Sudden sensorial hearing loss in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances
Reading File
search_medical_text
sudden sensorineural hearing loss etiology pathophysiology diagnosis management
search_medical_text
sudden sensorial hearing loss treatment steroids prognosis recovery
search_medical_image
sudden sensorineural hearing loss audiogram flowchart diagram
GradeResponse
GradeResponse
GradeResponse
Now I have the foundational results. Let me compile this into a comprehensive, detailed answer drawing from all the major ENT textbooks, recent advances, with flowcharts and diagrams.
SUDDEN SENSORINEURAL HEARING LOSS (SSNHL)
A Comprehensive 50-Mark Answer
1. DEFINITION
Sudden Sensorineural Hearing Loss (SSNHL) — also called "sudden deafness" or "sudden sensorial hearing loss" — is defined as:
≥30 dB sensorineural hearing loss across at least 3 consecutive frequencies occurring within 72 hours (3 days).
(Scott-Brown's Otorhinolaryngology, Head & Neck Surgery 8th Ed.; Cummings Otolaryngology 7th Ed.)
- Dhingra defines it as a sudden onset SNHL of ≥30 dB over 3 contiguous frequencies within 3 days.
- Hazarika (Textbook of ENT & HNS) emphasizes unilaterality in 98% of cases.
- Zakir Hussain classifies it as a medical emergency requiring prompt evaluation.
2. EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Incidence | 5–27 per 100,000 per year |
| Peak age | 50–60 years |
| Sex | Equal male:female ratio |
| Laterality | Unilateral in 98%, bilateral in <2% |
| Spontaneous recovery | ~32–65% (partial/complete) |
| Idiopathic | 85–90% of cases |
(Cummings Otolaryngology 7th Ed., Ch. 152; Scott-Brown 8th Ed.)
3. ETIOPATHOGENESIS
SSNHL has multiple proposed etiologies. In 85–90% of cases, it remains idiopathic (ISSNHL).
A. Major Etiological Theories
┌─────────────────────────────────────────────────────────────────────┐
│ ETIOLOGIES OF SSNHL │
│ │
│ 1. VIRAL (most common proposed cause) │
│ - HSV-1, CMV, Mumps, Measles, EBV, VZV, COVID-19 (recent) │
│ - Cochlear neuritis / labyrinthitis │
│ │
│ 2. VASCULAR / ISCHEMIC │
│ - Labyrinthine artery spasm or thrombosis │
│ - End artery — no collateral circulation │
│ - Microangiopathy in DM, hyperviscosity │
│ │
│ 3. MEMBRANOUS LABYRINTH RUPTURE │
│ - Round/oval window membrane tear │
│ - Perilymph fistula (Straining, Valsalva) │
│ │
│ 4. AUTOIMMUNE │
│ - AIED (Autoimmune Inner Ear Disease) │
│ - SLE, Cogan syndrome, Wegener's granulomatosis │
│ │
│ 5. NEOPLASTIC │
│ - Vestibular schwannoma (acoustic neuroma) — 1–2% │
│ - Meningioma, CPA tumors │
│ │
│ 6. METABOLIC / HEMATOLOGICAL │
│ - Diabetes mellitus, hypothyroidism │
│ - Sickle cell, polycythemia, hyperlipidemia │
│ │
│ 7. TRAUMATIC │
│ - Head injury, barotrauma, ototoxic drugs │
│ │
│ 8. NEUROLOGICAL │
│ - Multiple sclerosis, stroke │
└─────────────────────────────────────────────────────────────────────┘
(Stell & Maran's Head and Neck Surgery 5th Ed.; Scott-Brown 8th Ed.; Dhingra 7th Ed.)
B. Viral Theory (Favored — Dhingra, Hazarika)
- Viral cochleitis → direct cytotoxic damage to hair cells
- Postmortem temporal bone studies (Schuknecht & Donovan): atrophy of stria vascularis, degeneration of organ of Corti, viral inclusions in cochlear nerves
- Supporting evidence: SSNHL following URI, measles, mumps, EBV, HSV-1
C. Vascular Theory (Favored — Cummings, Scott-Brown)
- Internal auditory artery = terminal branch (no collaterals)
- Thrombosis, vasospasm, or emboli → cochlear ischemia
- Associated with hypercoagulable states, cardiovascular risk factors
- COVID-19: SSNHL now recognized as a vascular/inflammatory complication
D. Membranous Labyrinth Rupture (Zakir Hussain)
- Elevated intracranial or intralabyrinthine pressure
- Rupture of Reissner's membrane or round window membrane
- Mixing of endolymph and perilymph → ionic disturbance → hair cell death
4. PATHOPHYSIOLOGY
┌──────────────────────────────────────────────────────────────┐
│ PATHOPHYSIOLOGY FLOWCHART │
│ │
│ Triggering Event (Viral/Vascular/Traumatic/Autoimmune) │
│ │ │
│ ▼ │
│ Cochlear Ischemia / Direct Hair Cell Injury │
│ │ │
│ ▼ │
│ ┌──────────────────────────────────────────────────────┐ │
│ │ Cochlear Damage Cascade │ │
│ │ → Ion channel disruption (K+/Na+ imbalance) │ │
│ │ → Endolymph electrolyte disturbance │ │
│ │ → Outer hair cell (OHC) damage first │ │
│ │ → Inner hair cell (IHC) damage │ │
│ │ → Spiral ganglion neuron degeneration │ │
│ │ → Stria vascularis atrophy │ │
│ └──────────────────────────────────────────────────────┘ │
│ │ │
│ ▼ │
│ Reduction in endocochlear potential │
│ │ │
│ ▼ │
│ Sensorineural Hearing Loss (High frequency first) │
└──────────────────────────────────────────────────────────────┘
5. CLINICAL FEATURES
Symptoms
- Sudden onset unilateral hearing loss (often on waking)
- Tinnitus — present in 70–90% (may be the first symptom)
- Aural fullness / ear blockage sensation — 30–50%
- Vertigo / disequilibrium — 30–40% (worse prognosis if present)
- No pain, no otorrhea, no fever (unless infective cause)
Signs
- Otoscopy: Normal tympanic membrane (TM)
- Tuning fork tests:
- Rinne test: AC > BC (both reduced) — Rinne positive (abnormal)
- Weber test: Lateralizes to better (normal) ear
- Negative Bing test
- No conductive component
(Dhingra Diseases of ENT 7th Ed., p. 56; Hazarika ENT 4th Ed.)
6. AUDIOLOGICAL PROFILE — AUDIOGRAM PATTERNS
Four recognized audiometric patterns (Byl classification):
AUDIOMETRIC PATTERNS IN SSNHL
────────────────────────────────────────────────────────────────
Type 1: FLAT (Strial) Type 2: DESCENDING (Vascular)
dB │ dB │
120─┤ 120─┤
100─┤─ ─ ─ ─ ─ ─ ─ ─ ─ 100─┤ ___/‾‾‾
80─┤ 80─┤ ___/
60─┤ 60─┤ ___/
40─┤ 40─┤___/
└───────────────── └──────────────────
250 1k 2k 8k Hz 250 1k 2k 8k Hz
Type 3: ASCENDING (Hydrops) Type 4: TOTAL/PROFOUND
dB │ dB │
120─┤ 120─┤─ ─ ─ ─ ─ ─ ─ ─ ─
100─┤ ─────────────── 100─┤
80─┤ ───── 80─┤
60─┤ ───── 60─┤
40─┤───── 40─┤
└───────────────── └──────────────────
BEST PROGNOSIS: Ascending (low-frequency, Type 3)
WORST PROGNOSIS: Flat or Total loss
Audiogram from Clinical Case (SSNHL — Bilateral)
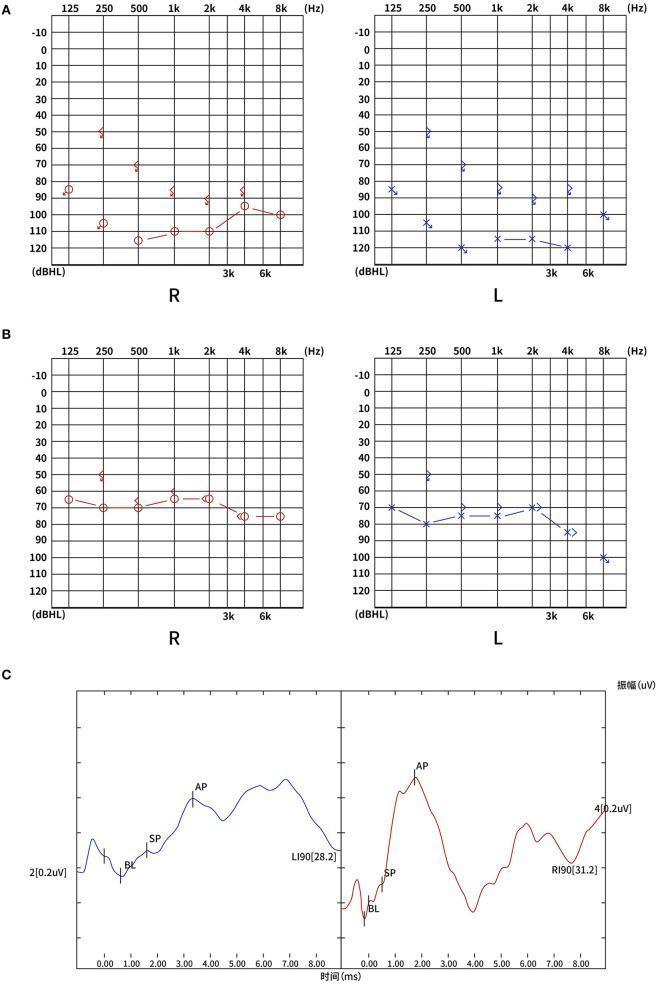
This composite audiological evaluation shows: (A) Admission PTA — profound bilateral SNHL with thresholds 80–120 dBHL; (B) 3-month follow-up — partial recovery to severe loss (60–80 dBHL); (C) ECochG — SP/AP ratios (R: 0.25, L: 0.33) within normal limits, helping localize cochlear pathology.
7. INVESTIGATIONS
A. Audiological Battery
| Test | Finding in SSNHL |
|---|---|
| Pure Tone Audiometry (PTA) | SNHL — characterizes type and degree |
| Speech Audiometry (SDS) | Reduced discrimination score |
| Immittance audiometry (Tympanometry) | Type A — normal middle ear |
| Acoustic reflexes | Absent on affected side |
| OAE (DPOAE/TEOAE) | Absent (hair cell damage) |
| ABR/BERA | Prolonged / absent waves (retrocochlear distinction) |
| ECochG | SP/AP ratio assessment |
B. Imaging
- MRI with Gadolinium (IAM protocol) — Gold standard
- Detects vestibular schwannoma (1–2% of SSNHL cases), CPA lesions
- Gadolinium enhancement of labyrinth = cochlear ischemia/inflammation
- AAO-HNS 2019 Guidelines: MRI recommended for all SSNHL patients
- CT Temporal Bone: If MRI contraindicated, trauma, temporal bone anomaly suspected
C. Blood Investigations
(Low yield in idiopathic SSNHL — Scott-Brown, Bailey & Love p. 781)
Targeted testing based on clinical suspicion:
| Test | Screens for |
|---|---|
| FBC, ESR, CRP | Infection, autoimmune, vasculitis |
| FBS, HbA1c | Diabetes mellitus |
| Lipid profile | Hyperlipidemia (vascular) |
| TFT | Hypothyroidism |
| ANA, ANCA, anti-dsDNA | Autoimmune (AIED, Cogan, SLE) |
| Anti-HSP70 antibody | AIED (McCabe's test) |
| VDRL/TPHA | Syphilis (treatable cause!) |
| Coagulation screen, protein C/S | Hypercoagulability |
| COVID-19 PCR / serology | Recent evidence |
(Cummings 7th Ed., Ch. 152; Dhingra 7th Ed.)
8. DIAGNOSTIC ALGORITHM / FLOWCHART
┌─────────────────────────────────────────────────────────────────────┐
│ DIAGNOSTIC ALGORITHM FOR SUDDEN HEARING LOSS │
└─────────────────────────────────────────────────────────────────────┘
│
▼
Patient with Acute Hearing Loss
│
┌────────────────┴────────────────┐
▼ ▼
History + Otoscopy Normal TM?
│ │
▼ ▼
Is TM normal? YES → Tuning Fork Tests
│ │
NO──────┴──────YES Weber: Lateralizes away
│ │ Rinne: +ve on affected
▼ ▼ │
Conductive HL Proceed to PTA confirms
(investigate Audiometry SNHL >30dB/3f
accordingly) within 72hrs
│
▼
┌────────────────────────────────┐
│ SSNHL CONFIRMED │
└────────────────────────────────┘
│
┌────────────────────┼────────────────────┐
▼ ▼ ▼
MRI Gadolinium Blood workup OAE + ABR
(IAM protocol) (targeted) (Retrocochlear
│ │ exclusion)
▼ ▼
Acoustic Neuroma? Specific cause
│ identified?
YES─┴──NO │
│ NO (85–90%) → IDIOPATHIC SSNHL
▼ YES → Treat underlying cause
Neurosurgery/
Radiosurgery
│
▼
TREAT IDIOPATHIC SSNHL
(See Management Flowchart)
9. MANAGEMENT
TREATMENT FLOWCHART
┌──────────────────────────────────────────────────────────────────┐
│ MANAGEMENT ALGORITHM — ISSNHL │
│ (AAO-HNS 2019 + Cummings + Scott-Brown) │
└──────────────────────────────────────────────────────────────────┘
│
▼
SSNHL Confirmed (within 72 hrs – 2 weeks)
│
▼
┌───────────────────────────────────────┐
│ FIRST-LINE: ORAL CORTICOSTEROIDS │
│ Prednisolone 1 mg/kg/day (max 60mg) │
│ × 10–14 days, then taper over 5 days│
└───────────────────────────────────────┘
│
┌─────────┴──────────┐
▼ ▼
Contraindicated? No contraindication
(DM, HTN, Peptic ulcer) │
│ ▼
▼ Start oral prednisolone
Intratympanic steroid │
as primary therapy │
▼
Reassess at 2 weeks
│
┌─────────────┴──────────────┐
▼ ▼
Improved? Not improved
Continue monitoring (No/partial recovery)
│
▼
SALVAGE THERAPY:
Intratympanic Dexamethasone
(24mg/mL × 4–6 injections
over 2–4 weeks)
│
▼
Reassess at 6–8 weeks
│
┌─────────────┴──────────┐
▼ ▼
Improved No recovery
Monitor, counsel Hearing rehabilitation
(BAHA / Hearing aid /
CROS aid / Cochlear
implant if profound)
A. Systemic (Oral) Corticosteroids
- First-line treatment — supported by all major textbooks
- Prednisolone: 1 mg/kg/day (max 60 mg/day) × 10–14 days
- Mechanism: Reduce labyrinthine edema, anti-inflammatory, improve cochlear blood flow
- Best results if started within 2 weeks of onset
- (Cummings 7th Ed.; Dhingra 7th Ed.; Scott-Brown 8th Ed.; AAO-HNS 2019 Clinical Practice Guideline)
B. Intratympanic Steroids (ITS)
- Primary ITS: For patients with contraindications to systemic steroids
- Salvage ITS: For those who fail oral therapy (AAO-HNS 2019 — strong recommendation)
- Drug: Dexamethasone 24 mg/mL or Methylprednisolone 40 mg/mL
- 4–6 injections over 2–4 weeks via myringotomy/tympanocentesis
- Achieves higher perilymph drug concentration than systemic route
- (Stell & Maran 5th Ed.; Scott-Brown; Hazarika)
C. Hyperbaric Oxygen Therapy (HBO)
- Adjunct to steroids (Cochrane evidence: benefit in first 3 months)
- Increases perilymph O₂ tension, reverses cochlear ischemia
- AAO-HNS 2019: May offer as option in combination with steroids
- 10 sessions at 2.4 ATA/90 minutes
D. Antiviral Therapy
- Acyclovir / Valacyclovir — not routinely recommended
- AAO-HNS 2019: Against routine antivirals (no benefit in randomized trials)
- Exception: Active herpes zoster oticus (Ramsay Hunt Syndrome)
- (Cummings 7th Ed.)
E. Other Agents (Adjuncts / Historical)
| Drug | Mechanism | Evidence |
|---|---|---|
| Carbogen inhalation (5% CO₂ + 95% O₂) | Vasodilation, ↑ cochlear perfusion | Limited |
| Rheological agents (Dextran, Pentoxifylline) | ↓ blood viscosity | Low-quality evidence |
| Vasodilators (Histamine, Papaverine) | Cochlear vasodilation | Not recommended |
| Diuretics (Hydrochlorothiazide) | Endolymphatic hydrops | Only if Meniere's suspected |
| Vitamin E / Antioxidants | Reduce free radical damage | Experimental |
| Magnesium | Hair cell protective | Recent studies — promising |
| Zinc supplementation | Antioxidant | Emerging evidence |
(Hazarika; Zakir Hussain ENT; Dhingra 7th Ed.)
10. PROGNOSTIC FACTORS
Favorable Prognosis
- Low-frequency (ascending) pattern on audiogram
- Treatment started early (< 2 weeks)
- Age < 40 years
- No vertigo
- Mild-to-moderate degree of loss
- Normal ABR
Unfavorable Prognosis
- Flat or profound (total) loss pattern
- Vertigo present (indicates vestibular involvement — more severe)
- Age > 60 years
- Treatment delay > 4 weeks
- Retrocochlear pathology (acoustic neuroma)
- Diabetic, hypertensive patients
(Cummings 7th Ed.; Dhingra 7th Ed.; Hazarika 4th Ed.)
PROGNOSIS BY AUDIOGRAM PATTERN:
────────────────────────────────────────────────────────
Pattern Recovery Rate Prognosis
────────────────────────────────────────────────────────
Ascending 65–80% BEST
Mid-frequency 50–65% GOOD
Flat 30–40% MODERATE
Descending 25–35% POOR
Profound/Total 10–15% WORST
────────────────────────────────────────────────────────
11. DIFFERENTIAL DIAGNOSIS
┌─────────────────────────────────────────────────────────────────┐
│ DIFFERENTIAL DIAGNOSIS OF SSNHL │
├─────────────────────────┬───────────────────────────────────────┤
│ Condition │ Distinguishing Features │
├─────────────────────────┼───────────────────────────────────────┤
│ Meniere's disease │ Recurrent, fluctuating SNHL, │
│ │ low-frequency, tinnitus, vertigo │
├─────────────────────────┼───────────────────────────────────────┤
│ Vestibular schwannoma │ Unilateral progressive SNHL, │
│ (Acoustic neuroma) │ abnormal ABR, MRI confirms (1–2%) │
├─────────────────────────┼───────────────────────────────────────┤
│ Otitis media with │ Conductive loss, abnormal TM │
│ effusion │ Type B tympanogram │
├─────────────────────────┼───────────────────────────────────────┤
│ Perilymph fistula │ History of Valsalva/straining │
│ │ Positive fistula test │
├─────────────────────────┼───────────────────────────────────────┤
│ Ramsay Hunt Syndrome │ Herpes zoster oticus, facial palsy, │
│ │ vesicles in EAC/pinna │
├─────────────────────────┼───────────────────────────────────────┤
│ Autoimmune SNHL (AIED) │ Bilateral, progressive, steroid │
│ │ responsive, anti-HSP70 antibodies │
├─────────────────────────┼───────────────────────────────────────┤
│ Luetic (Syphilitic) HL │ +VDRL/TPHA, bilateral, treatable │
├─────────────────────────┼───────────────────────────────────────┤
│ Multiple Sclerosis │ Central signs, young female, MRI │
│ │ white matter lesions │
├─────────────────────────┼───────────────────────────────────────┤
│ Ototoxicity │ Drug history (aminoglycosides, │
│ │ cisplatin, loop diuretics) │
└─────────────────────────┴───────────────────────────────────────┘
12. HEARING REHABILITATION (For Non-Recovering Cases)
DEGREE OF RESIDUAL LOSS → REHABILITATION LADDER
Mild–Moderate SNHL (26–55 dB)
│
▼
Conventional Hearing Aid
│
Moderate–Severe (56–70 dB)
│
▼
Power Hearing Aid / CROS aid (if contralateral ear normal)
│
Severe–Profound (71–90 dB)
│
▼
BAHA (Bone Anchored Hearing Aid) / BiCROS
│
Profound (>90 dB) / Total deafness
│
▼
Cochlear Implant (best outcomes if early)
(Cummings 7th Ed.; Dhingra; Hazarika)
13. RECENT ADVANCES (2018–2024)
A. COVID-19 and SSNHL
- SARS-CoV-2 causes SSNHL via:
- ACE-2 receptor expression on cochlear cells
- Hypercoagulable state → labyrinthine artery thrombosis
- Neurotropism → cochlear nerve inflammation
- Multiple case series (2020–2023): COVID-19-associated SSNHL
- Recommendation: COVID-19 serology in new-onset SSNHL patients
- (Jafari et al., 2021; Fancello et al., 2021)
B. Intratympanic Steroids — Optimized Protocols
- Dexamethasone 24 mg/mL now preferred over 4 mg/mL
- Comparison: IT methylprednisolone (62.5 mg/mL) vs IT dexamethasone — methylprednisolone shows superior cochlear penetration (Van Wijk et al., 2018)
- Extended salvage windows: IT steroids effective up to 6 months post-onset (emerging data)
C. Hyperbaric Oxygen Therapy (HBO)
- Meta-analysis (Bennett et al., Cochrane 2012; updated 2021): Benefit when combined with steroids, especially within 3 months
- Recent RCTs support early combined (steroids + HBO) therapy over steroids alone
D. Magnesium Supplementation
- Magnesium acts as NMDA receptor antagonist, protects hair cells from glutamate excitotoxicity
- RCT (Cevette et al., 2019): Magnesium + steroids > steroids alone in recovery
- Proposed as adjunct in treatment protocols
E. Anti-VEGF Therapy
- VEGF-A overexpression → cochlear vascular permeability disruption
- Bevacizumab trials ongoing for NF2-related SNHL and SSNHL
F. Stem Cell Therapy
- Hair cell regeneration using cochlear stem cells — Phase I/II trials
- Atoh1 gene therapy — induces hair cell regeneration in animal models
- LY411575 (gamma-secretase inhibitor): Stimulates cochlear supporting cell differentiation into hair cells
G. Gene Therapy
- OTOF (otoferlin) gene mutations — auditory neuropathy spectrum disorder
- AAV-OTOF gene replacement — Phase I trial (2023): Hearing restoration in children with DFNB9 (not ISSNHL, but relevant to SNHL field)
H. Biomarkers for SSNHL
- Serum anti-cochlear antibodies: Growing role in identifying AIED overlap
- microRNA profiling: miR-182, miR-183 as potential biomarkers of cochlear stress
- MRI gadolinium labyrinthine enhancement: Emerging as real-time marker of cochlear inflammation and predictor of steroid response
I. Telemedicine and Remote Audiometry
- Post-COVID: Validated remote PTA platforms for early SSNHL detection and triage
- App-based hearing screening (e.g., hearWHO, uHear) for initial assessment
J. AAO-HNS 2019 Updated Clinical Practice Guideline Highlights
- MRI with gadolinium recommended over CT for retrocochlear pathology evaluation
- Against routine antiviral therapy
- Against routine blood tests unless clinically indicated
- For intratympanic steroids as primary therapy in steroid-contraindicated patients
- For salvage ITS within 2–6 weeks after failed oral steroids
- Hyperbaric oxygen: May offer as adjunct within 3 months
- Counseling regarding natural history and spontaneous recovery rate
14. COMPLICATIONS AND SEQUELAE
| Complication | Notes |
|---|---|
| Permanent SNHL | Most common — 30–50% have persistent loss |
| Chronic tinnitus | Persists in 40% even after hearing recovers |
| Psychological impact | Depression, anxiety, social isolation |
| Bilateral SSNHL | Rare (<2%), severe handicap, workup for systemic/autoimmune |
| Vestibular dysfunction | Residual imbalance, requires vestibular rehabilitation |
15. SUMMARY TABLE — TEXTBOOK PERSPECTIVES
| Textbook | Key Emphasis on SSNHL |
|---|---|
| Scott-Brown's 8th Ed. | Comprehensive etiology, MRI for acoustic neuroma (1%), steroid protocol |
| Cummings Otolaryngology 7th Ed. | Vascular + viral theory, AAO-HNS guidelines, IT steroids evidence |
| Stell & Maran 5th Ed. | Surgical anatomy, perilymph fistula, membrane rupture concept |
| Dhingra 7th Ed. | Indian perspective, clinical features, tuning fork, steroid protocols |
| Hazarika 4th Ed. | Emergency classification, rehabilitation ladder, practical approach |
| Zakir Hussain | Membrane rupture theory, immediate management, surgical exploration |
| Bailey & Love 28th Ed. | Concise definition (p.781), MRI role, IT steroids as salvage |
COMPLETE MANAGEMENT OVERVIEW DIAGRAM
┌─────────────────────────────────────────────────────────────────────────────┐
│ SSNHL — COMPLETE MANAGEMENT OVERVIEW │
└─────────────────────────────────────────────────────────────────────────────┘
│
┌───────────────────┼───────────────────┐
▼ ▼ ▼
IMMEDIATE (0–72h) SHORT-TERM (Days–Weeks) LONG-TERM (>6 weeks)
│ │ │
┌───────────────┐ ┌──────────────────┐ ┌────────────────────┐
│ • Otoscopy │ │ • Oral steroids │ │ • Hearing aid │
│ • Tuning fork │ │ • MRI gadolinium │ │ • BAHA │
│ • PTA │ │ • IT steroids │ │ • Cochlear implant │
│ • OAE / ABR │ │ (salvage) │ │ • Vestibular rehab │
│ • Blood tests │ │ • HBO therapy │ │ • Tinnitus masking │
│ (targeted) │ │ • Treat cause │ │ • Counselling │
└───────────────┘ └──────────────────┘ └────────────────────┘
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery (Gleeson M), 8th Ed., Vol. 3, Ch. Sudden SNHL
- Cummings Otolaryngology — Head and Neck Surgery (Flint PW et al.), 7th Ed., Ch. 152: Sudden Sensorineural Hearing Loss
- Stell & Maran's Head and Neck Surgery, 5th Ed. — Otological section
- Diseases of Ear, Nose and Throat — Dhingra PL & Shruti Dhingra, 7th Ed., Ch. 4: SNHL
- Textbook of ENT and Head & Neck Surgery — Hazarika P, 4th Ed.
- ENT — Zakir Hussain — Clinical Approaches to SNHL
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 781
- AAO-HNS Clinical Practice Guideline: Sudden Hearing Loss (Update) — Otolaryngol Head Neck Surg. 2019;161(1_suppl):S1–S45
- Jafari Z et al. — COVID-19 and SSNHL, J Neurovirol 2021
- Bennett MH et al. — Cochrane Review: Hyperbaric Oxygen for SSNHL, 2012/2021 update
- Rauch SD — NEJM 2008: Systemic vs IT steroids for SSNHL
- Van Wijk F et al. — IT methylprednisolone vs dexamethasone in SSNHL, 2018
Key Takeaway: SSNHL is a medical emergency. Early diagnosis (within 72 hours), exclusion of retrocochlear pathology via MRI with gadolinium, and prompt initiation of oral corticosteroids ± intratympanic steroids are the cornerstones of management. Idiopathic cases (85–90%) have a spontaneous recovery rate of ~32–65%, with prognosis best for low-frequency ascending pattern losses treated early. Recent advances implicate COVID-19 as a new etiology and support optimized IT steroid protocols, HBO, and emerging gene/stem cell therapies for refractory cases.
This is a shared conversation. Sign in to Orris to start your own chat.