Orthopaedic manifestations bone fragility and fractures fractures heal in normal fashion initially but the bone does not remodel can lead to progressive bowing ligamentous laxity short stature scoliosis codfish vertebrae (compression fx) basilar invagination olecranon apophyseal avulsion fx most common first presenting sign coxa vara (10%) congenital anterolateral radial head dislocations explain me conceptually orthopaedic manifestations of osteogenesis imperfecta
Reading File
search_medical_text
osteogenesis imperfecta orthopaedic manifestations bone fragility fractures bowing scoliosis
search_medical_image
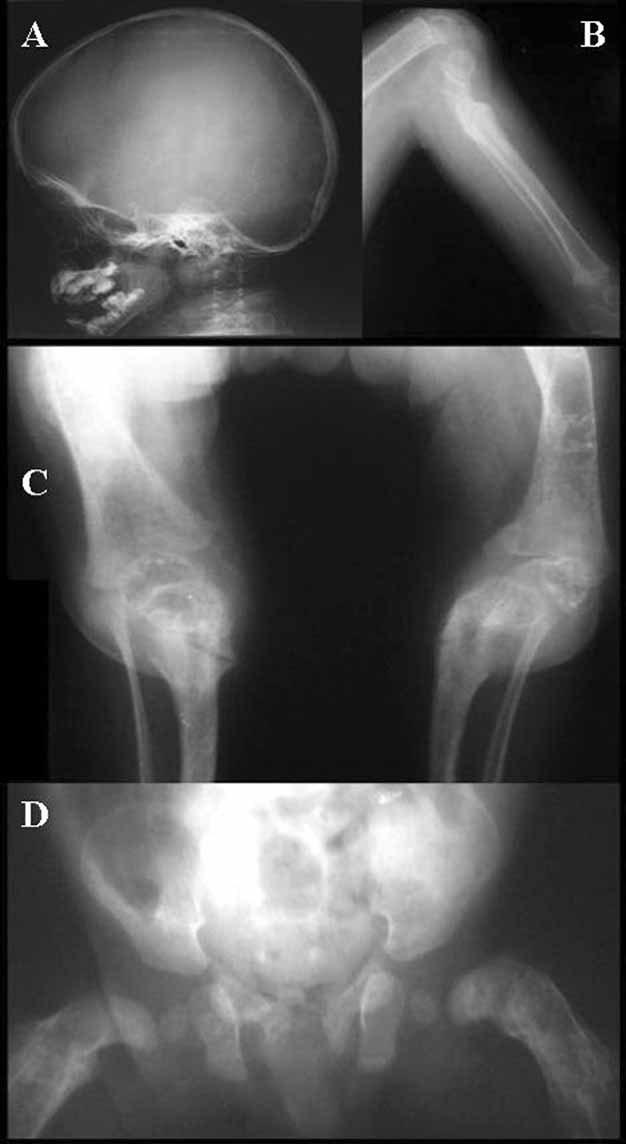
osteogenesis imperfecta codfish vertebrae coxa vara bowing deformity
GradeResponse
GradeResponse
Here is a conceptual breakdown of every orthopaedic manifestation you listed, organized around the underlying pathophysiology.
Osteogenesis Imperfecta — Orthopaedic Manifestations
The Core Defect (Conceptual Foundation)
OI is fundamentally a type I collagen disorder. Collagen is the scaffolding onto which hydroxyapatite crystals are deposited to form bone. When that scaffold is defective (either structurally abnormal or quantitatively deficient), the resulting bone has two inseparable problems:
- Decreased bone mass — less material
- Increased brittleness — the material that exists is poorly organized
This combination produces a bone that breaks easily and remodels abnormally — and every orthopaedic manifestation flows from one or both of these.
1. Bone Fragility & Fractures
| Concept | Explanation |
|---|---|
| Why fractures occur easily | Defective collagen scaffold → poor mineralization → bone cannot withstand normal mechanical loads |
| Why fractures heal "normally initially" | The inflammatory and proliferative phases of fracture healing (callus formation) do NOT depend on pre-existing collagen quality — cells still respond, hematoma still forms, woven bone still appears |
| Why remodeling fails | Remodeling requires osteoblast-osteoclast coupling on a collagen template. The template is defective, so the woven bone is never replaced by organized lamellar bone → bone remains weak at the fracture site |
Key concept: OI fractures are not a healing failure — they are a remodeling failure. The fracture "heals" mechanically but the bone never regains normal architecture.
2. Progressive Bowing
Conceptually, bowing is the result of recurrent fractures + abnormal remodeling + gravity + muscle forces acting on bones that cannot self-correct:
- Each fracture heals with slight angular malunion (because the remodeling capacity to straighten it is absent)
- Weight-bearing forces then act on the angulated bone, causing further deformation
- This is most dramatic in the femora and tibiae — the lower limbs carry load and the bone literally bends under physiologic stress over time
3. Ligamentous Laxity
OI is a collagen disorder of all connective tissue, not just bone. Ligaments are also composed of type I collagen, so they are structurally weak and over-compliant. This leads to hypermobile joints, joint instability, and contributes to progressive deformity.
4. Short Stature
Multiple compounding mechanisms:
- Recurrent fractures → long bones never achieve normal length
- Compression fractures of vertebrae → loss of axial height
- Progressive bowing → functional limb shortening
- Underlying growth plate dysfunction from collagen deficiency
5. Scoliosis
The spine is vulnerable for several interconnected reasons:
- Vertebral body weakness → wedging → asymmetric collapse drives curvature
- Ligamentous laxity → poor spinal stability → the spine drifts
- Muscle weakness (secondary to disuse and recurrent fractures) → reduced dynamic support
- Scoliosis is progressive and can compromise pulmonary function (a major cause of morbidity in OI)
6. Codfish Vertebrae (Compression Fractures)
- The intervertebral disc is made of nucleus pulposus, which is under hydrostatic pressure and is much stronger than the adjacent weakened OI vertebral bodies
- The disc therefore bulges symmetrically into both end-plates of the weak vertebral body above and below, creating the classic biconcave "codfish" shape
- This is a compression fracture equivalent in OI, not a disc herniation
7. Basilar Invagination
- The skull base is also made of collagen-dependent bone
- In OI, the occiput softens and the foramen magnum region gradually invaginates upward under the weight of the skull
- The odontoid process of C2 can then protrude into the foramen magnum → brainstem compression
- This is a life-threatening complication unique to OI among the skeletal dysplasias
8. Olecranon Apophyseal Avulsion Fracture — Most Common First Sign
This is a pathognomonic and pedagogically important point:
- At the olecranon, the triceps tendon attaches to the apophysis (a traction epiphysis)
- Normally, a child pulling to stand or throwing a ball generates tensile force at this site — the bone should easily resist this
- In OI, the weakened bone avulses at physiologic loads — a force that would not fracture normal bone
- This is often the first fracture that brings the child to medical attention, because it occurs with trivial activity and is anatomically unusual (avulsion fractures are rare in normal children)
- It serves as a red flag for an underlying bone fragility disorder
9. Coxa Vara (~10%)
Coxa vara = the neck-shaft angle of the femur is less than 120° (normally ~130°).
Mechanism in OI:
- The femoral neck is under continuous bending stress from body weight
- In normal bone, this is resisted easily; in OI, the weakened femoral neck gradually bends (plastic deformation + repeated microfractures) into a varus position
- This worsens gait, increases the lever arm on the abductors, and can progress to a shepherd's crook deformity in severe cases
10. Congenital Anterolateral Radial Head Dislocation
- Ligamentous laxity (from defective collagen in the annular ligament) is the primary driver
- The radial head is not held tightly within its socket → it subluxes/dislocates
- Anterolateral direction is the typical direction of dislocation in OI
- This is often missed clinically because elbow range of motion may be preserved, but it can eventually cause pain, limited forearm rotation, and a prominent lateral elbow bump
Summary Concept Map
Defective Type I Collagen
|
┌────┴─────┐
BONE (scaffold) SOFT TISSUE (ligaments)
| |
Poor mineralization Ligamentous laxity
Decreased mass → Joint instability
Increased brittleness → Radial head dislocation
|
┌────┴──────────────────────┐
FRACTURES DEFORMITY
• Olecranon avulsion (1st) • Bowing (femur, tibia)
• Recurrent long bone fx • Coxa vara
• Compression fx • Scoliosis
• Codfish vertebrae • Short stature
|
Abnormal remodeling
|
Progressive angulation → Bowing worsens
|
Axial skeleton involvement
|
Basilar invagination (skull base softening)
Every manifestation is mechanistically connected to the single upstream defect: collagen that cannot provide adequate tensile scaffolding for bone or soft tissue. (Harrison's, p. 11733)
This is a shared conversation. Sign in to Orris to start your own chat.