Late night food consumption patient came to me with acute right side iliac pain, what is the possible diagnosis?
Reading File
search_medical_text
acute right iliac fossa pain differential diagnosis
search_medical_text
appendicitis late night food consumption abdominal pain diagnosis
search_medical_image
right iliac fossa pain appendicitis differential diagnosis
GradeResponse
GradeResponse
GradeResponse
Acute Right Iliac Fossa (RIF) Pain with Late-Night Food Consumption
Given the clinical context — acute right iliac fossa pain following late-night food consumption — here are the possible diagnoses ranked by likelihood:
🔴 Most Likely Diagnosis: Acute Appendicitis
This is the top diagnosis to rule out first. Late-night heavy eating can increase intestinal peristalsis and luminal pressure, potentially triggering or exacerbating appendiceal obstruction.
Clinical Features:
- Pain typically starts periumbilical, then migrates to the right iliac fossa (McBurney's point)
- Low-grade fever, nausea, anorexia
- Pointing sign — patient points to where pain started vs. where it moved
- On examination: localised tenderness, muscle guarding, rebound tenderness in RIF
- Positive Rovsing's sign, Psoas sign, Obturator sign
"The diagnosis of appendicitis rests more on thorough clinical examination of the abdomen than on any aspect of the history or laboratory investigation." — Bailey & Love's Surgery, 28th Ed., p. 1360
Laparoscopic View: Appendicitis vs. Caecal Diverticulitis
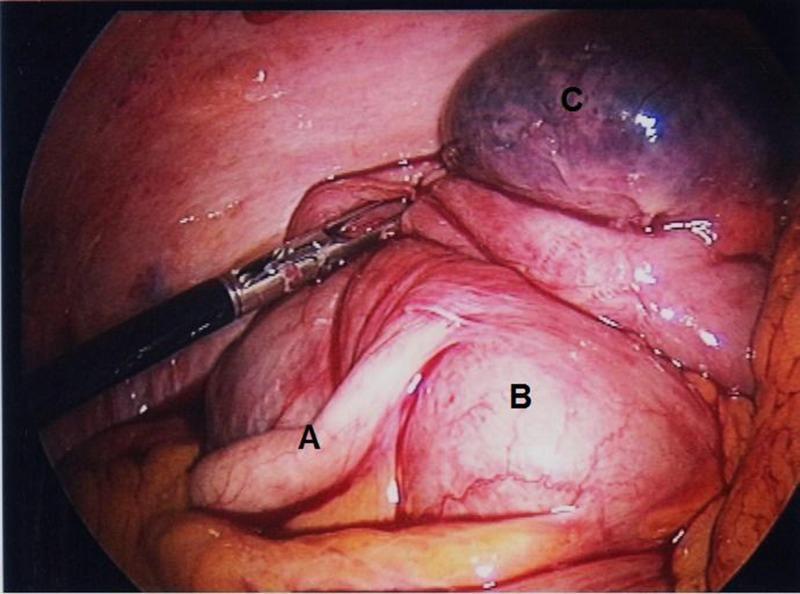
This intraoperative image illustrates the importance of differentiating appendicitis from solitary caecal diverticulitis — both present identically clinically.
Full Differential Diagnosis Table
| Diagnosis | Key Distinguishing Features | Relation to Food |
|---|---|---|
| Acute Appendicitis | Migratory pain to RIF, fever, rebound tenderness, guarding | Indirect (increased peristalsis) |
| Caecal/Meckel's Diverticulitis | Clinically identical to appendicitis; found intraoperatively | Similar mechanism |
| Mesenteric Lymphadenitis | Younger patients, often post-viral URTI; less guarding | Not directly related |
| Ileocaecal Tuberculosis | Chronic low-grade fever, weight loss, mass in RIF | Not related |
| Crohn's Disease (Terminal Ileitis) | Recurrent episodes, diarrhea, weight loss | Exacerbated by food |
| Irritable Bowel Syndrome (IBS) | Colicky pain, altered bowel habits, no fever | Strongly food-triggered |
| Gastroenteritis | Diffuse cramps, vomiting, diarrhea | Directly food-related |
| Rectus Sheath Haematoma | Post-exertion or trauma, localised without GI upset | Not food-related |
| Psoas Abscess | Gradual onset, fever, pain on hip extension | Not related |
| Right Ureteric Colic | Colicky, radiates to groin, hematuria | Not food-related |
| Ovarian Pathology (females) | Ovarian cyst torsion/rupture; cyclical or sudden pain | Not food-related |
| Ectopic Pregnancy (females) | Amenorrhoea, positive β-hCG, haemodynamic instability | Not food-related |
Recommended Workup
- History: Onset, character, radiation, associated symptoms (nausea, vomiting, fever, diarrhea, urinary symptoms, LMP in females)
- Examination: McBurney's point tenderness, Rovsing's, Psoas, Obturator signs
- Labs: CBC (leukocytosis), CRP, urinalysis, β-hCG (females), LFTs
- Imaging:
- Ultrasound abdomen — first-line (non-compressible appendix >6mm = appendicitis)
- CT abdomen/pelvis (with contrast) — gold standard if USS inconclusive
- Alvarado/MANTRELS Score — use to stratify appendicitis risk
"Solitary caecal diverticulitis can masquerade as acute appendicitis — the diagnosis is often made intraoperatively." — PMC Clinical VQA
Bottom Line
In a patient with acute RIF pain following late-night food consumption, acute appendicitis must be excluded urgently. Food-triggered abdominal pain in the RIF should also raise suspicion for IBS, gastroenteritis, or Crohn's disease — but none of these can be assumed until appendicitis is ruled out clinically and radiologically. Prompt surgical consultation is warranted if clinical suspicion is high.
Gastroenteritis: drug of choice and gold standard to reduce the symptoms in Indian case scenario?
search_medical_text
gastroenteritis drug of choice treatment management guidelines
search_medical_text
gastroenteritis oral rehydration therapy ORS India treatment
GradeResponse
GradeResponse
search_medical_text
acute gastroenteritis antibiotic zinc probiotics treatment adults
search_medical_text
infectious diarrhea antiemetic ondansetron loperamide symptomatic treatment
Gastroenteritis: Drug of Choice & Gold Standard Management (Indian Context)
🥇 Gold Standard: Oral Rehydration Therapy (ORT)
The absolute cornerstone of gastroenteritis management — in India and globally — is rehydration, not antibiotics.
"Reduced osmolarity ORS is recommended as the first-line therapy of mild to moderate dehydration in infants, children, and adults with acute diarrhea from any cause." — Diagnosis and Management of Infectious Diarrhea, p. 9
WHO/UNICEF Low-Osmolarity ORS (the standard in India via government health programs):
| Component | Amount per litre |
|---|---|
| Sodium chloride | 2.6 g |
| Trisodium citrate | 2.9 g |
| Potassium chloride | 1.5 g |
| Glucose (anhydrous) | 13.5 g |
| Osmolarity | 245 mOsm/L |
In India, WHO-ORS sachets are freely distributed through ASHA workers, PHCs, and anganwadi centres under national diarrheal disease control programs.
Home-based ORS alternative (widely used in rural India):
- 1 litre boiled/cooled water + 6 level teaspoons sugar + ½ teaspoon salt
💊 Drug of Choice — By Symptom & Cause
1. Rehydration (All Cases)
- Mild–Moderate: Oral ORS (low-osmolarity)
- Moderate with vomiting: Nasogastric ORS
- Severe dehydration: IV Ringer's Lactate or Normal Saline
2. Antiemetic (Vomiting Control)
- Drug of Choice: Ondansetron (5-HT3 antagonist)
- Dose: 4–8 mg orally/IV
- Reduces vomiting, improves ORS tolerance
- Preferred over metoclopramide (fewer extrapyramidal side effects)
- Widely available and affordable in India (generic brands: Emeset, Ondem)
3. Anti-diarrheal
- Loperamide — for non-bloody, non-febrile diarrhea in adults
- Reduces stool frequency; contraindicated in dysentery and children <2 years
- Racecadotril (Acetorphan) — increasingly preferred in India
- Antisecretory, does not inhibit motility; safer than loperamide, especially in children
4. Zinc Supplementation (India-specific — National Program)
| Population | Dose | Duration |
|---|---|---|
| Children <5 years | 20 mg/day | 10–14 days |
| Infants 2–6 months | 10 mg/day | 10–14 days |
Zinc is officially recommended by IAP (Indian Academy of Pediatrics) and IMNCI guidelines for all diarrheal episodes in children. It reduces severity, duration, and recurrence risk.
5. Antibiotics (Selective Use Only)
Antibiotics are NOT routine for gastroenteritis. Use only when:
| Indication | Drug of Choice |
|---|---|
| Cholera (Vibrio cholerae) — endemic in India | Doxycycline 300 mg single dose (adults) |
| Shigella/Bacillary dysentery | Azithromycin or Ciprofloxacin |
| Traveller's diarrhea (E. coli) | Azithromycin 500 mg OD × 3 days |
| Giardiasis (common in India) | Metronidazole 400 mg TDS × 5–7 days |
| Entamoeba histolytica (amoebic dysentery) | Metronidazole + Diloxanide furoate |
| Typhoid (enteric fever) | Ceftriaxone / Azithromycin (due to fluoroquinolone resistance in India) |
6. Probiotics (Adjunct in Indian Practice)
- Lactobacillus rhamnosus GG and Saccharomyces boulardii — evidence-supported
- Commonly prescribed in India as adjuncts (Darolac, Vizylac, Bifilac)
- Reduce diarrhea duration by ~1 day
Summary Algorithm (Indian Setting)
Acute Gastroenteritis
↓
Assess dehydration severity
↓
Mild–Moderate → ORS (WHO low-osmolarity) + Zinc (children)
Severe → IV Ringer's Lactate
↓
Vomiting? → Ondansetron
↓
Bloody stool / High fever / No improvement in 48h?
→ Stool culture → Targeted antibiotics
↓
Children < 5 yrs → Zinc mandatory (IAP/IMNCI guideline)
↓
Probiotics as adjunct (optional)
Key India-Specific Points
- Cholera and typhoid remain endemic in several states — always consider in rural/peri-urban patients
- Metronidazole is heavily used empirically due to high prevalence of amoebic and giardial infections
- Fluoroquinolone resistance (especially in Salmonella Typhi) is a major concern — azithromycin and ceftriaxone are now preferred
- Zinc + ORS combo is the national standard for pediatric diarrhea under IMNCI and Integrated Action Plan for Pneumonia and Diarrhoea (IAPPD)
This is a shared conversation. Sign in to Orris to start your own chat.