Meningitis
Reading File
search_medical_text
meningitis etiology pathophysiology clinical features diagnosis
search_medical_text
meningitis treatment management antibiotics empirical therapy complications
search_medical_image
meningitis CSF findings bacterial viral imaging
GradeResponse
GradeResponse
GradeResponse
Meningitis
Overview
Meningitis is inflammation of the meninges (pia mater, arachnoid, and dura) and subarachnoid space, most commonly caused by infection. It is a neurological emergency with significant morbidity and mortality if not recognized and treated promptly.
Etiology
| Type | Common Pathogens / Causes |
|---|---|
| Bacterial | S. pneumoniae (most common in adults), N. meningitidis, L. monocytogenes (neonates/elderly/immunocompromised), H. influenzae, E. coli, Group B Strep (neonates) |
| Viral (Aseptic) | Enteroviruses (most common), HSV-2, HIV, mumps, arboviruses, CMV |
| Fungal | Cryptococcus neoformans (esp. in HIV/immunocompromised), Histoplasma |
| Tuberculous | Mycobacterium tuberculosis |
| Non-infectious | Malignancy (carcinomatous meningitis), drugs (NSAIDs, TMP-SMX, IVIG), sarcoidosis, SLE |
Pathophysiology
(Harrison's, p. 1101–1102)
- Bacteria colonize the nasopharynx → bacteremia → blood-brain barrier disruption
- Bacterial components (LPS, teichoic acid) trigger cytokine release (TNF-α, IL-1)
- Cytokine-mediated inflammation → increased BBB permeability → cerebral edema
- Raised intracranial pressure (ICP) → impaired cerebral blood flow → neuronal injury
- Exudate accumulates in subarachnoid space → impairs CSF flow → hydrocephalus
Clinical Features
(Harrison's, p. 978, 1102)
Classic Triad (present in <50% of patients):
- Fever
- Nuchal rigidity (neck stiffness)
- Altered mental status
Other features:
- Headache (severe, progressive — most common symptom)
- Photophobia / phonophobia
- Nausea and vomiting
- Seizures (~30% of bacterial cases)
- Focal neurological deficits
Meningeal Signs:
- Kernig's sign: inability to fully extend the knee with the hip flexed to 90°
- Brudzinski's sign: passive neck flexion causes involuntary hip/knee flexion
- Jolt accentuation: worsening headache with horizontal head rotation at 2–3 Hz
Meningococcal-specific:
- Petechial/purpuric, non-blanching rash (septicemia) — a medical emergency
- May progress to Waterhouse-Friderichsen syndrome (adrenal hemorrhage, DIC)
Diagnosis
CSF Analysis (Lumbar Puncture) — Key Differentiator
| Parameter | Bacterial | Viral | Tuberculous | Fungal |
|---|---|---|---|---|
| Appearance | Turbid/purulent | Clear | Fibrin web/clear | Clear/turbid |
| Opening pressure | ↑↑ (>250 mmH₂O) | Normal/↑ | ↑ | ↑↑ |
| WBC | >1000 cells/μL (PMN) | 10–1000 (lymph) | 100–500 (lymph) | 10–500 (lymph) |
| Protein | ↑↑ (>100 mg/dL) | Normal/↑ | ↑↑ | ↑ |
| Glucose (CSF:serum) | ↓ (<0.4) | Normal | ↓↓ (<0.3) | ↓ |
| Gram stain | Positive ~60–90% | Negative | Negative (AFB stain) | India ink/Crypto Ag |
| Culture | Positive ~80% | Negative | Positive (slow) | Positive |
(Harrison's, p. 1102–1103)
Before LP: CT head is required first if any of:
- Papilledema
- New focal neurological deficit
- Severely depressed consciousness (GCS ≤10)
- Seizure history
- Immunocompromised
Do not delay antibiotics while waiting for CT/LP — if bacterial meningitis is suspected, treat immediately, then investigate.
Other Investigations
- Blood cultures (×2, before antibiotics if possible)
- CBC, CRP, procalcitonin, serum glucose, coagulation profile
- CT/MRI brain — evaluate complications, rule out other diagnoses
- PCR (bacterial, viral, TB) on CSF
- Cryptococcal antigen (serum + CSF in immunocompromised)
MRI Findings in Bacterial Meningitis
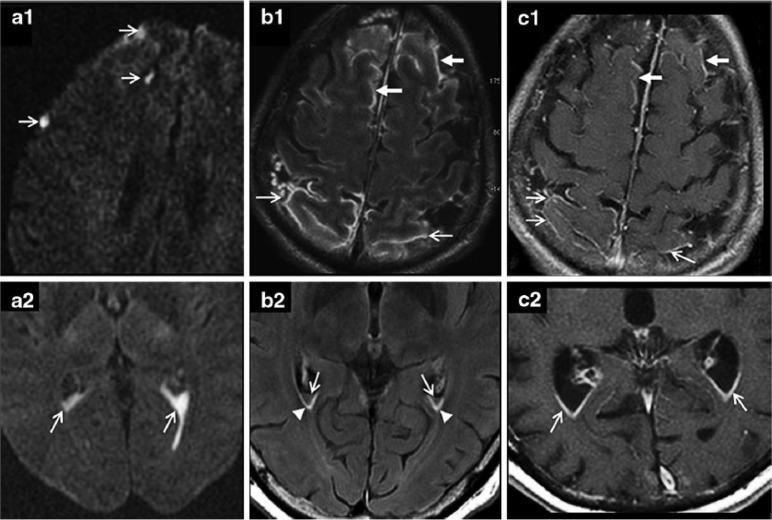
Axial MRI sequences in acute bacterial meningitis: (a) DWI showing hyperintense signals in cortical sulci and ventricular horns (diffusion restriction from intracranial/intraventricular pus); (b) FLAIR showing increased signal in frontal/parietal sulci and sub-ependymal lining (protein-enriched CSF); (c) Contrast-enhanced T1 showing leptomeningeal and ependymal enhancement. (Source: PMC Clinical VQA)
Management
Empirical Antibiotic Therapy
(Harrison's, p. 4159, Table 138-1)
| Patient Group | Empirical Regimen |
|---|---|
| Adults (18–50 yrs) | Ceftriaxone 2g IV q12h + Vancomycin 15–20 mg/kg IV q8–12h |
| >50 yrs / immunocompromised | Above + Ampicillin 2g IV q4h (covers Listeria) |
| Neonates | Ampicillin + Cefotaxime (or Gentamicin) |
| Penicillin allergy | Chloramphenicol ± Vancomycin; Meropenem |
Adjust antibiotics once cultures and sensitivities return.
Adjunctive Dexamethasone
- 0.15 mg/kg IV q6h × 4 days, given 15–20 min before or with the first dose of antibiotics
- Reduces TNF-α-mediated inflammation
- Most benefit in pneumococcal meningitis in adults (reduces hearing loss, mortality)
- Should NOT delay antibiotics
Supportive Care
- Elevate head of bed to 30°
- Strict fluid balance (avoid hypotension and hyponatremia — risk of SIADH)
- Seizure management (benzodiazepines acutely; consider prophylaxis)
- ICP management if raised (mannitol, hyperventilation, neurosurgery if needed)
- ICU monitoring for septic shock / DIC
Viral Meningitis
- Mostly supportive care
- Acyclovir 10 mg/kg IV q8h for HSV or VZV meningitis/encephalitis
- Antiretrovirals if HIV-associated
- Ganciclovir/Foscarnet for CMV (immunocompromised)
Cryptococcal Meningitis (HIV/Immunocompromised)
- Induction: Liposomal Amphotericin B + Flucytosine × 2 weeks
- Consolidation: Fluconazole 400mg/day × 8 weeks
- Maintenance: Fluconazole 200mg/day
- Serial LPs or lumbar drain for elevated ICP
Complications
(Harrison's, p. 1105–1106, 1200)
- Hearing loss (most common long-term sequela — especially pneumococcal)
- Hydrocephalus (communicating or obstructive)
- Cerebral venous sinus thrombosis
- Cerebral infarction / stroke
- Subdural effusion / empyema
- Cranial nerve palsies (II, III, VI, VII, VIII)
- Cognitive impairment / learning disability
- Septic shock, DIC, multi-organ failure (bacterial)
- Death — bacterial meningitis case fatality rate: ~20–30% for pneumococcal, ~5–10% for meningococcal
Prophylaxis / Prevention
| Indication | Intervention |
|---|---|
| Close contacts of meningococcal disease | Rifampicin 600mg BD × 2 days OR Ciprofloxacin 500mg single dose OR Ceftriaxone 250mg IM single dose |
| Vaccination | MenACWY, MenB vaccines (adolescents, asplenic patients, pilgrims) |
| Pneumococcal | PCV13/PPSV23 (elderly, immunocompromised, asplenic) |
| Hib | Routine childhood vaccination (virtually eliminated Hib meningitis in immunized populations) |
| Recurrent bacterial meningitis | Investigate for CSF leak or complement deficiency |
Differential Diagnosis
- Encephalitis (prominent altered consciousness, seizures, focal signs without meningismus)
- Subarachnoid hemorrhage (thunderclap headache, xanthochromia on LP)
- Brain abscess (focal signs, fever, CT ring-enhancing lesion)
- Migraine, tension headache
- Subdural empyema
- Malignant meningitis (cytology positive, low glucose)
Key teaching point: In any patient with fever + headache + neck stiffness, bacterial meningitis must be ruled out immediately. Blood cultures and empirical antibiotics should never be delayed for imaging or LP.
This is a shared conversation. Sign in to Orris to start your own chat.