Therapeutic status of drug cotrimoxazole
Reading File
Finding Sources
Finding Sources
Searching PubMed
cotrimoxazole trimethoprim sulfamethoxazole clinical uses
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the comprehensive information needed. Let me compile the full detailed answer.
Cotrimoxazole (Co-Trimoxazole / TMP-SMX) - Therapeutic Status
1. What Is It?
Cotrimoxazole is a fixed-dose combination of:
- Trimethoprim (TMP) + Sulfamethoxazole (SMX) in a 1:5 ratio (by weight)
- Brand names: Bactrim, Septra
- Formulations: Single-strength (SS): TMP 80 mg + SMX 400 mg; Double-strength (DS): TMP 160 mg + SMX 800 mg; IV solution: 80 mg TMP + 400 mg SMX per 5 mL
In much of the world, the combination of TMP with SMX is known as cotrimoxazole. - Goodman & Gilman's Pharmacological Basis of Therapeutics, 14th Ed.
2. Mechanism of Action
Cotrimoxazole achieves sequential blockade of the bacterial folate synthesis pathway - this is the basis of its synergy:
| Step | Drug | Enzyme Inhibited | Effect |
|---|---|---|---|
| Step 1 | Sulfamethoxazole (sulfonamide) | Dihydropteroate synthase (DHPS) | Blocks conversion of PABA → dihydropteroic acid |
| Step 2 | Trimethoprim | Dihydrofolate reductase (DHFR) | Blocks conversion of dihydrofolic acid → tetrahydrofolic acid |
The result: depletion of tetrahydrofolate → impaired synthesis of thymidylate, purines, and ultimately DNA.
- TMP is 100,000 times more selective for bacterial DHFR than mammalian DHFR, explaining its low toxicity in humans.
- Each drug alone is bacteriostatic; the combination is often bactericidal when the organism is sensitive to both.
- The formulation achieves a 20:1 plasma ratio of SMX:TMP (the optimal ratio for in vitro synergy).
3. Antimicrobial Spectrum
Susceptible organisms:
| Category | Organisms |
|---|---|
| Gram-positive cocci | S. aureus (MSSA and MRSA, >90%), S. pneumoniae (variable resistance), S. pyogenes |
| Gram-positive bacilli | Listeria monocytogenes |
| Gram-negative rods | E. coli (variable; resistance up to 30%+), H. influenzae, Proteus mirabilis, Klebsiella spp., Enterobacter spp., Salmonella, Shigella, Legionella pneumophila, Serratia spp., Stenotrophomonas maltophilia, Yersinia spp., Brucella abortus |
| Others | Pneumocystis jirovecii, Toxoplasma gondii, Nocardia asteroides, Cyclospora cayetanensis, Cystoisospora belli |
Intrinsically resistant: Pseudomonas aeruginosa, Bacteroides fragilis, enterococci, Mycoplasma, Chlamydia, spirochetes.
4. Therapeutic Uses (Clinical Applications)
A. Urinary Tract Infections (UTIs)
- TMP-SMX is effective for uncomplicated cystitis: DS tablet (160/800 mg) twice daily for 3 days
- For complicated UTI or pyelonephritis: 10-14 days
- Empiric use is NOT recommended if local E. coli resistance exceeds 20% or if the patient received TMP-SMX recently
- TMP concentrates in prostatic fluid (due to lipid solubility and the more acidic pH of prostatic secretions), making it effective for acute and chronic bacterial prostatitis
- Prophylaxis for recurrent UTIs: 1 SS tablet three times weekly
B. Pneumocystis jirovecii Pneumonia (PCP)
- Drug of choice for both treatment and prophylaxis
- Treatment: High-dose TMP 15-20 mg/kg/day + SMX 75-100 mg/kg/day IV or oral in 3-4 divided doses for 21 days; adjunctive corticosteroids for moderate-to-severe disease (PaO₂ <70 mmHg)
- Primary prophylaxis: CD4+ count <200 cells/μL in HIV patients - one DS tablet daily or three times weekly
- Secondary prophylaxis: Indefinitely in HIV until immune reconstitution
- IV route preferred for moderately severe to severe disease
C. Skin and Soft Tissue Infections
- Effective against MRSA skin and soft tissue infections (first-line alternative to doxycycline)
- Standard dose DS tablet twice daily; bone and joint infections due to S. aureus: 8-10 mg/kg/day of TMP component
D. Respiratory Tract Infections
- Acute exacerbations of chronic bronchitis (mild outpatient cases)
- Acute otitis media in children and acute maxillary sinusitis in adults (due to susceptible H. influenzae, S. pneumoniae)
- NOT recommended for streptococcal pharyngitis (does not eradicate organism)
E. Gastrointestinal Infections
- Shigellosis (alternative to fluoroquinolones; use only if susceptibility confirmed due to rising resistance)
- Typhoid / Salmonella (alternative therapy)
- Cyclospora cayetanensis infection - drug of choice
- Cystoisosporiasis (Isospora belli): 10-day course, followed by long-term suppression in immunosuppressed patients
- No longer routinely recommended for traveler's diarrhea due to widespread resistance
F. Nocardiosis
- TMP-SMX is the drug of choice for Nocardia asteroides infections (pulmonary, CNS, disseminated)
- High doses required, often combined with imipenem or amikacin for severe disease
G. Toxoplasmosis (Alternative therapy)
- Used as an alternative when pyrimethamine + sulfadiazine is not tolerated
- Also used for prophylaxis in HIV patients (same dose as PCP prophylaxis covers Toxoplasma as well)
H. Stenotrophomonas maltophilia
- Drug of choice for infections with this intrinsically multidrug-resistant organism
- High doses required (TMP 15-20 mg/kg/day IV)
I. Listeria infections
- Preferred alternative when patients cannot tolerate ampicillin (IV TMP-SMX)
J. Gram-negative Bacteremia
- Can treat bacteremia caused by susceptible Enterobacteriaceae; alternative for some MDR species (Enterobacter, Serratia)
K. Melioidosis (Burkholderia pseudomallei)
- TMP-SMX alone has been shown effective and better tolerated than TMP-SMX + doxycycline for eradication therapy
L. Pediatric Prophylaxis
- Standard prophylaxis agent in children with recurrent UTI, vesicoureteral reflux
- Children's dose: TMP 1-2 mg/kg/day (avoid in infants <2 months; risk of hyperbilirubinemia)
- Also used in pediatric HIV for OI prophylaxis (avoid <3 months)
5. Pharmacokinetics
| Parameter | TMP | SMX |
|---|---|---|
| Absorption | Well absorbed orally | Well absorbed orally |
| Peak concentration | ~2 h | ~4 h |
| Protein binding | ~40% | ~65% |
| Volume of distribution | Large (9× that of SMX) | Smaller |
| Half-life | ~11 h | ~10 h |
| CSF penetration | Good | Good |
| Urinary excretion | 50-60% in 24 h | 25-50% in 24 h |
| Plasma ratio achieved | 1 part TMP : 20 parts SMX | - |
- TMP concentrates in prostatic fluid, vaginal fluid (more acidic environments) and sputum - useful for site-specific infections
- Dose reduction required when CrCl is 15-30 mL/min (reduce by half); avoid if CrCl <15 mL/min
6. Bacterial Resistance
- Mechanisms:
- Point mutations in DHFR (TMP resistance) or DHPS (SMX resistance)
- Plasmid-encoded resistant DHFR (via transposons on conjugative plasmids - most common)
- Reduced cell wall permeability
- Overproduction of DHFR
- Resistance to the combination is lower than to either agent alone
- Growing resistance in E. coli (up to 30%+ in many regions) and S. pneumoniae limits empiric use
7. Adverse Effects
| Adverse Effect | Details |
|---|---|
| Hypersensitivity (sulfonamide allergy) | Rash, urticaria, Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis - most serious |
| Hematologic | Leukopenia, thrombocytopenia, megaloblastic anemia (folate antagonism) |
| Renal | Crystalluria (SMX), interstitial nephritis, elevated serum creatinine (TMP blocks tubular creatinine secretion - does not reflect true GFR decline) |
| GI | Nausea, vomiting, anorexia |
| Hepatic | Elevated transaminases, cholestatic jaundice |
| Hyperkalemia | TMP blocks ENaC channels in the collecting duct (similar to amiloride) |
| Hyponatremia | Reported with prophylactic use in children |
| Photosensitivity | Sulfonamide component |
| HIV patients | Higher rates of all hypersensitivity reactions, particularly rash |
8. Drug Interactions
| Drug | Interaction |
|---|---|
| Warfarin | Potentiates anticoagulant effect (SMX displaces from protein binding; inhibits CYP2C9) |
| Methotrexate | Increased toxicity (additive folate antagonism; competition for renal tubular secretion) |
| Phenytoin | Increased phenytoin levels |
| Cyclosporine | Reduced cyclosporine levels; increased nephrotoxicity |
| ACE inhibitors / K-sparing diuretics | Additive hyperkalemia risk (TMP's amiloride-like effect) |
| Digoxin | Increased digoxin levels in elderly |
9. Contraindications
- Allergy to sulfonamides or trimethoprim
- Infants <2 months (risk of kernicterus - sulfonamides displace bilirubin from albumin)
- Pregnancy (especially first and third trimesters): folate antagonism risks neural tube defects; risk of neonatal hemolysis and hyperbilirubinemia at term
- Megaloblastic anemia due to folate deficiency
- Severe renal or hepatic impairment (relative contraindication)
10. Summary of Therapeutic Status
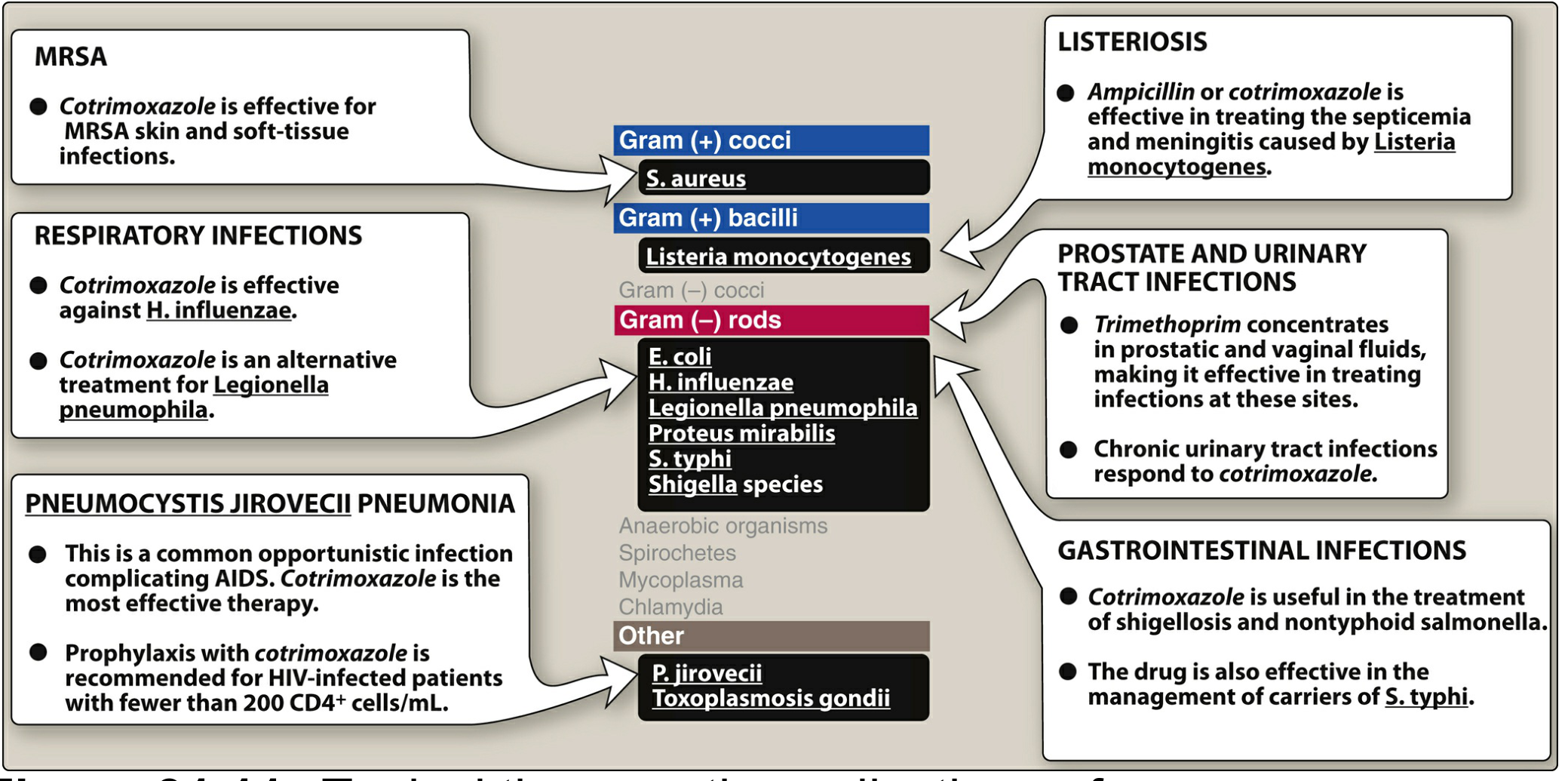
Figure: Typical therapeutic applications of cotrimoxazole (from Lippincott Illustrated Reviews Pharmacology)
Cotrimoxazole remains a first-line or major alternative drug for several key infections. Its unique coverage of P. jirovecii and Nocardia, combined with activity against MRSA skin infections and many common gram-negative pathogens, makes it one of the most versatile inexpensive antibiotics available. However, rising resistance among E. coli and S. pneumoniae limits empiric use in UTIs and pneumonia in many regions.
Sources:
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th Ed., Chapter 57 (TMP-SMX section)
- Katzung's Basic and Clinical Pharmacology, 16th Ed., Chapter 46
- Lippincott Illustrated Reviews: Pharmacology, Chapter 31
This is a shared conversation. Sign in to Orris to start your own chat.