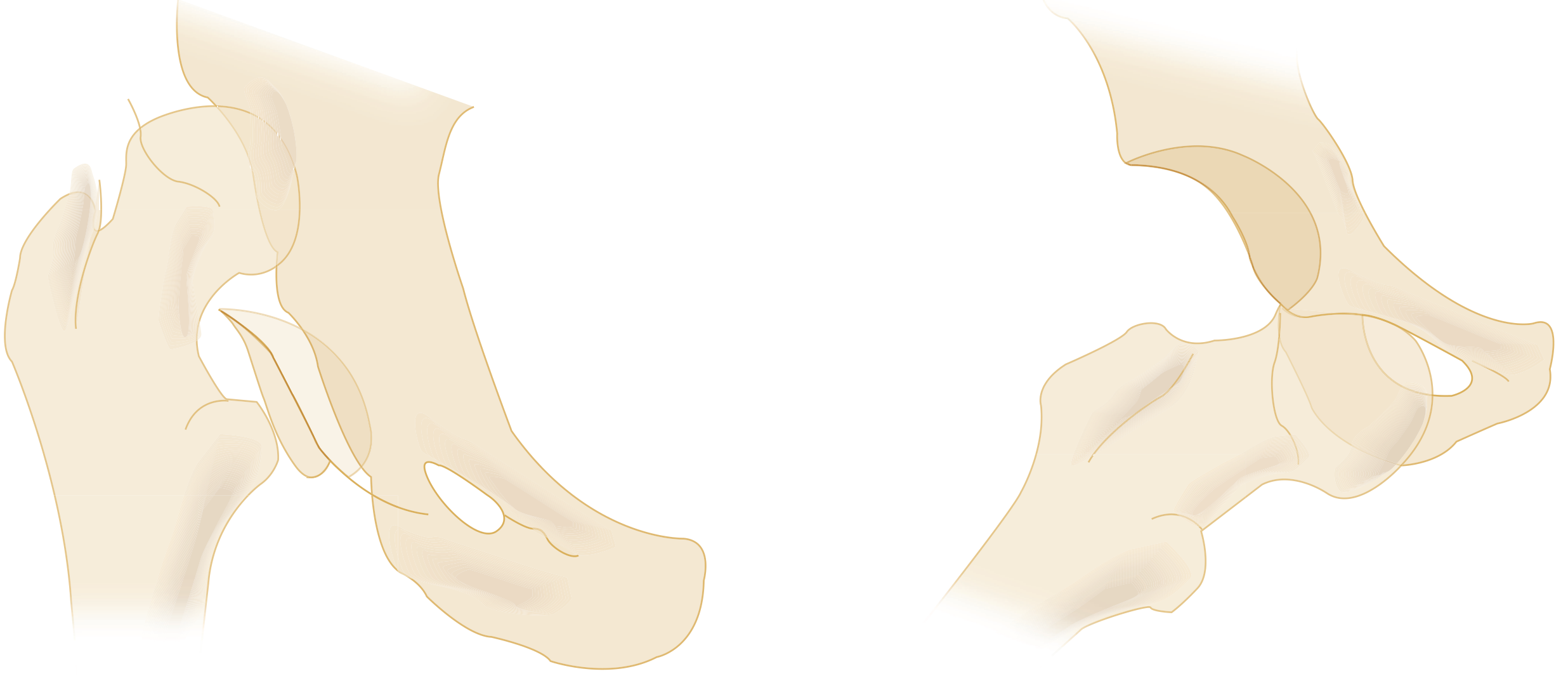
Left: anterior superior dislocation. Right: anterior inferior (obturator) dislocation (Tintinalli's)
Management: Anterior hip dislocations mandate reduction in the OR under general anesthesia.
Indications for Open Reduction
- Failed closed reduction
- Unsatisfactory reduction
- Complex fracture-dislocations
- Irreducible dislocations
PART 2 - DISPLACED FRACTURES OF THE HIP
Anatomy of Fracture Sites
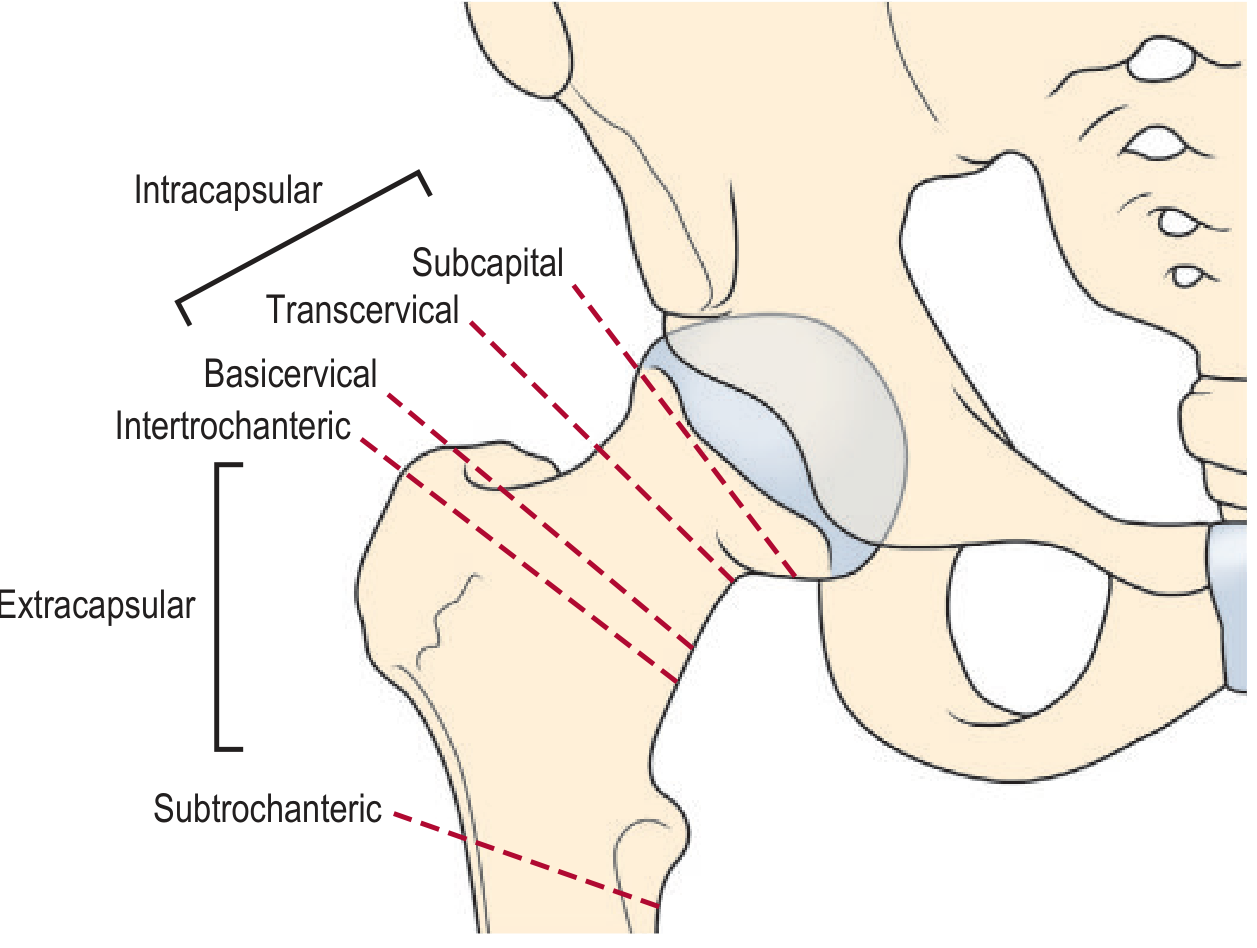
Proximal femoral fracture sites with intracapsular vs. extracapsular zones (Grainger & Allison's)
Key distinction:
| Zone | Fracture Types | AVN Risk |
|---|---|---|
| Intracapsular | Subcapital, transcervical, basicervical | HIGH (blood supply to femoral head at risk) |
| Extracapsular | Intertrochanteric, subtrochanteric | Lower (blood supply preserved) |
2A. Femoral Neck Fractures (Intracapsular)
The blood supply to the femoral head runs via recurrent arteries closely applied to the femoral neck. Displaced intracapsular fractures disrupt this supply.
- AVN risk: 15-35% with displaced intracapsular fractures
- ~15% of fractures are radiographically subtle initially
- Occult fractures: if weight-bearing is limited at 24 hours, MRI is the investigation of choice (specific and sensitive)
Garden Classification of Intracapsular Fractures:
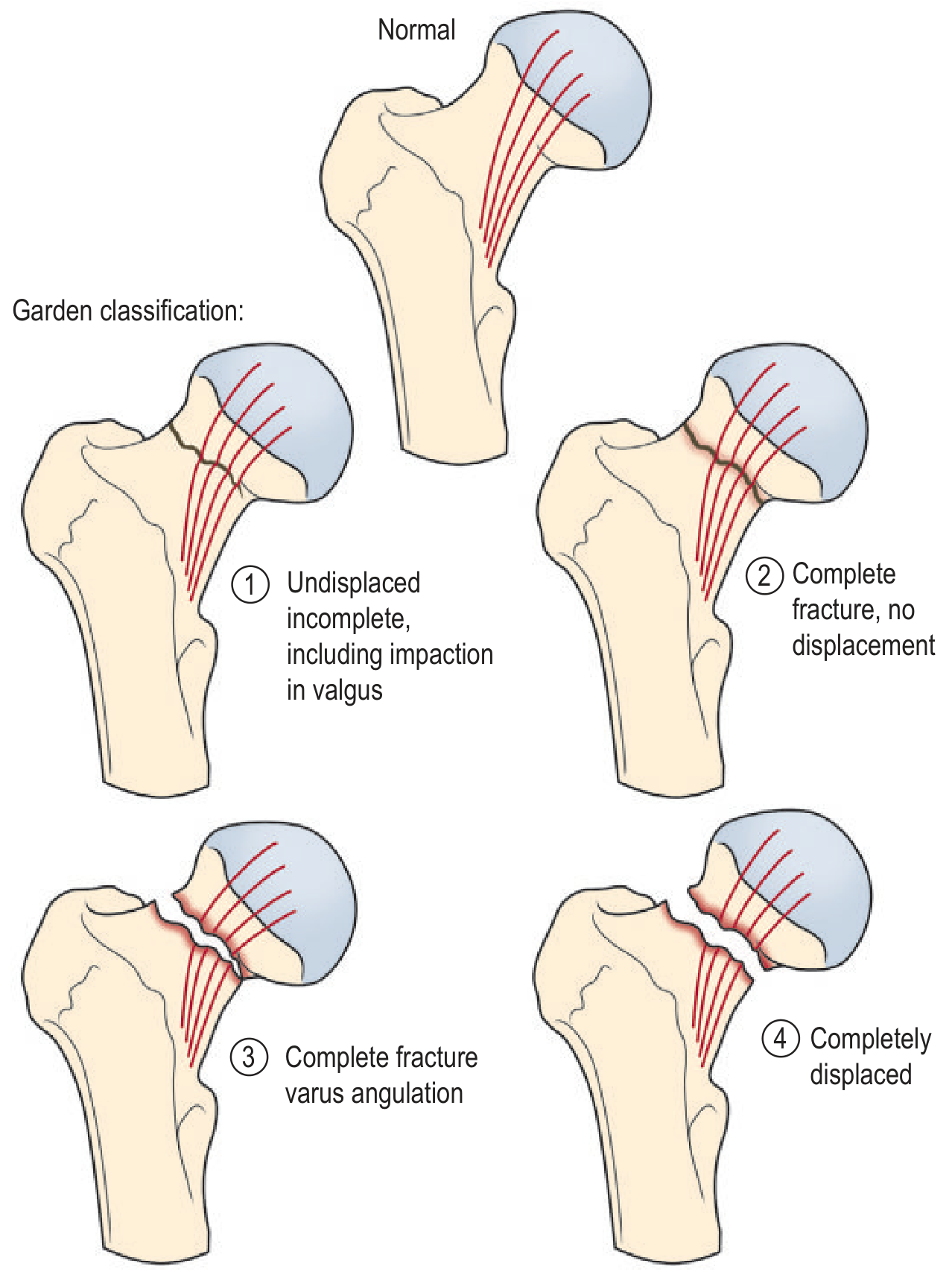
Garden Classification (Grainger & Allison's Diagnostic Radiology)
| Stage | Description |
|---|---|
| 1 | Undisplaced incomplete (including valgus impaction) |
| 2 | Complete fracture, no displacement |
| 3 | Complete fracture, varus angulation |
| 4 | Completely displaced |
Garden 3 and 4 carry the highest AVN risk as the blood supply is almost inevitably interrupted (particularly in displaced subcapital fractures).
Treatment:
- Garden 1 & 2 (undisplaced): Internal fixation with dynamic hip screw or multiple cannulated screws (especially in patients <60 who were independently mobile)
- Garden 3 & 4 (displaced): Hemiarthroplasty; or total hip replacement in patients who were independently mobile before fracture
- Interruption of trabecular lines on X-ray = subtle fracture; use lateral view and MRI to confirm
2B. Intertrochanteric Fractures (Extracapsular)
- Run between the greater and lesser trochanters
- Blood supply is preserved - lower AVN risk
- Can be treated with plate and dynamic screw fixation or intramedullary nailing
- Severely comminuted fractures are easily identified on X-ray
- Subtle/minimally displaced fractures may be missed - air trapped in skin crease of groin can mimic or mask a fracture
- Approximately 1% are initially occult on plain X-ray; if not detected and patient mobilizes, fracture may displace
2C. Subtrochanteric Fractures (Extracapsular)
- Below the lesser trochanter, extracapsular
- Treated by intramedullary nailing
- Lower AVN risk compared to intracapsular fractures
PART 3 - COMPLICATIONS
| Complication | Associated With | Timing |
|---|---|---|
| Avascular necrosis (AVN) | Posterior dislocation; displaced subcapital fractures | Weeks-months |
| Sciatic nerve injury | Posterior dislocation | Acute (~10%) |
| Femoral nerve/artery injury | Anterior dislocation | Acute |
| Post-traumatic arthritis | Any fracture-dislocation | Late |
| Fracture displacement | Occult undisplaced fractures if mobilized | Early |
- AVN risk from hip dislocation increases from <10% at <10 hours delay to ~25% at 15 hours delay
- Outcomes are measured with Harris Hip Score, WOMAC, and Merle d'Aubigne scores; overall health with SF-12 and SMFA
Summary Table
| Injury | Mechanism | Position of Limb | Key Complication | Treatment |
|---|---|---|---|---|
| Posterior dislocation | Dashboard (flexed knee) | Short, adducted, internally rotated | AVN, sciatic nerve injury | Closed reduction (6 hrs), OR if failed |
| Anterior dislocation | Forced abduction | Abducted, externally rotated | Femoral nerve/vessel | Open reduction in OR |
| Displaced subcapital (Garden 3/4) | Low-energy fall (elderly) | Externally rotated, shortened | AVN (15-35%) | Hemiarthroplasty or THA |
| Undisplaced femoral neck (Garden 1/2) | Variable | May be minimal | Fracture displacement if missed | Internal fixation |
| Intertrochanteric | Low energy (elderly) | Externally rotated | Less AVN risk | DHS or IMN |
| Subtrochanteric | High energy | Variable | Deformity, delayed union | IMN |
Sources: Tintinalli's Emergency Medicine (9th Ed.) - pp. 1888-1891; Rockwood & Green's Fractures in Adults (10th Ed. 2025) - pp. 2574-2579; Grainger & Allison's Diagnostic Radiology - pp. 1162-1163; Roberts & Hedges' Clinical Procedures in Emergency Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.