Explain me 10 common heart diseases with images of ECG changes of diseases
Reading File
Finding Sources
Searching the Web
common heart diseases ECG changes with images explained
Finding Sources
Searching the Web
ECG changes atrial fibrillation heart block ventricular tachycardia STEMI site:litfl.com OR site:ecglibrary.com
Finding Sources
Reading Web Page
https://litfl.com/inferior-stemi-ecg-library
Reading File
Searching the Web
ECG images STEMI atrial fibrillation heart block WPW long QT pericarditis hypertrophic cardiomyopathy site:litfl.com
Finding Sources
Loading Image
Finding Sources
Loading Image
Finding Sources
Finding Sources
Loading Image
Loading Image
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Searching the Web
pericarditis long QT syndrome Wolff-Parkinson-White left ventricular hypertrophy ventricular fibrillation ECG 12 lead images
Loading Image
Loading Image
Here is a comprehensive guide to 10 common heart diseases with their ECG changes, illustrated with textbook images:
10 Common Heart Diseases and Their ECG Changes
1. ST-Elevation Myocardial Infarction (STEMI)
Disease Overview: STEMI occurs when a coronary artery is completely occluded, causing transmural (full-thickness) myocardial ischemia and necrosis. It is a medical emergency requiring immediate reperfusion therapy.
ECG Changes:
- Hyperacute T waves - earliest sign (tall, broad, peaked T waves)
- ST elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in precordial leads
- Pathological Q waves - develop within hours (>40 ms wide and >25% of R wave height), indicating necrosis
- T wave inversion - follows the ST elevation as the infarct evolves
- Reciprocal ST depression in leads opposite to the infarct zone
Territory-Lead Correlation:
- Anterior STEMI: V1-V4 (LAD occlusion)
- Inferior STEMI: II, III, aVF (RCA or LCx occlusion)
- Lateral STEMI: I, aVL, V5-V6
ECG - Anterior STEMI (ST elevation in V1-V4):
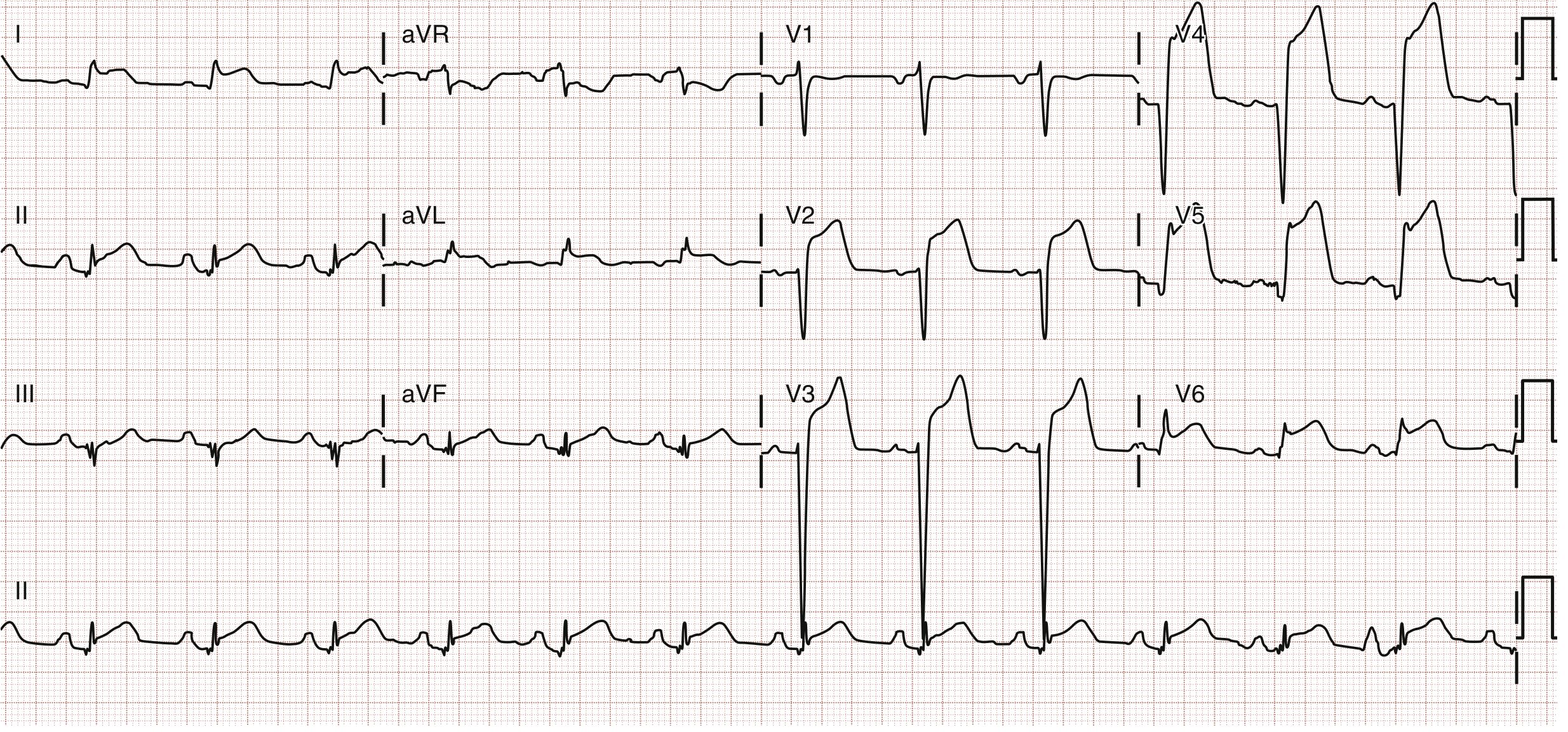
Fig. 64.6 - Anterior wall STEMI. ST elevation is prominent in leads V1 to V4. Emergency catheterization revealed 90% LAD stenosis. (Source: Rosen's Emergency Medicine)
ECG - Anterolateral STEMI showing irregularly irregular response consistent with prior STEMI (ST/T changes across V2-V6, I, aVL):
Anterolateral STEMI with STE in V2-V6, I, and aVL. (Source: Rosen's Emergency Medicine)
2. Atrial Fibrillation (AF)
Disease Overview: AF is the most common sustained cardiac arrhythmia, characterized by chaotic, rapid atrial depolarizations (350-600/min). It causes loss of coordinated atrial contraction, increasing risk of stroke, heart failure, and hemodynamic compromise.
Causes: Hypertension, valvular disease, coronary artery disease, thyrotoxicosis, alcohol ("holiday heart"), heart failure.
ECG Changes:
- Absent P waves - replaced by chaotic fibrillatory baseline (f waves), best seen in V1 and lead II
- Irregularly irregular R-R intervals - the hallmark (no two R-R intervals are equal)
- Narrow QRS complexes (unless aberrant conduction or bundle branch block is present)
- Variable ventricular rate - typically 100-180 bpm if uncontrolled
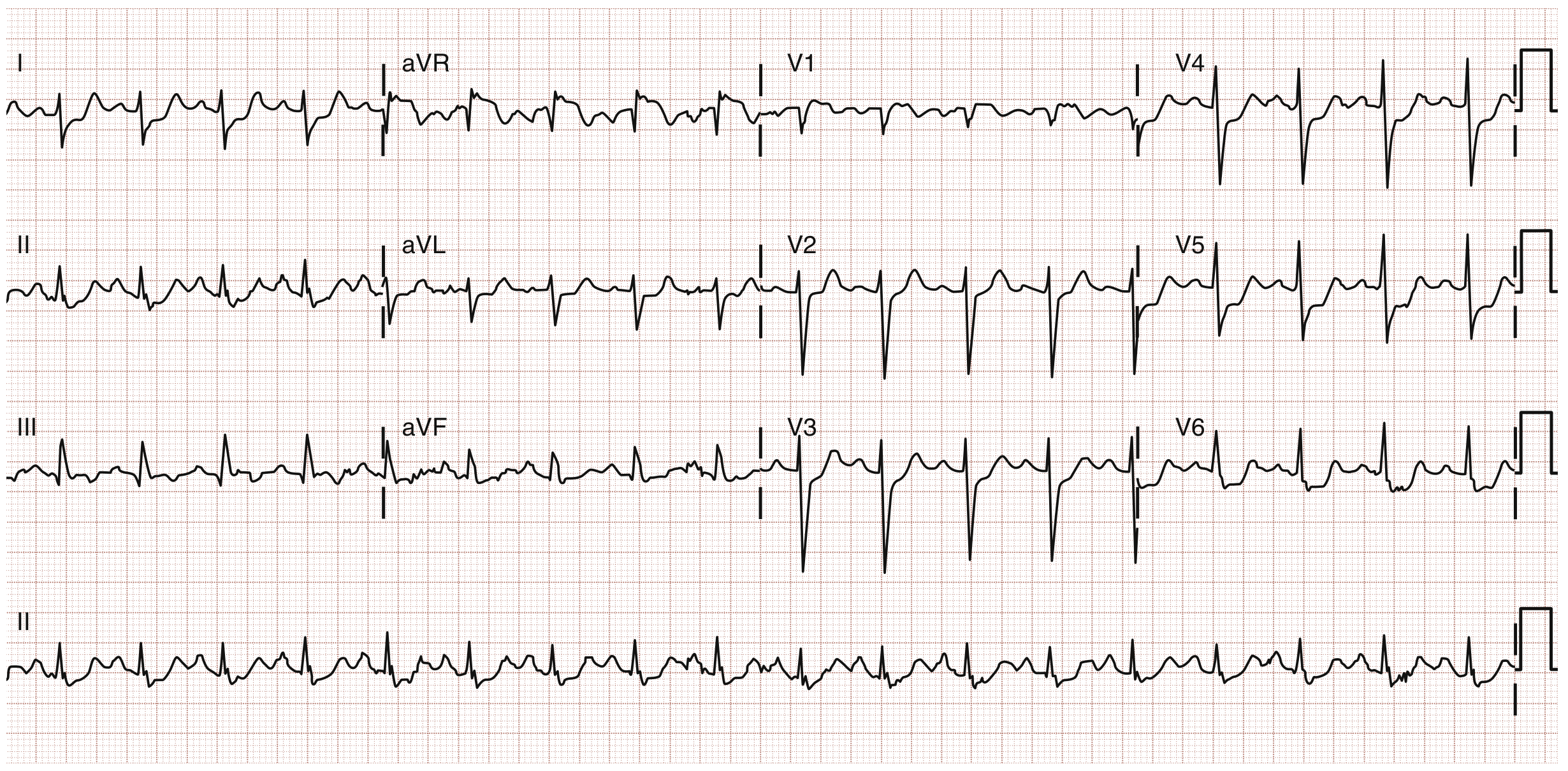
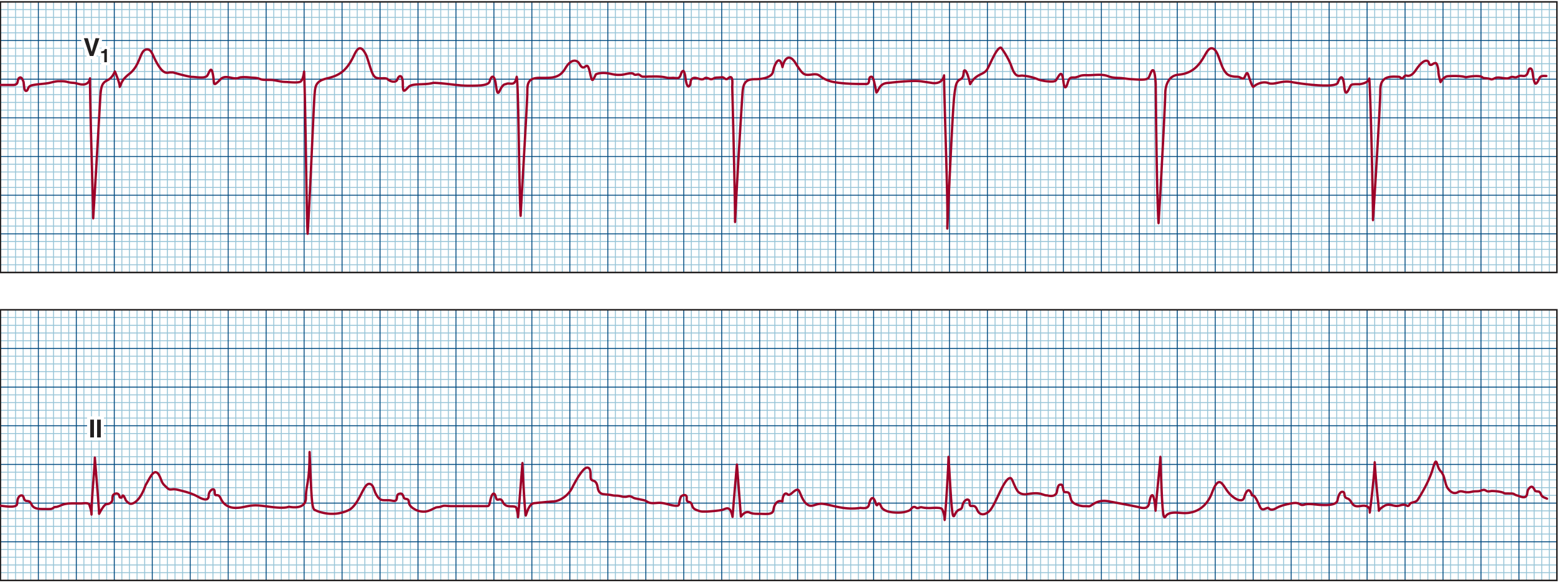
ECG - Atrial Fibrillation (irregularly irregular rhythm, no discernible P waves):
ECG of an irregularly irregular heart rhythm without discernible P waves. The disorganized atrial activation is best seen in lead V1. (Source: Goldman-Cecil Medicine)
ECG - PAC initiating AF:
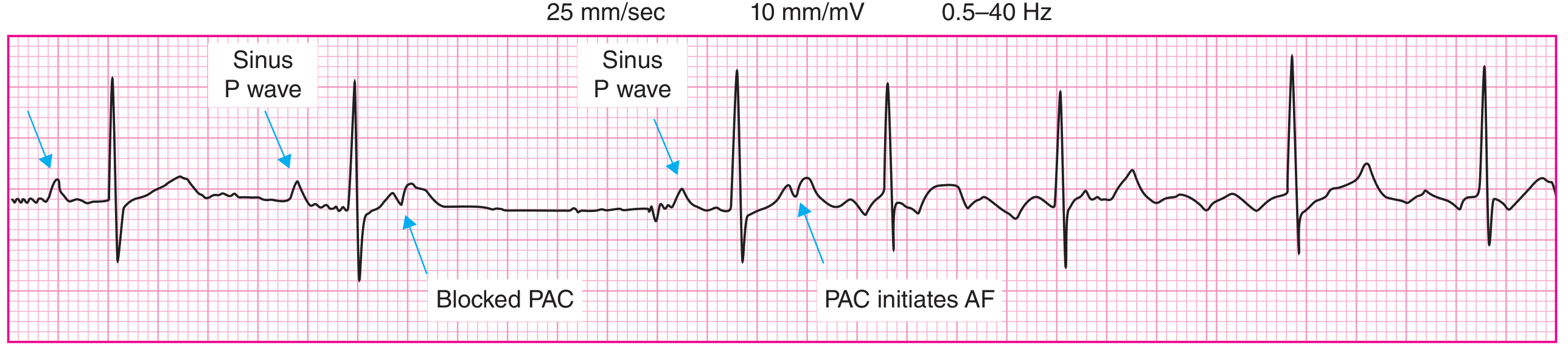
Surface ECG: sinus beats followed by a blocked PAC, then a PAC initiating atrial fibrillation with subsequent chaotic atrial activity and irregular ventricular response. (Source: Goldman-Cecil Medicine)
3. Complete Heart Block (Third-Degree AV Block)
Disease Overview: Complete dissociation between atrial and ventricular electrical activity. The AV node or His-Purkinje system fails entirely to conduct impulses from the atria to the ventricles. The ventricles are driven by a slow escape rhythm.
Causes: Idiopathic fibrosis (most common in adults), inferior STEMI (RCA occlusion), Lyme disease, drugs (beta-blockers, digoxin toxicity, calcium channel blockers), cardiac sarcoidosis.
ECG Changes:
- P waves and QRS complexes are completely independent (AV dissociation) - P waves "march through" at their own rate (60-100 bpm)
- Slow ventricular escape rhythm:
- Junctional escape (narrow QRS): 40-60 bpm
- Ventricular escape (wide QRS): 20-40 bpm - indicates block below the His bundle
- P rate > QRS rate always
- No relationship between P waves and QRS complexes
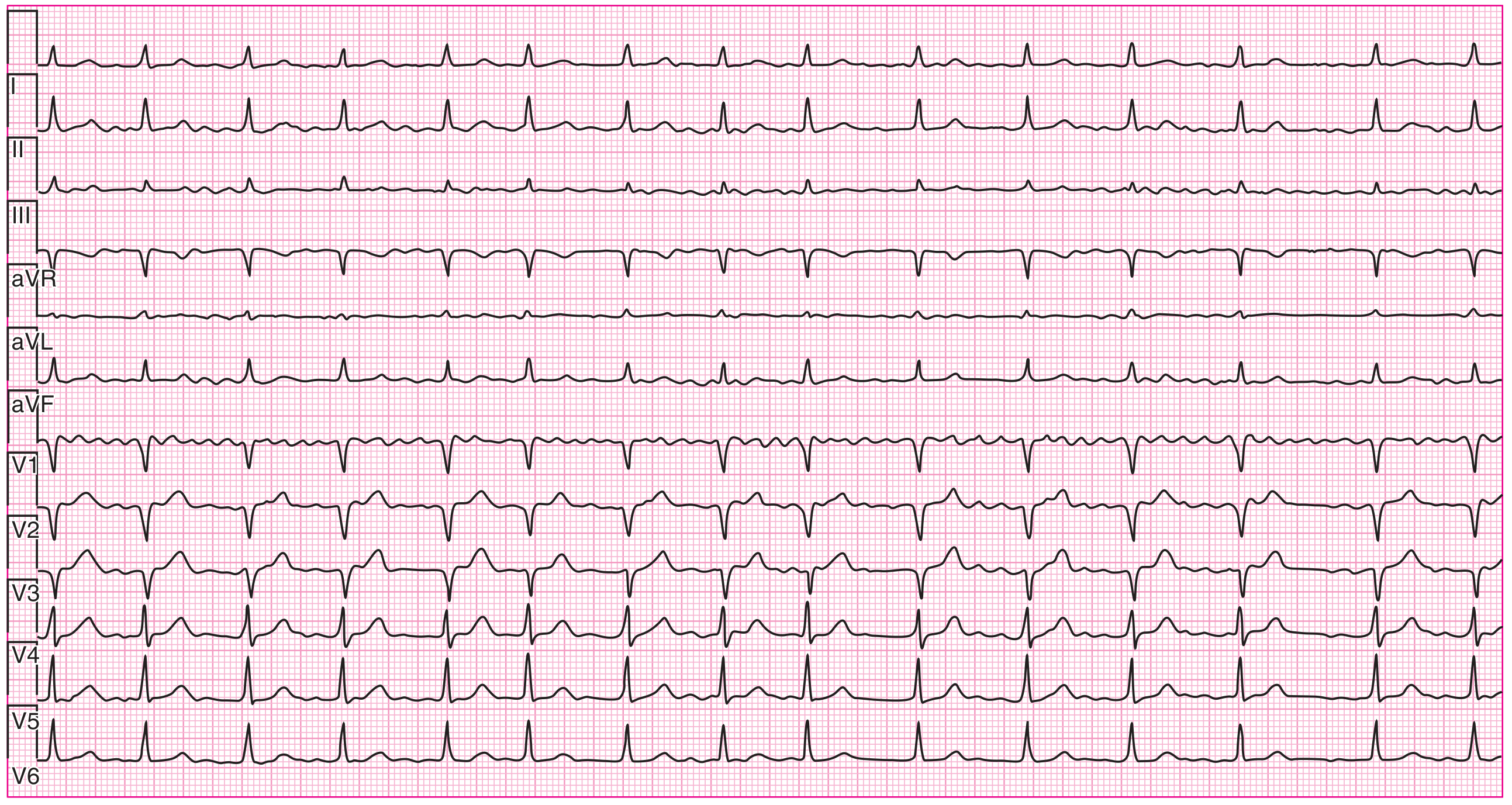
ECG - Complete Heart Block with narrow complex escape (junctional):
Complete heart block. Surface leads show complete heart block with a narrow complex escape rhythm - the atria and ventricles beat independently. (Source: Harrison's Principles of Internal Medicine)
4. Ventricular Tachycardia (VT)
Disease Overview: VT is a potentially life-threatening arrhythmia with 3 or more consecutive ventricular beats at ≥100 bpm, originating from the ventricles. Most commonly occurs in the setting of ischemic heart disease, cardiomyopathy, or electrolyte disturbances.
ECG Changes:
- Wide complex tachycardia - QRS duration >120 ms (usually >160 ms)
- Rate: 100-250 bpm
- AV dissociation - P waves independent of QRS (key diagnostic feature)
- Fusion beats and capture beats - pathognomonic when present
- Concordance across precordial leads (all positive or all negative)
- Morphology criteria: RBBB or LBBB morphology depending on origin
Differentiating VT from SVT with aberrancy: VT is more likely with:
- AV dissociation
- QRS >160 ms
- Northwest axis (-90° to ±180°)
- History of structural heart disease
ECG - Ventricular Tachycardia (long-term monitor, showing nonsustained VT run):
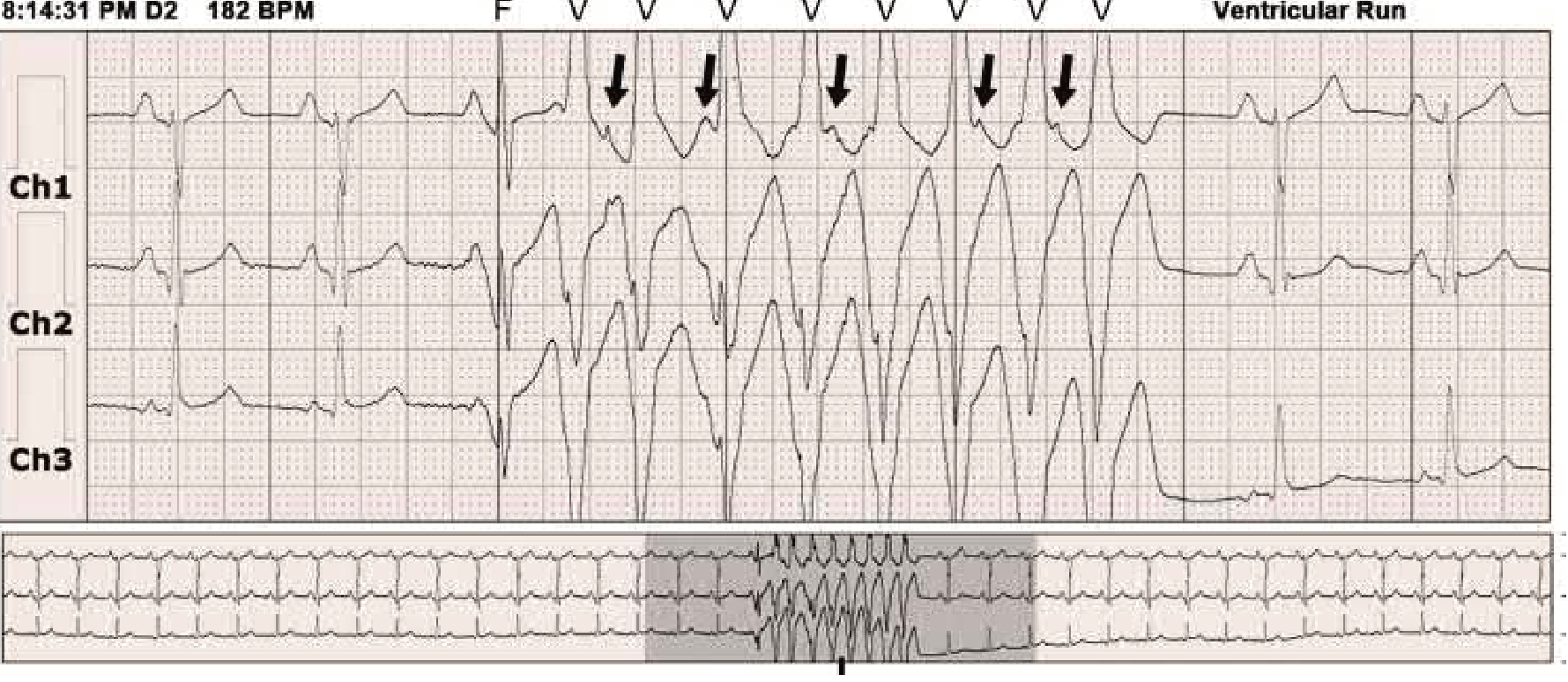
Three-channel monitor showing sinus rhythm followed by 9 wide QRS complexes of VT (labeled "V"), with a fusion beat (F) at onset. Arrows indicate retrograde P waves. Fewer P waves than QRS complexes and a fusion complex confirm VT. (Source: Braunwald's Heart Disease)
5. Ventricular Fibrillation (VF)
Disease Overview: VF is disorganized, chaotic ventricular electrical activity resulting in no effective cardiac output. It is the most common cause of sudden cardiac death and requires immediate defibrillation.
Causes: Acute MI (most common), severe electrolyte disturbances, hypothermia, drug toxicity, long QT syndrome.
ECG Changes:
- Completely chaotic, irregular waveforms - no identifiable P waves, QRS complexes, or T waves
- Irregular, rapid undulations of varying amplitude and frequency (>300 bpm chaotic)
- Coarse VF - larger amplitude waves (more amenable to defibrillation)
- Fine VF - smaller amplitude, often a late finding indicating prolonged arrest
ECG - Progression to Ventricular Fibrillation (Holter monitor showing VF onset):

Long-term Holter monitoring showing progression from ventricular tachycardia to ventricular fibrillation (chaotic high-frequency activity) recorded between 05:23-05:24. (Source: Braunwald's Heart Disease)
6. Wolff-Parkinson-White Syndrome (WPW)
Disease Overview: A congenital preexcitation syndrome caused by an accessory conduction pathway (Bundle of Kent) that bypasses the AV node. This causes early ventricular activation (preexcitation) and predisposes to tachyarrhythmias. WPW can cause sudden cardiac death due to AF with rapid ventricular conduction through the accessory pathway.
ECG Changes (during sinus rhythm):
- Short PR interval (<120 ms) - impulse bypasses the AV node delay
- Delta wave - slurred, broad upstroke at the beginning of the QRS (preexcitation of the ventricle)
- Wide QRS complex (>120 ms) - from the combination of normal and accessory pathway conduction
- ST-T changes - secondary to abnormal depolarization
- Pseudo-Q waves (negative delta waves) in certain leads can mimic MI
During tachycardia:
- Orthodromic AVRT (most common): narrow complex, regular, fast tachycardia (retrogrades via accessory pathway)
- Antidromic AVRT: wide complex tachycardia (mimics VT)
- AF with WPW: extremely rapid, irregular, wide-complex tachycardia (delta waves seen) - DANGEROUS
Key ECG Features to Remember:
| Feature | Finding |
|---|---|
| PR interval | <120 ms |
| Delta wave | Slurred QRS onset |
| QRS duration | >120 ms |
| Risk | AF→VF (avoid AV nodal blockers) |
7. Acute Pericarditis
Disease Overview: Inflammation of the pericardium, most commonly viral (Coxsackievirus). Presents with sharp pleuritic chest pain, relieved by sitting forward. Can cause pericardial effusion.
ECG Changes (4 classic stages):
- Stage 1 (hours to days): Diffuse concave-up ("saddle-shaped") ST elevation in nearly all leads (except aVR and V1), with PR depression - the hallmark
- Stage 2 (days): ST normalization, PR depression persists
- Stage 3 (1-3 weeks): Diffuse T wave inversion
- Stage 4 (weeks to months): ECG returns to normal
Key distinguishing features from STEMI:
- ST elevation in pericarditis is diffuse (multiple territories), not focal
- Concave ("saddle-shaped") ST morphology (vs. convex in STEMI)
- PR depression in II, aVF, and V4-V6 (virtually pathognomonic)
- No reciprocal changes (except aVR which shows ST depression)
- No Q waves develop
8. Heart Failure with Left Ventricular Hypertrophy (LVH)
Disease Overview: LVH develops as a compensatory response to chronic pressure overload (hypertension, aortic stenosis) or volume overload. It independently increases the risk of arrhythmias, sudden cardiac death, and myocardial ischemia.
ECG Changes:
- Increased QRS voltage - the primary feature
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm
- R in aVL ≥11 mm
- Cornell criteria: S in V3 + R in aVL >28 mm (men) or >20 mm (women)
- Left axis deviation (-30° or more)
- "LVH strain" pattern: asymmetric ST depression and T wave inversion in lateral leads (I, aVL, V5-V6) - indicates "pressure overload"
- Prolonged QRS duration (up to 110-120 ms)
- Tall R waves in lateral leads (I, aVL, V5-V6)
- Deep S waves in right precordial leads (V1-V2)
- Left atrial enlargement (P mitrale): notched P waves in II, biphasic P in V1
9. Long QT Syndrome (LQTS)
Disease Overview: A disorder of cardiac repolarization resulting in a prolonged QT interval, predisposing to a characteristic polymorphic VT called Torsades de Pointes (TdP), which can degenerate into VF and cause sudden cardiac death. Can be congenital (LQT1-13) or acquired (drugs, electrolyte disturbances).
ECG Changes:
- Prolonged QTc interval (corrected for heart rate using Bazett formula: QT/√RR)
- Abnormal: QTc >440 ms (men), >460 ms (women)
- High risk: QTc >500 ms
- T wave abnormalities depending on subtype:
- LQT1: broad-based T waves
- LQT2: low amplitude, notched T waves ("double-humped")
- LQT3: prolonged isoelectric segment with late-onset T wave
- Torsades de Pointes (TdP): the feared complication
- Polymorphic VT
- QRS complexes that twist around the isoelectric baseline (characteristic spiraling pattern)
- Initiated by "short-long-short" R-R interval sequence
Common acquired causes (DRUGS): antibiotics (azithromycin, fluoroquinolones), antipsychotics (haloperidol, quetiapine), antiarrhythmics (amiodarone, sotalol), hypokalemia, hypomagnesemia.
10. Hypertrophic Cardiomyopathy (HCM)
Disease Overview: A genetic disorder (usually autosomal dominant, sarcomere protein mutations) causing asymmetric LVH, dynamic outflow tract obstruction, and diastolic dysfunction. A leading cause of sudden cardiac death in young athletes. Symptoms include exertional syncope, dyspnea, and chest pain.
ECG Changes:
- Abnormal ECG in >90% of patients - the ECG is often the first clue
- Massive LVH voltage criteria (as above)
- "Giant" deeply inverted T waves in lateral leads (I, aVL, V4-V6) - most characteristic finding in the apical variant (Yamaguchi syndrome)
- Deep narrow Q waves ("septal Q waves") in lateral leads I, aVL, V5-V6 - from abnormal septal depolarization (key distinguishing feature from STEMI - narrow, not wide)
- Left axis deviation
- Left atrial enlargement
- WPW pattern occasionally (accessory pathway association)
- In apical HCM: giant T wave inversions (>10 mm deep) in V4-V6 are diagnostic
Summary Table
| Disease | Key ECG Features |
|---|---|
| STEMI | ST elevation + Q waves (territory-specific) |
| Atrial Fibrillation | Absent P waves, irregularly irregular RR |
| Complete Heart Block | P waves unrelated to QRS, slow escape rhythm |
| Ventricular Tachycardia | Wide complex tachycardia, AV dissociation |
| Ventricular Fibrillation | Chaotic undulations, no QRS/P/T |
| WPW Syndrome | Short PR, delta wave, wide QRS |
| Acute Pericarditis | Diffuse saddle ST elevation, PR depression |
| LVH / Heart Failure | High voltage, lateral strain, LAE |
| Long QT Syndrome | QTc >500 ms, T wave abnormalities, Torsades |
| Hypertrophic Cardiomyopathy | Massive LVH, deep narrow Q waves, giant T inversions |
Sources: Braunwald's Heart Disease (10th ed.), Goldman-Cecil Medicine, Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, Costanzo Physiology, Harrison's Principles of Internal Medicine.
Clinical Note: ECG interpretation must always be correlated with the patient's clinical presentation, history, and symptoms. No ECG finding should be interpreted in isolation.
Create pdf of this
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.