spindle cell tumors
Reading File
search_medical_text
spindle cell tumors classification histopathology diagnosis
search_medical_text
spindle cell neoplasms differential diagnosis immunohistochemistry
search_medical_image
spindle cell tumor histology microscopy
GradeResponse
GradeResponse
GradeResponse
Spindle Cell Tumors
Spindle cell tumors are a broad category of neoplasms characterized by elongated, fusiform (spindle-shaped) cells on histology. They span benign to malignant entities and arise from diverse cell lineages — mesenchymal, epithelial, melanocytic, and neural.
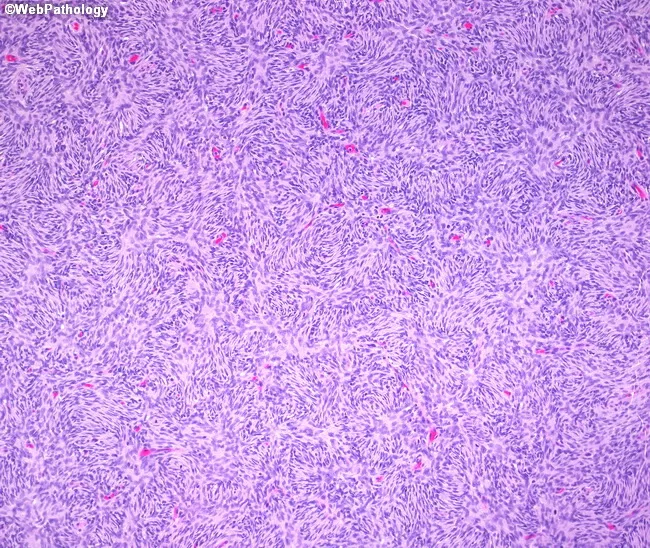
Histologic Appearance
The hallmark is elongated cells with oval-to-tapering nuclei arranged in fascicles, whorls, or storiform (cartwheel) patterns. Assessing mitotic activity, nuclear pleomorphism, necrosis, and architectural pattern is critical to grading.
Classification by Cell of Origin
| Category | Key Tumors | Malignant Counterpart |
|---|---|---|
| Fibroblastic/Myofibroblastic | Nodular fasciitis, desmoid fibromatosis, DFSP | Fibrosarcoma, myofibrosarcoma |
| Smooth muscle | Leiomyoma | Leiomyosarcoma |
| Peripheral nerve sheath | Neurofibroma, schwannoma | MPNST |
| GI stromal (GIST) | Benign GIST | Malignant GIST |
| Vascular | Spindle cell hemangioma | Angiosarcoma, Kaposi sarcoma |
| Melanocytic | — | Spindle cell melanoma, desmoplastic melanoma |
| Epithelial | — | Spindle cell carcinoma, sarcomatoid carcinoma |
| Thyroid | — | Anaplastic thyroid carcinoma (spindle cell variant) |
| Mixed/Other | Synovial sarcoma | Biphasic/monophasic synovial sarcoma |
Key Entities in Detail
1. GIST (Gastrointestinal Stromal Tumor)
The most common mesenchymal tumor of the GI tract. Per Harrison's (p. 2463):
- Histology: Spindle cell subtype ~70%; epithelioid ~20%; mixed ~10%
- IHC: c-kit (CD117) and CD34 positivity; mutational analysis of cKIT and PDGFRA required in all cases
- Treatment:
- Localized: laparoscopic wedge/segmental resection (lymphadenectomy not needed)
- High-risk/metastatic: imatinib (c-kit tyrosine kinase inhibitor) for cKIT-mutated tumors
- Prognosis determinants: tumor size + mitotic index (not histology or mutation type alone)
2. Dermatofibrosarcoma Protuberans (DFSP)
- Low-grade fibroblastic sarcoma of the dermis/subcutis
- Storiform pattern; CD34+, factor XIIIa−
- Characteristic COL1A1-PDGFB translocation t(17;22)
- Low metastatic potential but high local recurrence; imatinib used for unresectable disease
3. Leiomyosarcoma
- Smooth muscle origin; intersecting fascicles of cells with "cigar-shaped" nuclei
- IHC: SMA+, desmin+, h-caldesmon+
- Common sites: uterus, retroperitoneum, vascular wall
- Graded by FNCLCC system; prognosis depends on grade and site
4. Malignant Peripheral Nerve Sheath Tumor (MPNST)
- Often arises in NF1 patients (50%) or sporadically
- IHC: S100+ (only ~50%), SOX10+, loss of H3K27me3 (trimethylation) — sensitive/specific marker
- High-grade; wide excision ± radiation; poor response to chemotherapy
5. Synovial Sarcoma
- Despite name, not of synovial origin; arises near joints in young adults
- Monophasic (pure spindle) or biphasic (spindle + epithelial glands)
- Cytogenetics: t(X;18)(p11;q11) → SS18-SSX fusion (diagnostic)
- IHC: TLE1+, EMA+, CK+; CD34−, S100−
- Chemosensitive (ifosfamide-based regimens)
6. Spindle Cell / Desmoplastic Melanoma
- Rare, arises on sun-damaged skin (head/neck)
- Mimics sarcoma or nerve sheath tumor
- IHC: S100+++ (strong), SOX10+; HMB-45 and Melan-A often negative (pitfall)
- Surgery is primary treatment; immunotherapy effective for metastatic disease
7. Anaplastic Thyroid Carcinoma (Spindle Cell Variant)
- Rapidly progressive, lethal; typically in elderly patients with large neck masses
- Diagnosis confirmed histologically (exclude lymphoma, MALT, medullary carcinoma — all more treatable) per Anaplastic Thyroid Cancer Update (p. 9)
- IHC: variable; often p53+, loss of TTF-1; cytokeratin focally positive
- Multi-modal approach (surgery + EBRT + systemic therapy); median survival ~5 months
Immunohistochemistry Panel for Differential Diagnosis
| Marker | Fibroblastic | Smooth Muscle | GIST | Neural | Melanoma | Synovial Sarcoma | Carcinoma |
|---|---|---|---|---|---|---|---|
| CD117 (c-kit) | − | − | + | − | − | − | − |
| CD34 | +/− | − | + | − | − | − | − |
| SMA | +/− | + | − | − | − | − | − |
| S100 | − | − | − | + | + | − | − |
| TLE1 | − | − | − | − | − | + | − |
| CK/EMA | − | − | − | − | − | +/− | + |
| HMB-45 | − | − | − | − | +/− | − | − |
Diagnostic Approach
- Core needle biopsy (preferred over FNA for soft tissue masses)
- H&E morphology → architecture, mitoses, necrosis, pleomorphism
- IHC panel tailored to morphologic differential
- Molecular/cytogenetic testing when IHC is ambiguous:
- FISH or RT-PCR for SS18-SSX (synovial sarcoma)
- PDGFB rearrangement (DFSP)
- cKIT/PDGFRA sequencing (GIST)
- H3K27me3 loss by IHC (MPNST)
- Staging imaging: MRI for local extent, CT chest/abdomen/pelvis for metastases
General Management Principles
- Surgery: mainstay for localized disease; wide negative margins critical
- Radiation: adjuvant for high-grade or close/positive margins (especially extremity sarcomas)
- Chemotherapy: most sarcomas have limited chemo-sensitivity; exceptions include synovial sarcoma, rhabdomyosarcoma, Ewing sarcoma
- Targeted therapy: imatinib/sunitinib (GIST), imatinib (DFSP with PDGFB fusion), dabrafenib+trametinib (BRAF-mutated anaplastic thyroid ca)
- Immunotherapy: effective in desmoplastic melanoma
The key to spindle cell tumor diagnosis is integrating morphology, IHC, and molecular findings — no single stain is sufficient, and clinical context (age, site, size, growth rate) remains indispensable.
This is a shared conversation. Sign in to Orris to start your own chat.