Anatomy and physiology of GU system Symptomatology of urological diseases. Laboratory, instrumental and radiologic examination of the genitourinary system. Congenital anomalies of genitourinary system Trauma of genitourinary system Nonspecific infections of the genitourinary system Urinary stone disease.(Urolithiasis) Hydronephrosis. Tumors of genitourinary system. Tumors of kidneys, ureters, urinary bladder, urethra. BPH. Prostate cancer Emergency urology
anatomy physiology genitourinary system kidneys ureters bladder urethra
urological symptoms hematuria dysuria urinary retention incontinence renal colic
urolithiasis kidney stones pathophysiology types diagnosis treatment
congenital anomalies kidney ureter bladder horseshoe kidney duplex system
kidney anatomy nephron urinary tract diagram
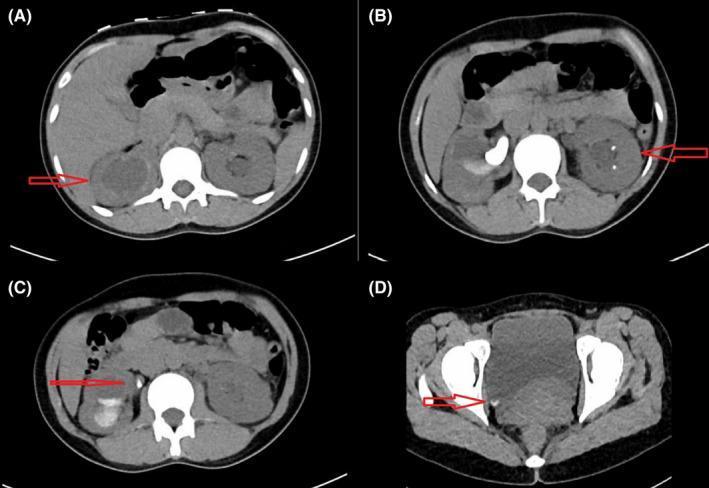
urolithiasis hydronephrosis bladder tumor imaging
Urology: Complete Study Guide
1. Anatomy & Physiology of the Genitourinary (GU) System
Upper Urinary Tract
| Structure | Key Features |
|---|---|
| Kidneys | Retroperitoneal, T12–L3; right kidney lies slightly lower than left; each ~11×6×3 cm, ~150g |
| Renal vasculature | Renal artery branches: segmental → interlobar → arcuate → interlobular → afferent arterioles |
| Nephron | ~1 million per kidney; functional unit: glomerulus + tubule |
| Renal pelvis | Funnel-shaped; receives urine from major/minor calyces |
| Ureters | 25–30 cm; three narrowing points: PUJ, pelvic brim, UVJ (most common stone lodgment sites) |
Lower Urinary Tract
| Structure | Key Features |
|---|---|
| Urinary bladder | Detrusor muscle (smooth); trigone between two ureteral orifices and internal urethral meatus |
| Urethra (male) | ~20 cm: prostatic → membranous (external sphincter) → bulbar → penile |
| Urethra (female) | ~4 cm; shorter = more prone to ascending UTI |
Physiology
- Filtration: ~180 L/day of plasma ultrafiltrate from cortical glomeruli
- Tubular modification: reabsorption (glucose, Na⁺, water) and secretion (K⁺, H⁺, drugs)
- Final urine: ~1.5–2 L/day
- Micturition reflex: bladder fills → stretch receptors activate → parasympathetic (S2–S4) → detrusor contracts + internal sphincter relaxes; somatic control via pudendal nerve (external sphincter)
- Renin-angiotensin-aldosterone axis: kidneys regulate blood pressure via juxtaglomerular apparatus
- Erythropoietin: produced by peritubular cells in cortex → stimulates RBC production
- Vitamin D activation: 1α-hydroxylation in kidney → active 1,25(OH)₂D₃
Male Reproductive Anatomy
- Testes: produce testosterone (Leydig cells) and spermatogenesis (Sertoli cells); lie in scrotum (~2°C cooler than core)
- Epididymis → vas deferens → ejaculatory duct → urethra
- Accessory glands: seminal vesicles (60% of semen volume, fructose), prostate (PSA, zinc), bulbourethral (Cowper's) glands
2. Symptomatology of Urological Diseases
Urinary Symptoms
| Symptom | Definition / Significance |
|---|---|
| Hematuria | Blood in urine; gross vs. microscopic; initial (urethral), terminal (bladder neck/prostate), total (kidney/upper tract) |
| Dysuria | Painful/burning urination; UTI, urethritis, stones |
| Frequency | >8 voids/day; UTI, OAB, BPH |
| Urgency | Sudden compelling need to void |
| Nocturia | ≥2 voids/night; BPH, heart failure, DM |
| Urinary retention | Acute (painful) or chronic (painless); BPH, neurogenic, stricture |
| Incontinence | Stress (cough/sneeze), urge, overflow, functional |
| Hesitancy / weak stream / straining | Obstructive symptoms; BPH, stricture |
| Pneumaturia / fecaluria | Vesicovaginal or enterovesical fistula |
Pain Patterns
| Location | Source |
|---|---|
| Flank / costovertebral angle (CVA) pain | Kidney (pyelonephritis, obstruction, tumor) |
| Ureteral colic | Severe colicky flank → groin → genitalia; stone |
| Suprapubic pain | Bladder, cystitis |
| Perineal / rectal pain | Prostatitis, prostatic abscess |
| Scrotal pain | Epididymo-orchitis, torsion, tumor (often painless) |
Other Symptoms
- Urethral discharge: gonorrhea (purulent), chlamydia (clear/mucoid)
- Pyuria: WBCs in urine → infection, TB, interstitial nephritis
- Pneumaturia: fistula or gas-forming organism (Enterobacter)
- Oliguria / anuria: AKI, obstruction, renal failure
Harrison's (p. 8396): "Hematuria associated with flank pain or ureteral colic is more characteristic of a lower urinary tract source, such as a stone or an obstructing lesion."
3. Laboratory, Instrumental & Radiologic Examination
Laboratory Studies
| Test | Purpose |
|---|---|
| Urinalysis (UA) | pH, SG, protein, glucose, ketones, blood, nitrites, leukocyte esterase |
| Urine microscopy | RBC casts (GN), WBC casts (pyelonephritis), granular casts (ATN), crystals |
| Urine culture & sensitivity | Gold standard for UTI |
| Urine cytology | Screening for urothelial carcinoma |
| 24-hour urine | Stone risk factors: Ca²⁺, oxalate, urate, citrate, Cr, volume |
| Serum creatinine / GFR | Renal function |
| PSA (total + free) | Prostate cancer screening; >4 ng/mL abnormal; free/total ratio <10% → malignancy |
| AFP, β-hCG, LDH | Testicular tumor markers |
| CBC, coagulation | Hematuria workup, pre-op |
Instrumental
| Procedure | Indication |
|---|---|
| Cystoscopy | Gold standard for bladder lesions, hematuria workup; allows biopsy |
| Ureteroscopy | Upper tract stones, tumors |
| Urodynamics | Evaluate bladder function; detrusor overactivity, sphincter competence |
| Transrectal US (TRUS) + biopsy | Prostate cancer diagnosis |
| Renal biopsy | Glomerular disease, transplant evaluation |
Radiologic
| Modality | Key Uses |
|---|---|
| Plain X-ray (KUB) | Radio-opaque stones (Ca oxalate, struvite, Ca phosphate); 90% of stones visible |
| Ultrasound | Hydronephrosis, renal masses, bladder residual, testicular pathology; first-line, no radiation |
| IVU / IVP | Ureteral anatomy, filling defects; largely replaced by CT |
| Non-contrast CT (NCCT/KUB) | Gold standard for urolithiasis; detects all stone types; also trauma |
| CT urography (CTU) | Hematuria workup; urothelial tumors, stones, masses |
| MRI | Soft tissue (prostate staging, renal masses); no radiation |
| Renal angiography | Renal artery stenosis, arteriovenous fistula, pre-nephrectomy |
| Radionuclide scan (DMSA, MAG3, DTPA) | Split renal function, obstruction, scarring |
| Retrograde pyelogram | Upper tract filling defects when CT inconclusive |
| Voiding cystourethrogram (VCUG) | Vesicoureteral reflux, urethral strictures |
4. Congenital Anomalies of the GU System
Renal Anomalies
| Anomaly | Features |
|---|---|
| Horseshoe kidney | Fused lower poles across midline (anterior to aorta); increased risk of stones, UPJ obstruction, Wilms tumor |
| Renal agenesis | Unilateral (compensatory hypertrophy of contralateral kidney); bilateral = Potter sequence (fatal) |
| Renal ectopia | Pelvic, iliac, thoracic; associated with UPJ obstruction |
| Duplex system | Duplex ureter; upper moiety ureter → ectopic insertion (obstructed); lower moiety → reflux (Weigert-Meyer rule) |
| UPJO (UPJ obstruction) | Most common congenital obstruction; causes hydronephrosis; Rx: pyeloplasty |
| Polycystic kidney disease | ADPKD (PKD1/PKD2 mutation) — adults; ARPKD — children; bilateral cysts |
| Multicystic dysplastic kidney | Non-functional; spontaneous involution; contralateral kidney at risk for VUR |
| Medullary sponge kidney | Dilated collecting tubules; nephrocalcinosis, stones, UTIs |
Ureteral Anomalies
| Anomaly | Features |
|---|---|
| Vesicoureteral reflux (VUR) | Grade I–V; predisposes to pyelonephritis, renal scarring; Rx: prophylactic antibiotics or ureteral reimplantation |
| Ureterocele | Cystic dilation of intravesical ureter; orthotopic or ectopic |
| Retrocaval ureter (circumcaval) | Right ureter passes behind IVC; causes right hydronephrosis |
| Ectopic ureter | Insertion below bladder neck → incontinence in females (continuous dribbling with normal voiding) |
Bladder & Urethral Anomalies
| Anomaly | Features |
|---|---|
| Bladder exstrophy | Failure of anterior bladder wall closure; exposed mucosa; associated with epispadias |
| Patent urachus | Umbilical fistula (urine from umbilicus), urachal sinus/cyst/diverticulum |
| Posterior urethral valves (PUV) | Most common obstructive uropathy in males; hypertrophied mucosal folds at verumontanum; causes bilateral hydronephrosis, bladder dysfunction; diagnosed on VCUG |
| Hypospadias | Ventral urethral meatus opening; associated with chordee; NEVER circumcise before repair |
| Epispadias | Dorsal urethral meatus; associated with bladder exstrophy |
| Cryptorchidism | Undescended testis; 30× increased risk of testicular cancer; orchidopexy by age 1 year |
| Phimosis / paraphimosis | Tight foreskin; paraphimosis is a urological emergency |
5. Trauma of the Genitourinary System
Classification by Structure
Renal Trauma (Most Common GU Injury)
- Mechanism: blunt (80%) — MVA, falls; penetrating — GSW, stab
- AAST Grade:
- I: contusion/subcapsular hematoma
- II: <1 cm laceration, no collecting system involvement
- III: >1 cm laceration, no collecting system
- IV: laceration through collecting system, or renal artery/vein injury with contained hemorrhage
- V: shattered kidney, avulsion of renal hilum
- Dx: CT with contrast (gold standard); hematuria ≠ grade of injury (>20% grade IV have no hematuria)
- Rx: Grades I–III → conservative; Grade IV-V with hemodynamic instability → angioembolization or surgery
Ureteral Trauma
- Rare; 75% iatrogenic (gynecologic surgery)
- Dx: IVP or CTU (extravasation)
- Rx: primary repair/ureteral stenting if early; ureteroureterostomy or ureteroneocystostomy
Bladder Trauma
- 90% associated with pelvic fracture
- Extraperitoneal rupture (60%): most common; pelvic hematoma confines injury; Rx: Foley catheter drainage alone
- Intraperitoneal rupture (40%): dome injury from distended bladder; Rx: surgical repair
- Dx: CT cystography (retrograde filling with 350 mL contrast); plain cystogram if CT unavailable
Urethral Trauma
- Anterior urethra (bulbar): straddle injury; perineal/scrotal hematoma; "butterfly" hematoma pattern
- Posterior urethra (membranous): associated with pelvic fractures; classic triad: inability to void, blood at meatus, high-riding prostate on DRE
- Do NOT pass Foley if posterior urethral injury suspected → retrograde urethrogram (RUG) first
- Rx: suprapubic cystostomy; delayed urethroplasty
Genital Trauma
- Penile fracture: rupture of tunica albuginea during erection; "cracking sound" + immediate detumescence + "eggplant deformity" → emergency surgical repair
- Testicular rupture: trauma; scrotal US → surgical exploration if rupture confirmed
6. Nonspecific Infections of the GU System
UTI Classification
| Type | Definition |
|---|---|
| Uncomplicated UTI | Healthy, non-pregnant women; community-acquired |
| Complicated UTI | Anatomic/functional abnormality, instrumentation, male, pregnancy, immunosuppression, MDR organisms |
| Recurrent UTI | ≥2 episodes in 6 months or ≥3 in 12 months |
Pathogens
- E. coli (80%), Klebsiella, Proteus mirabilis (urease → struvite stones), Enterococcus, Staphylococcus saprophyticus (young sexually active women)
Clinical Syndromes
| Syndrome | Features | Management |
|---|---|---|
| Acute cystitis | Dysuria, frequency, urgency, suprapubic pain; no fever | TMP-SMX 3 days or nitrofurantoin 5 days or fosfomycin single dose |
| Acute pyelonephritis | Fever, rigors, CVA tenderness, nausea/vomiting; may have lower tract symptoms | Fluoroquinolone 7–14 days; IV if severe (ceftriaxone/aminoglycoside) |
| Urethritis | Dysuria, discharge; non-gonococcal (chlamydia) vs. gonococcal | Ceftriaxone + azithromycin/doxycycline |
| Prostatitis | See below | |
| Epididymo-orchitis | Scrotal pain/swelling, fever; <35yo → STI (chlamydia/gonorrhea); >35yo → gram-negative rods | Age-appropriate antibiotics |
Prostatitis Classification (NIH)
| Category | Type | Features |
|---|---|---|
| I | Acute bacterial | Fever, dysuria, tender boggy prostate; Do NOT massage; IV antibiotics |
| II | Chronic bacterial | Recurrent UTIs, same organism; fluoroquinolone 4–6 weeks |
| III | Chronic pelvic pain syndrome (CPPS) | Most common; no infection; multimodal Rx |
| IV | Asymptomatic inflammatory | Incidental finding |
Fournier's Gangrene
- Necrotizing fasciitis of perineum/genitalia
- Polymicrobial; diabetics, immunocompromised
- Emergency: aggressive surgical debridement + broad-spectrum antibiotics + ICU
- High mortality (20–40%)
7. Urinary Stone Disease (Urolithiasis)
Stone Composition
| Type | Frequency | Radiopacity | Risk Factors |
|---|---|---|---|
| Calcium oxalate | 70–80% | Radio-opaque | Hypercalciuria, hyperoxaluria, hypocitraturia |
| Calcium phosphate | 10% | Radio-opaque | RTA type I, hyperparathyroidism |
| Struvite (magnesium ammonium phosphate) | 10–15% | Radio-opaque | Urease-producing bacteria (Proteus, Klebsiella); forms staghorn calculi |
| Uric acid | 5–10% | Radiolucent | Hyperuricosuria, acidic urine, gout, myeloproliferative disorders |
| Cystine | 1–2% | Faintly opaque | Cystinuria (autosomal recessive) |
Pathophysiology
Clinical Presentation
- Ureteral colic: severe, colicky flank pain radiating to ipsilateral groin/genitalia; N/V
- Hematuria (micro or gross) in 85%
- Urinary urgency/frequency if stone near UVJ
- No comfortable position (unlike peritonitis)
Diagnosis
- Non-contrast CT KUB: gold standard; detects all stones; identifies hydronephrosis
- Ultrasound: first-line in pregnancy; detects hydronephrosis; poor at ureteral stones
- Plain KUB: radio-opaque stones; adjunct only
- Urine dipstick + microscopy: hematuria; pH (alkaline → struvite or infection; acidic → uric acid)
- 24-hour urine collection after stone event: Ca, oxalate, urate, citrate, Cr, volume, pH
Management
Acute
| Situation | Management |
|---|---|
| Stone <5 mm | Conservative; 95% pass spontaneously; NSAIDs (ketorolac) + α-blocker (tamsulosin = MET) |
| Stone 5–10 mm | MET with α-blocker; monitor |
| Stone >10 mm | Intervention likely needed |
| Infected obstructing stone | Urological emergency: urgent decompression (ureteral stent or percutaneous nephrostomy) + IV antibiotics |
| Stone with solitary kidney | Urgent intervention |
Elective Intervention
| Procedure | Indication |
|---|---|
| ESWL (extracorporeal shock wave lithotripsy) | Renal/proximal ureteral stones <2 cm; non-lower pole preferred |
| Ureteroscopy + laser lithotripsy (URS) | Ureteral stones, lower pole renal stones; any size |
| PCNL (percutaneous nephrolithotomy) | Large renal stones >2 cm, staghorn calculi, lower pole stones >1 cm |
| Open/laparoscopic surgery | Rare; complex anatomy, failed endourology |
Prevention
- General: fluid intake >2.5 L/day; reduce salt, animal protein; normal calcium intake
- Calcium oxalate: thiazides (↓ hypercalciuria), potassium citrate (↑ citrate), reduce oxalate intake
- Uric acid: allopurinol, urinary alkalinization (sodium bicarbonate / potassium citrate) to pH >6
- Struvite: treat underlying infection; acetohydroxamic acid (urease inhibitor)
- Cystine: aggressive hydration, urinary alkalinization, D-penicillamine or tiopronin
8. Hydronephrosis
Definition
Causes
| Level | Causes |
|---|---|
| Kidney / UPJ | Congenital UPJO, stone, tumor, fungus ball |
| Ureter | Stone, stricture, tumor, external compression (retroperitoneal fibrosis, tumor, lymphoma), megaureter |
| Bladder | Tumor, neurogenic bladder, diverticulum |
| Bladder outlet / urethra | BPH, PUV, urethral stricture, meatal stenosis |
| Extrinsic | Pregnancy, retroperitoneal fibrosis, endometriosis |
Grading (Society for Fetal Urology — SFU)
- Grade 0: Normal
- Grade 1: Mild pelvis dilation only
- Grade 2: Pelvis + some calyceal dilation
- Grade 3: Pelvis + all calyces dilated, normal parenchyma
- Grade 4: Grade 3 + thinned parenchyma
Clinical Features
- May be asymptomatic (chronic)
- Flank pain, UTIs, hematuria
- Bilateral severe hydronephrosis → renal failure (anuria, uremic symptoms)
- Hypertension (compression of renal vasculature)
Diagnosis
- Ultrasound: first-line; identifies dilation, parenchymal thinning
- CT urography: identifies cause and level of obstruction
- MAG-3 diuretic renogram: differentiates true obstruction from non-obstructive dilation; assesses split renal function (Furosemide washout T½ > 20 min = obstructed)
- Whitaker test: invasive pressure-flow study; gold standard for equivocal cases
Management
- Relieve obstruction: ureteral stent, percutaneous nephrostomy (urgent if infected)
- Treat underlying cause (stone removal, pyeloplasty for UPJO, BPH treatment)
- Nephrectomy if non-functioning kidney (<10% split function) causing complications
9. Tumors of the GU System
Renal Tumors
Renal Cell Carcinoma (RCC)
- Epidemiology: most common renal malignancy in adults; M:F = 2:1; peak age 60s
- Histology: Clear cell (75%) → VHL gene mutation; Papillary (15%); Chromophobe (5%); Collecting duct (rare, aggressive)
- Classic triad: flank pain + hematuria + palpable mass (only 10% present with all three; indicates advanced disease)
- Paraneoplastic syndromes: polycythemia (ectopic EPO), hypercalcemia (PTHrP), hypertension (renin), Stauffer syndrome (non-metastatic hepatic dysfunction)
- Staging (TNM): T1 ≤7 cm confined to kidney; T2 >7 cm; T3 vascular/adrenal/perinephric; T4 beyond Gerota's fascia
- Diagnosis: CT abdomen with/without contrast; IVC thrombus on MRI
- Treatment:
- Localized: partial nephrectomy (preferred) or radical nephrectomy
- Metastatic: VEGF-targeted therapy (sunitinib, pazopanib); immunotherapy (nivolumab + ipilimumab); mTOR inhibitors
- RCC is resistant to chemotherapy and radiation
Wilms Tumor (Nephroblastoma)
- Most common renal tumor in children (peak age 3–4 years)
- Associated with WAGR syndrome (Wilms, Aniridia, GU abnormalities, intellectual disability — WT1 gene)
- Abdominal mass (often found by parents bathing child); hypertension
- Do NOT palpate — risk of rupture and dissemination
- Rx: nephrectomy + chemotherapy (actinomycin D + vincristine) ± radiation; excellent prognosis (>90% survival)
Urothelial (Transitional Cell) Carcinoma
Bladder Cancer
- Most common urological malignancy in adults
- Risk factors: smoking (single most important), aniline dyes, aromatic amines, cyclophosphamide, Schistosoma haematobium (squamous cell variant)
- Presentation: painless gross hematuria (classic); irritative voiding symptoms
- Types: TCC/urothelial carcinoma (90%), squamous cell (5–10%), adenocarcinoma (1–2%)
- Staging:
- Non-muscle-invasive (NMIBC): Ta (papillary, non-invasive), Tis (CIS), T1 (lamina propria)
- Muscle-invasive (MIBC): T2+ (detrusor involvement)
- Diagnosis: cystoscopy + TURBT (transurethral resection of bladder tumor) — gold standard; urine cytology (good for high-grade/CIS); CTU
- Treatment:
- NMIBC: TURBT; intravesical BCG (high-grade/CIS) or mitomycin C (low-grade)
- MIBC: radical cystectomy (+ neobladder or ileal conduit) + neoadjuvant cisplatin-based chemotherapy
- Metastatic: cisplatin + gemcitabine; checkpoint inhibitors (pembrolizumab, atezolizumab)
Upper Tract Urothelial Carcinoma (UTUC)
- Renal pelvis > ureter
- Associated with Balkan nephropathy, aristolochic acid, Lynch syndrome
- Rx: radical nephroureterectomy with bladder cuff excision
Prostate Diseases
Benign Prostatic Hyperplasia (BPH)
- Proliferation of stromal and epithelial cells in transition zone
- Prevalence: 50% by age 50; 90% by age 85
- Symptoms: LUTS — obstructive (hesitancy, weak stream, straining, incomplete emptying, overflow incontinence) + irritative (frequency, urgency, nocturia)
- Diagnosis: IPSS questionnaire, PSA, DRE, uroflowmetry, post-void residual (PVR) ultrasound
- Treatment:
- Watchful waiting: mild symptoms (IPSS <8)
- Medical: α-1 blockers (tamsulosin, alfuzosin — quick onset, relax smooth muscle) + 5α-reductase inhibitors (finasteride, dutasteride — shrink prostate, prevent AUR)
- Surgical: TURP (gold standard), HOLEP, GreenLight laser vaporization, TUIP (small glands)
- Minimally invasive: prostatic urethral lift (UroLift), water vapor therapy (Rezum)
Prostate Cancer
- Most common malignancy in men; leading cause of cancer death in men (2nd after lung)
- Risk factors: age >50, African-American race, family history (BRCA2)
- Pathology: adenocarcinoma (95%); arises in peripheral zone (palpable on DRE)
- Grading: Gleason score (primary + secondary grade, each 1–5); Grade Group 1 = Gleason 3+3=6 (low risk) to Grade Group 5 = Gleason 9–10 (very high risk)
- Screening: PSA ± DRE; controversial; shared decision-making at age 50 (45 for high-risk)
- Diagnosis: transrectal ultrasound (TRUS)-guided biopsy; multiparametric MRI (mpMRI) fusion biopsy
- Staging: bone scan (metastases), CT abdomen/pelvis
- Risk stratification (D'Amico):
Risk PSA Gleason Stage Low <10 ≤6 ≤T2a Intermediate 10–20 7 T2b High >20 ≥8 T2c–T3 - Treatment:
- Low risk: active surveillance
- Localized: radical prostatectomy (retropubic or robotic) OR external beam radiotherapy (EBRT) OR brachytherapy
- High-risk/locally advanced: EBRT + androgen deprivation therapy (ADT; LHRH agonists: leuprolide; antagonists: degarelix)
- Metastatic: ADT + docetaxel or enzalutamide/abiraterone
- Castration-resistant (CRPC): abiraterone, enzalutamide, radium-223, PARP inhibitors (if BRCA mutant), sipuleucel-T
Testicular Tumors
- Most common solid malignancy in men 15–35 years
- 95% are germ cell tumors (GCTs):
Type Features Markers Seminoma (50%) Homogeneous; radiosensitive; AFP normal; β-hCG may be ↑ AFP (-), β-hCG (±), LDH (±) Non-seminomatous GCT (NSGCT) Embryonal, yolk sac, choriocarcinoma, teratoma AFP (↑), β-hCG (↑), LDH (↑) - Presentation: painless testicular mass ± heaviness; hydrocele; gynecomastia (β-hCG)
- Diagnosis: scrotal ultrasound; do NOT biopsy transscrotal (risk of lymphatic spread); CT chest/abdomen/pelvis for staging
- Treatment: radical inguinal orchiectomy (first step always); then:
- Seminoma stage I: surveillance or carboplatin × 1 cycle
- Seminoma metastatic: BEP chemotherapy (bleomycin, etoposide, cisplatin) ± RPLND
- NSGCT: BEP ± RPLND
- Prognosis: excellent; >95% cure rate even with metastatic disease
Urethral Tumors
- Rare; most common in females
- SCC most common histology
- Presentation: hematuria, obstructive symptoms, urethral mass
- Distal tumors: surgery (urethrectomy) ± radiation
- Proximal/invasive: combined modality
10. Emergency Urology
| Emergency | Presentation | Key Action |
|---|---|---|
| Testicular torsion | Sudden severe scrotal pain, nausea/vomiting; absent cremasteric reflex; "bell-clapper" deformity; US shows absent blood flow | Surgical emergency: bilateral orchidopexy within 6 hours (salvage rate ~100%); >24h → orchiectomy |
| Acute urinary retention (AUR) | Inability to void, painful distended bladder, suprapubic dullness | Immediate urethral catheterization (or SPC if catheter fails); treat cause (BPH, constipation, anticholinergics) |
| Urosepsis | SIRS criteria + urological source (obstructed UTI); hypotension, tachycardia, fever | IV antibiotics + urgent drainage (ureteral stent or PCN) + resuscitation — mortality >30% if not drained |
| Renal/ureteral colic with infection | Fever + obstructing stone | Urgent decompression (PCN or stent) + broad-spectrum antibiotics |
| Penile fracture | Cracking sound, immediate detumescence, "eggplant deformity" | Immediate surgical repair |
| Paraphimosis | Retracted foreskin cannot be reduced; glans edema → ischemia | Manual reduction with ice; dorsal slit or circumcision if fails; true emergency |
| Priapism | Erection >4 hours; ischemic (low-flow, painful) vs. non-ischemic (high-flow, painless after perineal trauma) | Ischemic: aspirate + intracavernous phenylephrine; if fails → shunt surgery; non-ischemic: observation or embolization |
| Fournier's gangrene | Scrotal/perineal necrosis, crepitus, rapid spreading infection | ICU + aggressive debridement + IV antibiotics + hyperbaric O₂ |
| Obstructive uropathy / bilateral hydronephrosis | Anuria, rising creatinine, flank pain; bilateral obstruction → renal failure | Bilateral stenting or PCN; identify cause (pelvic malignancy, stones, fibrosis) |
| Gross hematuria with clot retention | Cannot void due to clots in bladder | Three-way catheter + continuous bladder irrigation (CBI); cystoscopy if persistent |
Summary Table: Key Diagnostic Modalities
| Condition | Best First Test | Gold Standard |
|---|---|---|
| Urolithiasis | Ultrasound (or NCCT) | Non-contrast CT KUB |
| Bladder tumor | Ultrasound | Cystoscopy + TURBT |
| Renal mass | CT abdomen w/contrast | CT ± biopsy |
| Prostate cancer | PSA + DRE | TRUS biopsy / mpMRI fusion |
| Testicular tumor | Scrotal ultrasound | Radical inguinal orchiectomy |
| Hydronephrosis | Ultrasound | MAG-3 renogram (functional) |
| Urethral injury | RUG (retrograde urethrogram) | RUG |
| Bladder rupture | CT cystography | CT cystography |
| Vesicoureteral reflux | VCUG | VCUG |