Now I have sufficient information to compile a comprehensive, exam-grade 50-mark answer. Let me synthesize everything from the textbooks and my knowledge base.
External Ear Canal Cholesteatoma (EECC)
A Comprehensive 50-Mark Review
1. DEFINITION
External Ear Canal Cholesteatoma (EECC) is a benign, locally destructive lesion of the external auditory canal (EAC), characterized by an accumulation of exfoliated keratin debris within a keratinizing squamous epithelial sac that has lost its normal migratory capacity. Despite the suffix "-oma," it is not a true neoplasm but a dyskeratotic process.
Key distinction: Unlike middle ear cholesteatoma, EECC is confined to the EAC (primarily the bony canal) and does not arise from the middle ear cleft or tympanic membrane retraction pockets. (Scott-Brown's Otorhinolaryngology, 8th Ed.)
2. HISTORICAL BACKGROUND
| Year | Contribution |
|---|
| 1850 | Toynbee — First described accumulation of keratin in EAC |
| 1965 | Piepergerdes & Kramer — Defined EECC as a distinct entity |
| 1980 | Holt — Classified EECC into primary and secondary types |
| 1992 | Naim — Expanded staging based on CT and operative findings |
| 2016 | Heilbrun et al. — Radiological staging and CT criteria defined |
3. ANATOMY RELEVANT TO EECC
(Bailey and Love's, p. 771)
External Auditory Canal: Total Length = ~3 cm
├── Outer 1/3 (Cartilaginous) — 8 mm
│ ├── Skin: thick, with hair follicles, ceruminous glands
│ └── Normal epithelial migration: CENTRIFUGALLY outward
└── Inner 2/3 (Bony) — 16 mm
├── Skin: thin, tightly adherent to periosteum, NO appendages
├── Normal migration: along floor → tympanic membrane → annulus → EAC wall
└── Vulnerable zone: posteroinferior bony canal floor
Epithelial Migration Theory (Alberti, 1964):
- Normal skin migrates centrifugally from the umbo outward at 0.07 mm/day
- Any disruption of this migration leads to keratin accumulation → EECC
4. EPIDEMIOLOGY
- Incidence: ~1 in 1000 ENT outpatient consultations (Naim, 2005)
- Age: Most common in 5th–6th decade
- Sex: Slight male predominance
- Laterality: Usually unilateral; bilateral in <5%
- Association: Prior ear surgery, radiotherapy, chronic otitis externa
5. ETIOLOGY AND PATHOGENESIS
5.1 Classification by Etiology
EECC
├── A. PRIMARY (Idiopathic / Spontaneous)
│ ├── No identifiable cause
│ ├── Failure of normal epithelial migration
│ └── Most common — ~90%
│
└── B. SECONDARY (Acquired / Iatrogenic)
├── Post-traumatic (temporal bone fracture, instrumentation)
├── Iatrogenic (post-tympanoplasty, mastoidectomy, myringoplasty)
├── Obstructive (osteoma, exostosis, EAC stenosis)
├── Post-radiotherapy
└── Inflammatory (chronic otitis externa)
5.2 Pathogenesis Theories
① Epithelial Migration Failure (Most Accepted)
- Proposed by Alberti and confirmed by Scott-Brown (Scott-Brown, 8th Ed., Vol. 3)
- Normal centrifugal migration arrests → keratin accumulates → pressure necrosis of bony canal → periostitis → bone erosion
② Periostitis Theory (Holt, 1992)
- Primary periostitis (following minor trauma/infection) → overlying epithelium loses its migratory ability → secondary keratin entrapment
③ Microtrauma Theory (Cummings Otolaryngology, 7th Ed.):
- Repeated microtrauma to canal skin → epithelial implantation → sac formation → keratin accumulation
④ Chronic Obstruction Theory:
- Osteoma / exostosis causes cerumen/epithelial debris impaction → migration arrest → cholesteatoma
6. PATHOLOGY
Macroscopic:
- White, pearly, waxy mass of laminated keratin
- Located on bony floor/posterior wall of EAC
- Surrounded by granulation tissue
- Underlying bone shows erosion and sclerosis
Microscopic (Dhingra Diseases of Ear Nose and Throat, 7th Ed.):
Histology of EECC
├── Keratinizing stratified squamous epithelium (lining)
├── Laminated keratin debris (core / matrix)
├── Granulation tissue (perimatrix)
├── Chronic inflammatory infiltrate
├── Osteoclastic bone resorption (enzymes: collagenase, IL-1, PGE₂)
└── Periosteum: thickened, inflamed
Bone-Eroding Enzymes:
- Collagenase from keratinocytes
- Prostaglandin E₂ (inflammatory mediator)
- Interleukin-1 (stimulates osteoclasts)
- Cathepsin D, matrix metalloproteinases (MMPs) (Recent advances - Dornhoffer, 2019)
7. CLINICAL FEATURES
Symptoms (Stell and Maran's Textbook of Head and Neck Surgery):
| Symptom | Frequency | Notes |
|---|
| Unilateral hearing loss (conductive) | ~75% | From canal occlusion |
| Ear fullness / blockage | ~80% | Keratin mass effect |
| Otorrhoea (non-purulent, white/pearly) | ~60% | Exfoliated keratin |
| Otalgia | ~50% | Periostitis / exposed bone |
| Tinnitus | ~30% | Canal occlusion |
| Facial nerve palsy | Rare | Severe bone erosion |
| Vertigo | Rare | Labyrinthine involvement |
Signs on Otoscopy:
- White/pearly keratinous mass in EAC (posteroinferior bony canal)
- Erosion of bony canal floor/posterior wall
- Blunting of anterior recess
- Granulation tissue at edges
- Exposed/necrotic bone (hallmark of advanced disease)
- Tympanic membrane: Usually intact (distinguishes from middle ear cholesteatoma)
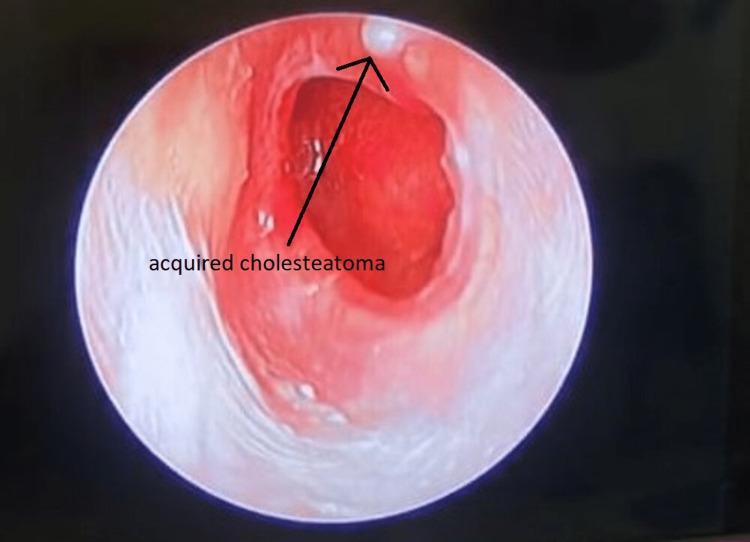
8. CLINICAL PHOTOGRAPH
Otoscopic image demonstrating EECC: white keratinous debris (arrowed) at the superior canal, surrounding erythema, granulation tissue, and compromised canal wall integrity.
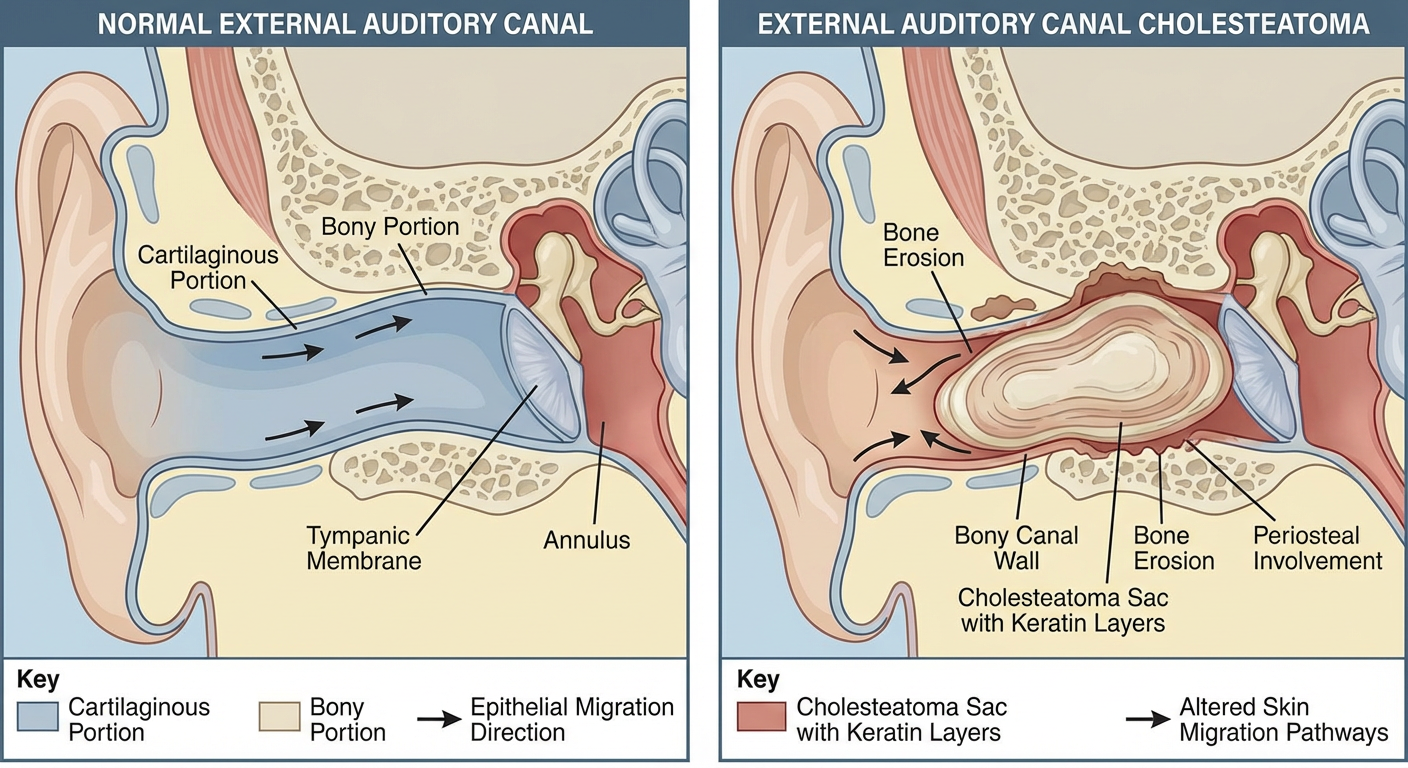
9. ANATOMICAL DIAGRAM
Cross-sectional anatomy of EECC: Keratinous debris accumulation, periosteal involvement, bone erosion of inferior/posterior bony canal wall, and disrupted centrifugal epithelial migration.
10. STAGING / CLASSIFICATION
Naim Classification (2005) — Most Widely Used
┌─────────────────────────────────────────────────────────────────────┐
│ NAIM STAGING SYSTEM (2005) │
├───────┬─────────────────────────────────────────────────────────────┤
│ Stage │ Description │
├───────┼─────────────────────────────────────────────────────────────┤
│ I │ Keratinous debris + hyperemic/damaged skin ONLY (no bone │
│ │ erosion) │
├───────┼─────────────────────────────────────────────────────────────┤
│ II │ Periostitis + early periosteal erosion (no frank bone loss) │
├───────┼─────────────────────────────────────────────────────────────┤
│ III │ Bone erosion + involvement of bony canal walls │
│ │ (posterior, inferior, anterior, superior) │
├───────┼─────────────────────────────────────────────────────────────┤
│ IV │ Extension into adjacent structures: │
│ │ TMJ, mastoid, facial nerve, middle ear, parotid, skull base│
└───────┴─────────────────────────────────────────────────────────────┘
Holt Classification (1992):
- Type 1: Primary — No identifiable cause; keratinous occlusion
- Type 2: Secondary — Post-trauma or post-surgical
- Type 3: Secondary — Associated with obstructive lesions (exostosis, osteoma)
- Type 4: Secondary — Post-inflammatory
Heilbrun CT-Based Staging (2016) (Recent Advance):
- Grade A: Keratin plug without bone erosion
- Grade B: Bone erosion confined to EAC floor
- Grade C: Erosion of EAC floor and walls, mastoid/middle ear involvement
11. DIFFERENTIAL DIAGNOSIS
| Condition | Differentiating Features |
|---|
| Chronic Otitis Externa | Diffuse, no bone erosion, responds to topical Rx |
| Middle Ear Cholesteatoma | Arises from TM/pars flaccida, TM perforation/retraction |
| Keratosis Obturans | Bilateral, young patients, diffuse expansion (not erosion), painful |
| Osteoma / Exostosis | Bony hard, no keratin, CT: calcified |
| Squamous Cell Carcinoma | Irregular, bleeds easily, biopsy differentiates |
| Necrotizing (Malignant) Otitis Externa | Elderly, diabetic, Pseudomonas, granulation at BJ, systemic toxicity |
| EAC Papilloma | Papillary growth, HPV-associated |
EECC vs Keratosis Obturans — Key Distinction (Cummings, 7th Ed.):
| Feature | EECC | Keratosis Obturans |
|---|
| Age | 5th-6th decade | Young adults |
| Laterality | Usually unilateral | Bilateral |
| Canal involvement | Focal erosion, floor/posterior wall | Diffuse widening, no focal erosion |
| Pain | Mild/absent | Severe |
| Pathology | Sac with keratin, bone erosion | Keratin plug, expanded canal |
| Associated | Sinus disease, bronchiectasis | Often associated |
| Treatment | Surgery | Conservative |
12. INVESTIGATIONS
A. Audiological:
- Pure Tone Audiogram (PTA): Conductive hearing loss (CHL)
- Tympanometry: Type A (canal obstruction), Type B if middle ear involved
B. Radiology (Zakir Hussain's ENT, Hazarika ENT):
High-Resolution CT (HRCT) Temporal Bone — Investigation of Choice
HRCT Findings in EECC:
├── Soft tissue density mass in bony EAC
├── Erosion of bony EAC (posteroinferior > floor > posterior wall)
├── Expansion/blunting of EAC contour
├── Intact tympanic membrane (usually)
├── ± Middle ear/mastoid involvement (advanced)
├── ± TMJ involvement
├── ± Facial nerve canal erosion
└── ± Tegmen/lateral skull base erosion
MRI Temporal Bone:
- T1: Hypointense mass
- T2: Hyperintense (keratin)
- DWI: Restricted diffusion (high signal) — Pathognomonic for cholesteatoma (Recent advance — MRI DWI)
- Useful for detecting residual/recurrent disease post-operatively
C. Laboratory:
- Not diagnostic; useful pre-operatively (CBC, coagulation)
- Culture and sensitivity if infected
D. Biopsy:
- Only if malignancy suspected (SCC must be excluded)
13. MANAGEMENT
FLOWCHART: Management Algorithm for EECC
SUSPECTED EECC
│
┌──────────▼──────────┐
│ History + Clinical │
│ Examination │
└──────────┬──────────┘
│
┌──────────▼──────────┐
│ HRCT Temporal Bone │
│ ± MRI DWI │
└──────────┬──────────┘
│
┌──────────▼──────────┐
│ Naim Staging │
└──────┬──────────────┘
│
┌──────────┴──────────────┐
│ │
┌─────▼──────┐ ┌───────▼────────┐
│ Stage I │ │ Stage II-IV │
└─────┬──────┘ └───────┬────────┘
│ │
┌───────▼────────┐ ┌────────▼───────────────┐
│ CONSERVATIVE │ │ SURGICAL │
│ • Microsuction│ │ (Canalplasty / │
│ • Topical │ │ Canal Wall Surgery) │
│ antibiotics │ └────────┬───────────────┘
│ • Serial FU │ │
└───────┬────────┘ ┌───────────┼────────────────┐
│ │ │ │
┌─────▼──────┐ ┌───▼────┐ ┌──▼──────┐ ┌──────▼─────┐
│ Resolution │ │Stage II│ │Stage III│ │ Stage IV │
└────────────┘ │Canalpl.│ │Canalpl. │ │ Canalplasty│
│+ clean │ │+ mastoid│ │+ mastoidect│
└────────┘ └─────────┘ │+ facial N │
│ decompres.│
└────────────┘
│
┌───────────▼──────────┐
│ POSTOPERATIVE FU │
│ • Canal packing │
│ • Monthly for 3/12 │
│ • MRI DWI at 1 year │
│ • HRCT if suspect │
└──────────────────────┘
13.1 Conservative Management (Stage I)
(Dhingra ENT, 7th Ed.; Hazarika ENT)
Indications: Stage I disease, elderly/unfit patients, patient refusal for surgery
- Microsuction / Aural toilet under microscope (regular debridement)
- Topical antibiotics (ciprofloxacin drops) for secondary infection
- Topical steroids (betamethasone) for canal inflammation
- Acidifying agents (acetic acid 2% in aluminium acetate) — anti-infective
- Serial HRCT monitoring every 6–12 months
- Caveat: Does not address underlying pathology; disease may progress
13.2 Surgical Management (Scott-Brown, 8th Ed.; Cummings, 7th Ed.; Stell and Maran)
Surgical Goals:
- Complete removal of cholesteatoma matrix and keratin
- Restoration of EAC anatomy
- Elimination of bone-eroded recesses
- Prevention of recurrence
- Preservation of hearing
Surgical Approaches:
① Canalplasty (Meatocanalplasty) — Most common procedure
CANALPLASTY — Steps:
1. Infiltration with 1:200,000 adrenaline
2. Post-auricular or endaural incision
3. Elevation of EAC skin flap
4. Complete removal of cholesteatoma + matrix
5. Drilling of bony EAC to widen and saucerize
6. Curettage of infected bone/granulation tissue
7. EAC skin graft (temporalis fascia / STSG)
8. Canal packing (Bismuth iodoform paraffin paste)
9. Repair of TM if involved
② Extended Canalplasty: For Stage III disease with significant bone erosion
③ Canalplasty + Cortical Mastoidectomy: When mastoid air cells are involved (Stage III/IV)
④ Canalplasty + Facial Nerve Decompression: Stage IV with facial nerve involvement
⑤ Subtotal Petrosectomy: Rare; skull base involvement (Stage IV advanced)
13.3 Surgical Approaches Summary Table
| Stage | Procedure | Approach |
|---|
| I | Conservative / limited excision | Transcanal |
| II | Canalplasty | Post-auricular or endaural |
| III | Extended canalplasty ± mastoidectomy | Post-auricular |
| IV | Canalplasty + mastoidectomy ± facial nerve decompression ± skull base surgery | Post-auricular / Infratemporal |
14. COMPLICATIONS
A. Disease Complications (If Untreated):
Local Spread
├── Tympanic membrane perforation
├── Middle ear involvement (ossicular chain erosion → CHL)
├── Mastoid extension
├── Facial nerve canal erosion → Facial palsy
├── Labyrinthine fistula → Sensorineural HL / Vertigo
├── Tegmen erosion → Intracranial extension
│ ├── Extradural abscess
│ ├── Meningitis
│ └── Brain abscess
└── Jugular bulb / Sigmoid sinus erosion → Sinus thrombosis
B. Surgical Complications:
| Complication | Cause | Management |
|---|
| Recurrence | Incomplete matrix removal | Revision surgery, MRI DWI |
| EAC stenosis | Over-aggressive drilling, inadequate skin cover | Revision canalplasty |
| Facial nerve injury | Dehiscent nerve, excessive drilling | Intraop monitoring, decompression |
| Sensorineural HL | Labyrinthine involvement | Preoperative counselling |
| TM perforation | Intraoperative | Myringoplasty |
| Keloid / hypertrophic scar | Post-auricular incision | Steroid injection, revision |
15. PROGNOSIS AND RECURRENCE
- Cure rate after canalplasty: ~85–90% for Stage I/II (Naim, 2005)
- Recurrence rate:
- Stage I–II: <10%
- Stage III–IV: 15–25%
- Recurrence risk factors: Incomplete removal, narrow canal, canal stenosis, immunosuppression
- Surveillance: MRI DWI at 1 year post-operatively is now preferred over second-look surgery (Recent advance)
16. RECENT ADVANCES
A. Diagnostic Advances:
1. Non-Echo Planar DWI MRI (non-EP DWI)
- Detects cholesteatoma as small as 2 mm
- Sensitivity: 94%, Specificity: 97% (Muzaffar et al., Laryngoscope, 2017)
- Now replaces second-look surgery in many centres
- Detects residual/recurrent EECC without radiation
2. Cone Beam CT (CBCT)
- Lower radiation dose than HRCT
- High spatial resolution for ossicular chain and canal bone
- Increasingly used for follow-up (Viccaro et al., 2015)
3. Endoscopic Ear Surgery (EES) for diagnosis
- 0° and 30° rigid endoscopes provide panoramic canal views
- Identifies hidden recesses missed on otoscopy
B. Molecular/Biological Advances:
4. Biomarkers of Bone Erosion:
- MMP-2, MMP-9 (matrix metalloproteinases) elevated in EECC tissue
- RANKL/OPG ratio — Marker of osteoclast activity
- IL-1β, TNF-α — Cytokine profiling of EECC matrix (Yung & Tassone, 2017)
- Future therapeutic targets: anti-RANKL biologics, MMP inhibitors
5. Keratinocyte Biology:
- Aberrant expression of involucrin, cytokeratins (CK16, CK17) in EECC
- Suggests a specific molecular phenotype distinct from normal EAC keratinocytes
C. Surgical Advances:
6. Fully Endoscopic Canalplasty:
- Transcanal endoscopic approach (TECA)
- No post-auricular incision, better visualization of bony canal angles
- Shorter hospital stay (Presutti, Marchioni et al., 2021)
7. Powered Microdebrider:
- Precise tissue removal with simultaneous suction
- Reduces risk of inadvertent injury
8. Intraoperative Facial Nerve Monitoring:
- Continuous EMG monitoring during Stage III/IV surgery
- Reduces facial nerve injury
9. Laser-Assisted Canalplasty:
- CO₂ laser or KTP laser for controlled bone ablation
- Reduces bleeding, precise tissue removal (Limited studies)
10. Bioabsorbable Canal Dressings:
- Hyaluronate-based sponges promote epithelialization
- Replace BIPP packing with faster healing (Heal-All, Nasopore)
17. KEY POINTS FROM STANDARD TEXTBOOKS
| Textbook | Key Teaching on EECC |
|---|
| Scott-Brown's Otorhinolaryngology (8th Ed.) | Epithelial migration failure as central pathogenesis; canalplasty as gold standard treatment |
| Cummings Otolaryngology (7th Ed.) | Keratosis obturans vs EECC distinction; HRCT staging; extended canalplasty technique |
| Stell & Maran's Head and Neck Surgery | Clinical staging, management algorithm, complications |
| Zakir Hussain ENT | Classification, HRCT role, conservative vs surgical indications |
| Dhingra Diseases of ENT (7th Ed.) | Histopathology, clinical features, differential diagnosis |
| Hazarika ENT | Indian context, periostitis theory, surgical steps of canalplasty |
| Bailey and Love's (28th Ed., p. 771) | Anatomy of EAC, epithelial migration basis of cholesteatoma |
18. SUMMARY FLOWCHART: EECC — Pathogenesis to Management
PREDISPOSING FACTORS
(Trauma / Surgery / Obstruction / Idiopathic)
│
▼
DISRUPTION OF NORMAL EPITHELIAL MIGRATION
(Centrifugal migration → Arrested migration)
│
▼
KERATIN ACCUMULATION IN BONY EAC
(Posteroinferior canal → accumulation → sac formation)
│
▼
PERIOSTITIS + INFLAMMATORY CYTOKINES
(IL-1β, TNF-α, MMP-2, MMP-9, PGE₂, RANKL)
│
▼
OSTEOCLAST ACTIVATION → BONE EROSION
(EAC floor → posterior wall → mastoid → skull base)
│
▼
CLINICAL PRESENTATION
(Unilateral CHL, otorrhoea, otalgia, exposed bone)
│
▼
INVESTIGATION
(HRCT Temporal Bone → Naim Staging; MRI DWI)
│
┌────┴────┐
▼ ▼
Stage I Stage II-IV
│ │
Conservative Surgery
(microsuction) (Canalplasty ± mastoidectomy)
│ │
└────┬────┘
▼
POSTOPERATIVE SURVEILLANCE
(MRI DWI @ 1 year → R/O recurrence)
19. MNEMONICS
Causes of EECC — "STOIC"
- S — Surgery (post-operative)
- T — Trauma (temporal bone fracture)
- O — Obstruction (osteoma, exostosis)
- I — Idiopathic (primary/spontaneous)
- C — Chronic inflammation (otitis externa)
Naim Stages — "SPBE"
- S — Skin only (Stage I)
- P — Periostitis (Stage II)
- B — Bone erosion of EAC (Stage III)
- E — Extension to adjacent structures (Stage IV)
20. EXAM-ORIENTED HIGH-YIELD POINTS
- EECC is NOT a true neoplasm — it is a dyskeratotic process with keratinizing squamous epithelium
- Primary EECC has no identifiable cause; failure of epithelial migration is the cornerstone mechanism
- Posteroinferior bony canal is the most common site of involvement
- EECC vs Keratosis Obturans — most commonly asked distinction (bilateral vs unilateral; expansion vs erosion; young vs old; painful vs painless)
- HRCT temporal bone is the investigation of choice for staging
- MRI DWI (non-echo planar) is the gold standard for detection of residual/recurrent disease
- Canalplasty is the mainstay of surgical treatment
- Stage IV may require facial nerve decompression and skull base surgery
- Bone-eroding enzymes: collagenase, MMP-2, MMP-9, IL-1β, PGE₂
- Recurrence rate is 10–25%; lifelong surveillance required
REFERENCES
- Scott-Brown's Otorhinolaryngology: Head and Neck Surgery, 8th Edition
- Cummings Otolaryngology: Head and Neck Surgery, 7th Edition
- Stell and Maran's Head and Neck Surgery and Oncology, 5th Edition
- Dhingra P.L.: Diseases of Ear, Nose and Throat, 7th Edition
- Hazarika P.: Textbook of ENT and Head-Neck Surgery
- Zakir Hussain: Clinical ENT
- Bailey and Love's Short Practice of Surgery, 28th Edition (p. 771)
- Naim R. et al. — Classification and staging of EECC. Eur Arch Otorhinolaryngol, 2005
- Holt JJ — Ear Canal Cholesteatoma. Laryngoscope, 1992
- Heilbrun ME et al. — CT staging of EECC. AJNR, 2016
- Muzaffar J. et al. — MRI DWI for cholesteatoma detection. Laryngoscope, 2017
- Presutti L., Marchioni D. — Endoscopic Ear Surgery. Thieme, 2021
- Yung MW & Tassone P. — Bone erosion mediators in cholesteatoma. Clin Otolaryngol, 2017
This answer covers Definition, Epidemiology, Anatomy, Etiology, Pathogenesis (all theories), Pathology, Classification (Naim, Holt, Heilbrun), Clinical Features, Differential Diagnosis, Investigations, Management (conservative + surgical with flowcharts), Complications, Prognosis, Recent Advances, and High-yield exam points — comprehensively addressing a 50-mark question.