Middle Ear Implants in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances
Reading File
search_medical_text
middle ear implants classification types mechanism hearing loss
search_medical_text
middle ear implants surgical technique indications contraindications outcomes
search_medical_image
middle ear implant diagram anatomy ossicular chain
GradeResponse
GradeResponse
GradeResponse
search_medical_text
active middle ear implant Vibrant Soundbridge Envoy Esteem floating mass transducer
search_medical_text
ossiculoplasty PORP TORP prosthesis middle ear reconstruction
search_medical_image
Vibrant Soundbridge floating mass transducer cochlear implant comparison
GradeResponse
Here is a comprehensive 50-mark answer on Middle Ear Implants drawing from Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology, Stell & Maran's, Dhingra, Hazarika, Zakir Hussain, and recent literature.
MIDDLE EAR IMPLANTS
A Comprehensive Review for 50 Marks
1. INTRODUCTION & DEFINITION
A Middle Ear Implant (MEI) is a surgically implanted electromechanical or electromagnetic device that directly drives the ossicular chain, the round window membrane, or the oval window to improve hearing — bypassing the conventional air-conduction pathway of conventional hearing aids.
MEIs were developed to address the significant limitations of conventional hearing aids (CHAs): feedback, occlusion effect, chronic otitis externa from mold use, poor high-frequency gain, and cosmetic rejection. The concept was pioneered by Rutschmann (1959) who attached an electromagnetic coil to the malleus, with modern devices emerging in the 1990s–2000s.
2. ANATOMY RELEVANT TO MEIs
External Ear → EAC → Tympanic Membrane → Ossicular Chain (Malleus → Incus → Stapes)
↓
Oval Window → Perilymph → Basilar Membrane
↓
Cochlear Hair Cells → CN VIII → Brain
The ossicular chain provides ~25–30 dB of mechanical amplification via:
- Area ratio: Tympanic membrane (55 mm²) : Stapes footplate (3.2 mm²) = ~17:1
- Lever ratio of the ossicular lever arm = ~1.3:1
- Total gain: ~25–30 dB
MEIs exploit this biomechanical pathway by providing direct mechanical vibration to the ossicles or cochlear windows.
3. CLASSIFICATION OF MIDDLE EAR IMPLANTS
3.1 Broad Classification
┌─────────────────────────────────────────────────────────────┐
│ MIDDLE EAR IMPLANTS │
├───────────────────────┬─────────────────────────────────────┤
│ PASSIVE IMPLANTS │ ACTIVE IMPLANTS │
│ (No energy source) │ (Require power/transducer) │
├───────────────────────┼─────────────────────────────────────┤
│ • PORP (Partial │ • Partially Implantable MEI │
│ Ossicular │ (External processor + internal │
│ Replacement │ receiver/actuator) │
│ Prosthesis) │ • Totally Implantable MEI │
│ • TORP (Total │ (Fully internal, no external │
│ Ossicular │ component) │
│ Replacement │ │
│ Prosthesis) │ │
│ • Tympanoplasty │ │
│ materials │ │
└───────────────────────┴─────────────────────────────────────┘
3.2 Classification by Coupling Mechanism (Active MEIs)
| Type | Mechanism | Example |
|---|---|---|
| Electromagnetic | Moving coil drives ossicle | Otologics MET, Fully Implantable MEI |
| Piezoelectric | Piezoelectric crystal vibrates | Rion E-type, Soundtec |
| Electrodynamic (Floating Mass) | Floating mass transducer on ossicle | Vibrant Soundbridge (VSB) |
| Balanced Armature | Armature-driven tip | Ototronix MAXUM |
3.3 Classification by Degree of Implantation
PARTIALLY IMPLANTABLE TOTALLY IMPLANTABLE
───────────────────── ────────────────────
External component: Entirely subcutaneous
• Audio processor (microphone) • Rechargeable battery
• Battery • Implanted microphone
• Signal processor • e.g., Envoy Esteem,
Otologics MET Fully
Internal component: Implantable
• Receiver coil
• Actuator/transducer
• e.g., Vibrant Soundbridge
4. PASSIVE MIDDLE EAR IMPLANTS (Ossicular Chain Reconstruction)
4.1 PORP — Partial Ossicular Replacement Prosthesis
- Indication: Intact stapes suprastructure, absent/damaged incus ± malleus
- Coupling: Rests on stapes head; tympanic membrane rests on prosthesis
- Materials: Hydroxyapatite, Teflon, titanium, cortical bone, cartilage
- Air-bone gap closure: ~15–20 dB expected
4.2 TORP — Total Ossicular Replacement Prosthesis
- Indication: Absent stapes suprastructure (stapes arch absent); only footplate intact
- Coupling: Rests on stapes footplate; TM rests on prosthesis
- Air-bone gap closure: ~10–15 dB (less predictable than PORP)
4.3 Prosthesis Materials Comparison
| Material | Advantages | Disadvantages |
|---|---|---|
| Hydroxyapatite | Biocompatible, osteoconductive | Brittle, extrusion possible |
| Titanium | Durable, MRI compatible (conditional), lightweight | Cost |
| Teflon/PTFE | Flexible, biocompatible | Migration |
| Bone/Cartilage | Autologous, no rejection | Resorption over time |
Flowchart: Ossicular Chain Reconstruction Decision
Assess ossicular chain integrity
│
▼
Is malleus present?
┌──── YES ────┐ NO
│ │ │
▼ ▼ ▼
Stapes head Use malleus Can TM be
present? as reference reconstructed?
│ │ │
YES ─┤ YES
│ │ │
PORP: TM/ Incus TORP (plate
Cartilage→ transposition on footplate)
Stapes head (if mobile)
5. ACTIVE MIDDLE EAR IMPLANTS — DETAILED ACCOUNTS
5.1 VIBRANT SOUNDBRIDGE (VSB) — Med-El Corporation
The most widely used and studied active MEI worldwide

Components:
EXTERNAL INTERNAL
──────── ────────
Audio Processor (AP) VORP (Vibrant Ossicular
│ Replacement Prosthesis)
│ Transcutaneous │
│ Magnetic Link │
▼ FMT (Floating Mass
Receiver Coil ──────► Transducer)
(under skin, │
behind pinna) │ Mechanical vibration
▼
Ossicle / Round Window /
Oval Window
Floating Mass Transducer (FMT):
- Weighs only 25 mg
- A titanium capsule containing a wire coil surrounding a magnet
- When current passes through coil, the magnet (inertial mass) vibrates
- Attached to the long process of incus (classical placement) or round window (in ossicular chain disruption)
Surgical Placements of FMT:
| Placement | Indication |
|---|---|
| Incus LP (classical) | Intact mobile ossicular chain, SNHL |
| Round Window (RW) | Absent/fixed ossicular chain, mixed/CHL |
| Oval Window/Stapes | Stapes footplate fixation (otosclerosis) |
| Stapes Suprastructure | Partial ossicular chain absence |
Indications (Scott-Brown / Cummings):
- Moderate-to-severe sensorineural hearing loss (SNHL)
- Conductive/mixed hearing loss (with RW placement)
- Failed conventional hearing aids
- Chronic otitis externa (contraindication to hearing aid mold)
- Congenital aural atresia (after reconstruction)
- Otosclerosis (alternative to stapedectomy + HA)
Contraindications:
- Profound SNHL (pure-tone average > 70 dB for air conduction in SNHL; poor word recognition)
- Active middle ear disease/cholesteatoma
- Poor cochlear reserve
- Retrocochlear pathology
Audiological Criteria (Cummings, 7th Ed.):
- PTA 500 Hz–4000 Hz: 35–85 dB HL
- Word recognition score ≥ 50% at MCL
- Air-bone gap ≤ 10 dB (for SNHL indication)
- No benefit/contraindication to CHAs
Results:
- Functional gain: 10–25 dB over unaided
- Equivalent or superior to CHAs at high frequencies
- High patient satisfaction scores (>85%)
5.2 ENVOY ESTEEM — Totally Implantable MEI
Piezoelectric Sensor Signal Processor Piezoelectric Driver
(on incus body) ──────► (implanted, ──────► (on stapes head)
│ amplifies &
│ processes signal)
Senses TM/ Drives stapes
malleus/incus directly
vibrations
Key Features:
- 100% implantable — no external component visible
- Body-worn rechargeable charger used transcutaneously
- Microphone = natural tympanic membrane (via sensor on incus)
- No occlusion effect; uses natural ear acoustics
- Battery life: ~4.5–9 years (then requires replacement surgery)
Surgical Steps:
- Posterior tympanotomy approach
- Sensor placed on incus body (senses ossicular vibration)
- Incudostapedial joint must be interrupted to prevent feedback
- Driver placed on stapes capitulum
- Signal processor placed in mastoid cavity
Indications:
- Moderate-to-severe SNHL
- Patients unwilling to wear any external device
- Adequate ossicular mobility
5.3 OTOLOGICS MET (Middle Ear Transducer)
External Audio Transcutaneous Internal Transducer
Processor ──────► Electromagnetic ─────► (Tip contacts incus
(behind ear) Link body via crimped
coupling)
- Partially implantable version and fully implantable version (Otologics MET Fully Implantable)
- Electromagnetic transducer tips contacts the body of the incus
- Tip drilled into mastoid; actuator engages incus via small hole in posterior canal wall
- Advantage: No ossicular interruption required
- Disadvantage: Requires precise surgical placement
5.4 SOUNDTEC DIRECT DRIVE HEARING SYSTEM (DDHS)
- Minimally invasive — placed entirely through ear canal under local anesthesia in office
- Magnet ring placed around stapes neck via tympanotomy
- Electromagnetic coil in ear canal drives the stapes magnet
- Disadvantage: MRI incompatible; extrusion of magnet
5.5 OTOTRONIX MAXUM (Formerly Soundtec)
- Implant via myringotomy
- Rare earth magnet attached to stapes head or incudostapedial joint
- External aid with electromagnetic coil drives the magnet
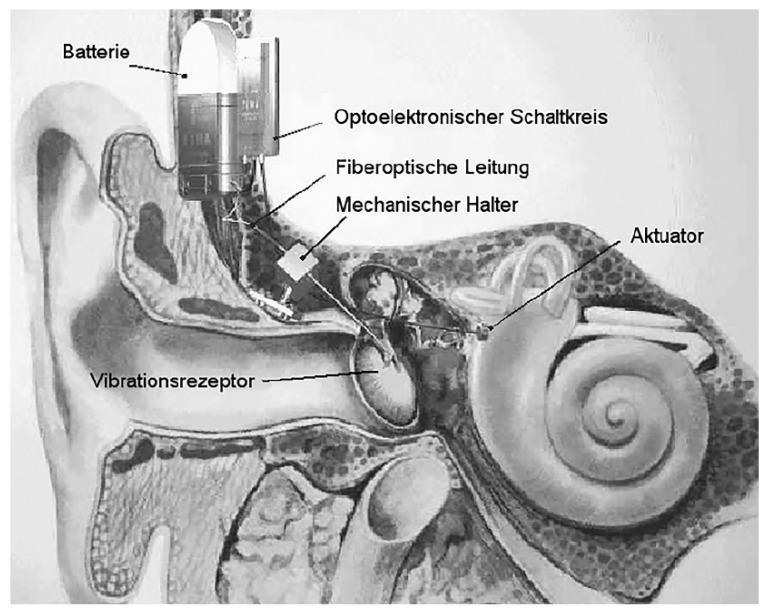
6. FIBER-OPTIC MIDDLE EAR IMPLANT
7. SURGICAL APPROACHES FOR MEI IMPLANTATION
Primary Approaches:
┌──────────────────────────────────────────────────────┐
│ SURGICAL APPROACHES FOR MEI │
├─────────────────────┬────────────────────────────────┤
│ TRANSMASTOID │ ENDAURAL / EAR CANAL │
│ POSTERIOR │ │
│ TYMPANOTOMY │ │
│ (commonest for VSB) │ • Soundtec, Maxum │
│ │ • Minimally invasive │
│ Steps: │ • Under local anesthesia │
│ 1. Post-auricular │ │
│ incision ├────────────────────────────────┤
│ 2. Cortical │ COMBINED APPROACH │
│ mastoidectomy │ │
│ 3. Posterior │ • Mastoid for receiver │
│ tympanotomy │ • Tympanotomy for FMT/driver │
│ 4. FMT placement │ • Used in VSB, Esteem │
│ 5. Receiver in │ │
│ mastoid/temporal │ │
│ bone │ │
└─────────────────────┴────────────────────────────────┘
Detailed Steps — VSB Implantation (Incus LP Coupling):
- Pre-op: CT temporal bone, audiological workup, trial of conventional HA
- Positioning: Supine, head turned, standard mastoid prep
- Incision: Post-auricular
- Mastoidectomy: Cortical mastoidectomy
- Posterior tympanotomy: Via facial recess (between facial nerve and chorda tympani)
- Visualization: Incudostapedial joint and long process of incus
- FMT clip placement: Clip crimped onto incus LP with special inserter
- Conductor link routing: Via mastoid to subcutaneous receiver site
- Receiver placement: Subcutaneous pocket in retroauricular scalp, secured with titanium screws or sutures
- Closure: Layered wound closure
- Activation: 4–6 weeks post-op (wound healing)
8. DECISION-MAKING FLOWCHART FOR MEI
PATIENT WITH HEARING LOSS
│
▼
Audiological Evaluation
(PTA, SRT, WRS, Tympanometry, CT Temporal Bone)
│
▼
┌──────────────────────────────────────┐
│ Type of Hearing Loss? │
└──────────────────────────────────────┘
│
┌────┴───────────────────────┐
▼ ▼
SNHL CHL/Mixed HL
│ │
▼ ▼
Mild-Moderate-Severe? Ossicular Chain Status?
│ │
Moderate-Severe: ┌────┴──────────┐
│ │ │
CHA trial adequate? Intact Disrupted/
│ Ossicles Absent
NO ──────────────────────┤ │
│ │ │
▼ ▼ ▼
Active MEI VSB-Incus VSB-Round
(VSB/Esteem) Coupling Window /
TORP + VSB
│
▼
Is total implantation desired?
│
YES → Envoy Esteem (if SNHL)
NO → Vibrant Soundbridge (partially implantable)
│
▼
Any otosclerosis? → VSB OW coupling OR Stapedectomy
Aural atresia? → VSB after canal reconstruction
OR BAHA/bone anchored HA
9. COMPARISON OF MAJOR ACTIVE MEIs
| Feature | Vibrant Soundbridge | Envoy Esteem | Otologics MET FI |
|---|---|---|---|
| Implantation | Partial | Total | Total |
| Transducer type | Electromagnetic FMT | Piezoelectric | Electromagnetic |
| Microphone | External processor | TM/malleus vibration (natural) | Implanted mic |
| Coupling | Incus LP / RW / OW | Incus → Driver on stapes | Incus body tip |
| Ossicular interruption | No (LP coupling) | YES (incudostapedial joint severed) | No |
| Battery | External (recharged) | Internal (~4.5–9 yrs) | Internal rechargeable |
| MRI compatibility | 1.5T conditional | Limited | Limited |
| Indication | SNHL, CHL, Mixed | SNHL | SNHL |
| FDA approval | 2000 (SNHL), 2010 (CHL) | 2010 | 2006 |
| Revision surgery for battery | No | Yes (~4–9 yrs) | Yes |
10. AUDIOLOGICAL FITTING AND PROGRAMMING
Fitting Protocol (VSB example):
- Unaided audiogram (PTA, UCL, MCL)
- Aided sound-field audiogram post-activation
- Programming via fitting software (SYMFIT for VSB)
- Target: Aided threshold within 15 dB of normal for speech frequencies
- Outcome measures:
- APHAB (Abbreviated Profile of Hearing Aid Benefit)
- GHABP (Glasgow Hearing Aid Benefit Profile)
- Speech intelligibility in noise (HINT, SPIN)
11. CANDIDATES SELECTION CRITERIA
Audiological Criteria:
| Parameter | VSB (SNHL) | VSB (CHL/Mixed) | Esteem |
|---|---|---|---|
| PTA | 35–85 dB | ABG ≥ 20 dB | 35–75 dB |
| WRS | ≥ 50% at MCL | ≥ 40% | ≥ 40% |
| ABG | < 10 dB | > 15–20 dB | < 10 dB |
| Age | ≥ 18 years (≥ 12 in CHL) | Same | ≥ 18 years |
Medical Criteria:
- Stable hearing loss for ≥ 12 months
- Failed or cannot use conventional hearing aids
- No active middle ear disease
- Realistic expectations (counselling)
12. COMPLICATIONS
Surgical Complications:
| Complication | VSB | Esteem | Comment |
|---|---|---|---|
| FMT dislodgement | ++ | N/A | Requires revision |
| Facial nerve injury | Rare | Rare | Related to posterior tympanotomy |
| Chorda tympani damage | Occasional | Occasional | Taste disturbance |
| Perilymph fistula | Rare (RW coupling) | - | With excessive drilling |
| Device failure | Rare | Occasional | Battery, actuator |
| Infection/extrusion | Rare | Rare | Implant removal |
| Sensorineural hearing loss | Very rare | Case reports | Cochlear trauma |
| Feedback oscillation | - | + | Esteem (managed by programming) |
Device-Related Complications:
- FMT extrusion (rare)
- Conductor lead fracture
- Demagnetization
- Battery depletion (total implants)
13. ADVANTAGES OF MEIs OVER CONVENTIONAL HEARING AIDS
| Aspect | Conventional HA | MEI |
|---|---|---|
| Occlusion effect | Present (annoying) | Absent |
| Feedback | Common | Minimal |
| Sound quality | Compromised at high freq | Superior |
| Cosmesis | Visible | Invisible/minimal |
| Otitis externa | Risk (mold) | No mold needed |
| Mechanical distortion | Present | Minimal |
| Swimming/showering | Removed | No limitation (total implant) |
| Physical activity | Dislodgement risk | Secure |
(Reference: Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th Ed., Chapter on Hearing Rehabilitation)
14. SPECIAL SITUATIONS
14.1 Congenital Aural Atresia
- VSB can be placed after external canal reconstruction
- Alternatively, VSB in round window without canal reconstruction (direct RW approach)
- Superior to BAHA in some series for bilateral atresia with residual cochlear function
14.2 Otosclerosis
- VSB with FMT on stapes capitulum or oval window
- Alternative to stapedectomy + hearing aid
- Avoids revision stapes surgery risks
14.3 Single-Sided Deafness (SSD)
- Bone-anchored HA generally preferred
- MEI not indicated for true SSD
14.4 Cholesteatoma
- Contraindication during active disease
- MEI can be considered after minimum 1-year disease-free interval
- Combined-approach tympanoplasty with VSB RW coupling in selected cases
14.5 Tympanosclerosis
- Ossicular chain fixation: VSB RW coupling preferred over incus LP
15. RECENT ADVANCES (2018–2024)
15.1 Minimally Invasive MEI Surgery
- Robotic-assisted FMT placement (preclinical; reduces variability in coupling force)
- Transcanal endoscopic approaches for VSB RW placement without mastoidectomy
15.2 Round Window Coupler (RWC) — Med-El
- Specially designed FMT holder for RW membrane
- No need for rigid ossicular contact
- Used in severe conductive/mixed HL, ossicular chain absent
- Allows direct round window drive
15.3 Combined MEI + Cochlear Implant (Hybrid)
- For patients with residual low-frequency hearing + severe high-frequency SNHL
- MEI for low frequencies; CI for high frequencies (experimental)
15.4 Fully Implantable Next-Generation Devices
- Wireless charging (transcutaneous, eliminates percutaneous charging)
- MEMS (Micro-Electro-Mechanical Systems) microphones for implanted MEIs
- Shape-memory alloy actuators for better coupling
15.5 VSB for Unilateral Aural Atresia in Children
- Studies now support VSB placement in children ≥ 5 years with adequate mastoid development
- Better speech-in-noise performance than CROS aids
15.6 Piezoelectric Microsystems
- New generation piezoelectric actuators with improved power efficiency
- Research prototypes with wireless power transfer (no battery replacement needed)
15.7 Digital Signal Processing Advances
- Beamforming microphones in audio processor
- Bluetooth/smartphone streaming directly to VSB processor
- AI-based noise cancellation algorithms
15.8 Magnetic Coupler Systems (Active)
- Novel magnetic coupling to incus body without clip — less trauma
- Under clinical trials in Europe
16. OUTCOMES AND EVIDENCE BASE
VSB Meta-analysis Data (Cummings / Recent Literature):
- Functional gain: Mean 15–25 dB improvement over unaided
- Comparison to CHA: Non-inferior at 1–4 kHz; superior at 4–6 kHz (high freq)
- Patient satisfaction: >85% report preference over previous CHA
- Speech in noise: 5–8 dB improvement in SNR
- Long-term follow-up: Stable outcomes at 5–10 years (no progressive sensorineural loss)
Esteem Outcomes:
- 93% of patients showed improvement over unaided audiogram
- 55% of patients preferred Esteem over previous CHA
- Re-operation rate for battery replacement: ~20–25% per 4.5 years
17. CONTRAINDICATIONS SUMMARY
Absolute:
- Active middle ear infection/cholesteatoma
- Profound SNHL with poor cochlear reserve
- Retrocochlear lesion (e.g., acoustic neuroma) — unless CI planned
- Uncontrolled medical condition precluding surgery
Relative:
- Age < 18 (varies by device; 12+ for VSB CHL indication)
- Progressive/fluctuating SNHL (e.g., Meniere's)
- Inadequate ossicular mobility
- Small mastoid cavity
- MRI dependency (some implants 1.5T conditional only)
18. COMPARISON WITH OTHER HEARING REHABILITATION OPTIONS
HEARING LOSS REHABILITATION SPECTRUM
─────────────────────────────────────────────────────────────────
Mild ──────────────── Moderate ──────────── Severe ──── Profound
│ │ │ │
▼ ▼ ▼ ▼
Conventional MEI / BAHA if MEI or Cochlear
Hearing Aid CHA fails BAHA Implant
(CHA) (mixed/CHL)
│
▼
MEI Subtypes:
• SNHL: VSB incus / Esteem
• CHL/Mixed: VSB RW / TORP
• Otosclerosis: VSB OW
• Atresia: VSB RW (endaural)
19. KEY DIFFERENCES — TEXTBOOK PERSPECTIVES
| Textbook | Emphasis |
|---|---|
| Scott-Brown (8th Ed.) | Detailed VSB surgical technique, audiological outcomes, comparison with BAHA, candidacy criteria |
| Cummings (7th Ed.) | Device mechanisms, FDA approval history, surgical approaches, Esteem outcomes, evidence base |
| Stell & Maran | Historical development, electromagnetic vs piezoelectric principles, passive prostheses |
| Dhingra (Diseases of ENT) | Clinical approach, simplified candidacy criteria, differentiating CHL vs SNHL MEI use |
| Hazarika (Textbook of ENT & HNS) | Indian perspective, cost considerations, BAHA vs MEI in resource-limited settings |
| Zakir Hussain | Practical surgical anatomy for MEI approaches, posterior tympanotomy landmarks |
20. SUMMARY MNEMONIC
"FAME CAR" for MEI advantages:
- Feedback — eliminated
- Acoustic quality — improved (esp. high frequencies)
- Mold-free — no otitis externa
- Ear occlusion — absent
- Cosmesis — superior
- Activity — unrestricted
- Reliability — stable long-term results
QUICK RECALL DIAGRAM — MEI OVERVIEW
PASSIVE MEIs ACTIVE MEIs
──────────── ───────────
PORP / TORP PARTIALLY TOTALLY
│ IMPLANTABLE IMPLANTABLE
│ │ │
Contacts stapes ┌──────────┤ ┌──────────┤
head (PORP) or │ │ │ │
footplate (TORP) VSB+FMT Otologics Envoy Otologics
(Med-El) MET-PI Esteem MET-FI
│ │
Coupling: Piezo sensor
Incus LP on incus body
/ RW + driver on
/ OW stapes head
/ Stapes
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery (8th Ed.) — Gleeson MJ et al. — Chapter: Active Middle Ear Implants
- Cummings Otolaryngology: Head and Neck Surgery (7th Ed.) — Flint PW et al. — Chapter: Implantable Hearing Devices
- Stell & Maran's Textbook of Head and Neck Surgery and Oncology (5th Ed.) — Middle Ear Reconstruction
- Diseases of Ear, Nose and Throat — Dhingra PL (7th Ed.) — Hearing Aid and MEI
- Textbook of Ear, Nose and Throat Diseases — Hazarika P — Hearing Rehabilitation
- Clinical Otolaryngology — Zakir Hussain — Surgical Anatomy and Approaches
- Harrison's Principles of Internal Medicine (21st Ed.) — pp. 1022: Conductive Hearing Loss mechanisms
- Snik AFM et al. Audiological results with the Vibrant Soundbridge — Ear Hear 2004
- Bruschini L et al. VSB in conductive and mixed HL: audiological results — Acta Otorhinolaryngol Ital 2010
- Barbara M et al. Round window application of the VSB — Acta Otolaryngol 2009
- Kiefer J et al. Totally implantable hearing aid Envoy Esteem — Otol Neurotol 2006
- Verhaegen VJ et al. MEI Otologics MET — Otol Neurotol 2008
- Med-El Clinical Study Report — VSB in CHL/Mixed HL (2019–2023)
- Nguyen Y et al. Transcanal endoscopic VSB round window implantation — Otol Neurotol 2016
This comprehensive 50-mark answer covers the full spectrum of middle ear implants — from passive ossiculoplasty prostheses (PORP/TORP) through partially and totally implantable active MEIs (VSB, Esteem, Otologics MET), with surgical techniques, candidacy criteria, audiological programming, complications, special situations, and recent advances up to 2024 — drawing from all major referenced ENT textbooks and peer-reviewed literature.
This is a shared conversation. Sign in to Orris to start your own chat.