Endoscopic resection for early gastric carcinoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"early gastric cancer" AND "endoscopic submucosal dissection"
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Endoscopic Resection for Early Gastric Carcinoma (EGC)
Early gastric cancer (EGC) is defined as adenocarcinoma confined to the mucosa or submucosa, regardless of lymph node status. Endoscopic resection offers curative-intent treatment while preserving the stomach - its major advantage over gastrectomy.
Modalities
Two primary techniques are used:
1. Endoscopic Mucosal Resection (EMR)
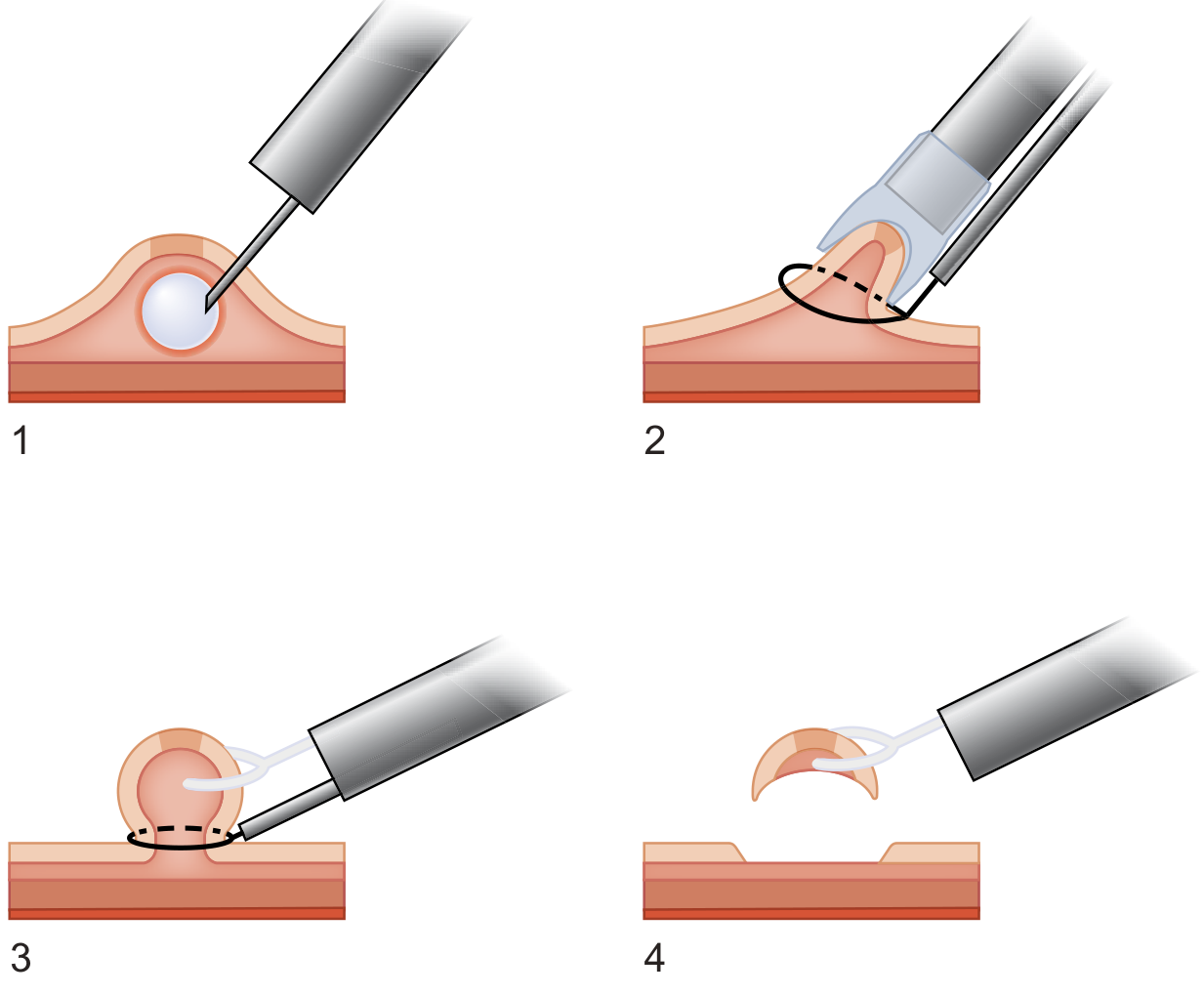
Figure: EMR by strip biopsy. (1) Saline injected into submucosa to elevate the lesion; (2) the mound is grasped with forceps and the snare placed at its base; (3) snare positioned; (4) electrosurgical current applied and the mucosal lesion is removed. - Sabiston Textbook of Surgery
- Technique: Saline injection into the submucosal layer lifts the lesion, which is then encircled with a snare or suction cap and excised with electrocautery.
- Methods: Cap-assisted (lesion sucked into transparent cap then snared), ligation-assisted (band creates pseudopolyp then excised), or injection-assisted.
- Perforation rate: Low; bleeding ~15% (usually controllable endoscopically).
- Key limitation: Piecemeal resection is common for larger lesions, which raises recurrence risk. En bloc resection is preferred.
2. Endoscopic Submucosal Dissection (ESD)
- Technique: Electrocautery marks the lesion borders; epinephrine + indigo carmine is injected submucosally to hydrodissect; an insulation-tipped (IT) knife dissects a submucosal plane deep to the tumor for complete en bloc removal; bleeding controlled with electrocautery throughout.
- Key advantage: Enables en bloc resection of larger tumors and those with limited submucosal invasion, regardless of tumor size, location, or ulceration status.
- En bloc resection rate: 92.7-98.0% across large series; a meta-analysis confirms ESD superior to EMR for en bloc rates.
- More technically demanding than EMR, with a higher risk of perforation.
- Predominantly performed in East Asian centers; adoption in Western centers remains limited due to the steep learning curve.
Indications
Standard (Absolute) Criteria
(Box 87.2, Sabiston Textbook of Surgery)
| Criterion | Requirement |
|---|---|
| Histological type | Intestinal-type (differentiated) adenocarcinoma |
| Depth | Confined to mucosa (Tis or T1a) |
| Lymphovascular invasion | Absent |
| Ulceration | None |
| Size | < 2 cm |
Risk of lymph node metastasis in patients meeting standard criteria: approximately 0.2%.
Expanded (Extended) Criteria
(Japanese guidelines / Clinical Gastrointestinal Endoscopy)
ESD allows curative resection for "extended indications" if the lesion is resected en bloc with negative margins, no lymphovascular invasion, and meets any one of the following:
- > 2 cm, differentiated type, intramucosal, without ulceration
- ≤ 3 cm, differentiated type, intramucosal, with ulceration (UL+)
- ≤ 2 cm, undifferentiated type, intramucosal, without ulceration
- ≤ 3 cm, differentiated type, SM1 invasion (< 500 µm into submucosa)
Risk of lymph node metastasis at expanded criteria: ~0.7% (vs 0.2% for standard criteria). Expanded criteria are not widely adopted in Western centers.
The JCOG 0607 trial validated ESD for expanded indications (excluding undifferentiated type): 5-year OS was 97.0% (95% CI: 95.0-98.2%), exceeding the pre-specified threshold, establishing ESD as a standard treatment for EGC within expanded indications.
Pre-procedural Assessment
- Endoscopic ultrasound (EUS): Critical for T staging - the first/second hypoechoic layers = mucosa; third hyperechoic = submucosa; fourth hypoechoic = muscularis propria. EUS distinguishes T1a (mucosal) from T1b (submucosal) disease.
- Magnifying NBI: The MESDA-G algorithm (Magnifying Endoscopy Simple Diagnostic Algorithm for EGC) guides optical diagnosis.
- Paris classification: Classifies superficial lesion morphology (0-I polypoid; 0-IIa/b/c flat; 0-III excavated).
- CT staging: To exclude lymph node involvement and distant metastasis before planning endoscopic vs surgical approach.
Post-resection Pathological Assessment and Decision-Making
After resection, the specimen is assessed for:
- Completeness: Lateral and vertical margins
- Depth of invasion: Mucosal (M) vs. submucosal (SM1 < 500 µm; SM2 ≥ 500 µm)
- Histological type: Differentiated vs. undifferentiated
- Lymphovascular invasion: ly(+) or ly(-)
- Ulceration: Present or absent
Management by Resection Result
| Scenario | Action |
|---|---|
| En bloc, negative margins, no LVI, meets standard/expanded criteria | Curative - surveillance only |
| Positive lateral margins | Repeat endoscopic therapy or close surveillance |
| Positive vertical margins, LVI, or SM2+ invasion | Refer for gastrectomy + lymphadenectomy |
Outcomes vs. Surgery
Meta-analyses show endoscopic resection is associated with:
- Higher rates of incomplete resection and local recurrence compared with conventional surgery
- No significant difference in 5-year overall survival when selection criteria are appropriately applied
- (Sabiston Textbook of Surgery)
A 2025 systematic review comparing ESD vs. EMR (Zheng & Xu, Front Med, PMID 41393136) reconfirms ESD superiority for en bloc and R0 resection rates.
Complications
| Complication | EMR | ESD |
|---|---|---|
| Bleeding | ~15% | ~5-7% (delayed bleeding a known risk) |
| Perforation | Low (< 1%) | Higher than EMR (1-5%) |
| Stricture | Rare in stomach | Rare in stomach |
A 2026 meta-analysis (Chen et al., PMID 41896436) identified risk prediction models for delayed bleeding after gastric ESD, noting anticoagulant use, lesion size, and specimen size as key predictors.
Complications including perforation and post-ESD bleeding are generally manageable endoscopically (clips, coagulation), avoiding the need for surgery in most cases.
Technical Innovations (2025-2026)
- Traction-assisted ESD: A 2026 meta-analysis (Zhang et al., Surg Endosc, PMID 41731140) confirms traction devices improve ESD efficacy and safety (faster dissection, reduced perforation).
- Pocket-creation method (PCM): A 2025 meta-analysis (Song et al., Saudi Med J, PMID 40335108) found PCM reduces procedure time and improves en bloc resection rates vs. conventional ESD.
Summary
| Feature | EMR | ESD |
|---|---|---|
| Best for | Lesions < 2 cm, no ulcer | Larger, ulcerated, or SM1 lesions |
| En bloc rate | Lower | 92-98% |
| Recurrence | Higher (piecemeal risk) | Lower |
| Complexity | Lower | Higher (steep learning curve) |
| Perforation risk | Lower | Higher |
| West adoption | Moderate | Limited |
Key principle: Any resection with positive vertical margins, lymphovascular invasion, or SM2 submucosal invasion should prompt referral for gastrectomy with lymphadenectomy, as these features correlate with meaningful lymph node metastasis risk that exceeds the safety threshold for endoscopic cure.
Sources: Sabiston Textbook of Surgery (p. 1803-1805); Clinical Gastrointestinal Endoscopy, Expert Consult 3e (pp. 487-492); Current Surgical Therapy 14e (p. 69); recent systematic reviews PMID 41393136, 41731140, 40335108, 41896436.
Describe the management of a 4 cm perforation of the first part of the duodenum. [10]
Reading File
Finding Sources
Finding Sources
Searching PubMed
"duodenal perforation" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the material needed. Here is the comprehensive answer:
Management of a 4 cm Perforation of the First Part of the Duodenum (D1)
A 4 cm perforation of D1 is a large ulcer perforation (>2 cm), which places it in a category demanding special surgical consideration beyond simple Graham patching. The size means primary suture closure alone risks breakdown, and omental patching of the raw hole may be insecure. This is a surgical emergency.
1. Immediate Resuscitation (Pre-operative)
- IV access, aggressive fluid resuscitation (crystalloids) to correct hypovolaemia and sepsis.
- Broad-spectrum IV antibiotics (e.g. co-amoxiclav or cephalosporin + metronidazole) promptly; add antifungal cover only in frail, immunosuppressed, or previously hospitalised patients.
- Nasogastric (NG) tube: stomach decompression, reduces further peritoneal soilage.
- Urinary catheter for monitoring urine output.
- Blood tests: FBC, U&E, LFTs, amylase, coagulation, crossmatch, ABG.
- IV proton pump inhibitor (PPI) infusion.
- CT abdomen (with IV contrast): confirms pneumoperitoneum, extent of peritoneal soilage, and any associated pathology. Most sensitive for diagnosing perforation and retroperitoneal involvement.
- Optimise but do not delay surgery unduly - resuscitation and surgical treatment must proceed in parallel.
2. Decision: Operative vs Non-operative
Non-operative management is reserved only for the rare stable patient with a radiologically confirmed sealed perforation and no peritonitis. A 4 cm free perforation with peritoneal soilage virtually always requires surgery.
3. Operative Approach
Access
Laparotomy (midline) is standard. Laparoscopic repair has been validated for perforated PUD and can be considered if the surgeon has the requisite skill and the patient is haemodynamically stable - it is not absolutely contraindicated but is technically demanding for large defects. The only absolute contraindications to minimally invasive surgery are major haemodynamic instability and lack of local laparoscopic skill.
Initial Steps
- Peritoneal washout with 5-10 litres of warm saline; send peritoneal fluid for culture and sensitivity including fungal studies.
- Biopsy the ulcer edge only if there is any suspicion of malignancy (routine biopsy is not necessary).
- Assess: size, exact location in D1, tissue quality, proximity to pylorus and ampulla, degree of local inflammation.
- A Kocher manoeuvre (mobilising the duodenum off the retroperitoneum) facilitates exposure and tension-free repair.
4. Repair Options for the Large (4 cm) Perforation
Standard Graham patching without primary closure is insufficient for a 4 cm defect. Options, in order of application:
A. Primary Closure + Omental Buttress (Patch)
- If tissue quality permits, close the defect with interrupted or running slowly absorbable sutures (one or two layers) without significantly narrowing the duodenal lumen. Up to 50% luminal narrowing is generally acceptable. For longitudinal lacerations, close transversely (Heineke-Mikulicz principle) to avoid stricture.
- Cover/buttress the primary closure with a well-vascularised omental flap, circumferentially sutured around the repair site with multiple interrupted sutures. Ensure the inferior end is well anchored to prevent tension on the patch.
- If no viable omentum, the falciform ligament (divided close to the abdominal wall and mobilised to the liver) is an alternative.
- Test repair integrity by injecting air/methylene blue through the NG tube while the site is submerged under irrigation fluid.
B. Omental Plug Technique (Modified Graham)
- If primary closure will cause unacceptable narrowing or the tissue is too friable to hold sutures, place double-armed sutures "inside out" through the duodenal wall surrounding the perforation, and pull a tongue of well-vascularised omentum directly into the defect as a plug. Tie sutures snugly to secure, without causing ischaemia.
C. Jejunal Serosal Patch (Thal Patch)
- A loop of healthy proximal jejunum is brought up (antecolic or retrocolic) adjacent to the perforation and sutured to the perforation margins with full-thickness bites to seromuscular bites of the jejunum.
- Better suited for defects not amenable to omental repair; however, carries a significant failure rate for very large defects or severe local inflammation.
D. Roux-en-Y Duodenojejunostomy
- For large, chronic perforations in a stable, low-risk patient, the debrided duodenal opening is anastomosed to a Roux limb in a tension-free two-layer side-to-side handsewn anastomosis. This provides durable closure and wide duodenal decompression.
5. The Triple-Tube Technique (High-Risk Adjunct)
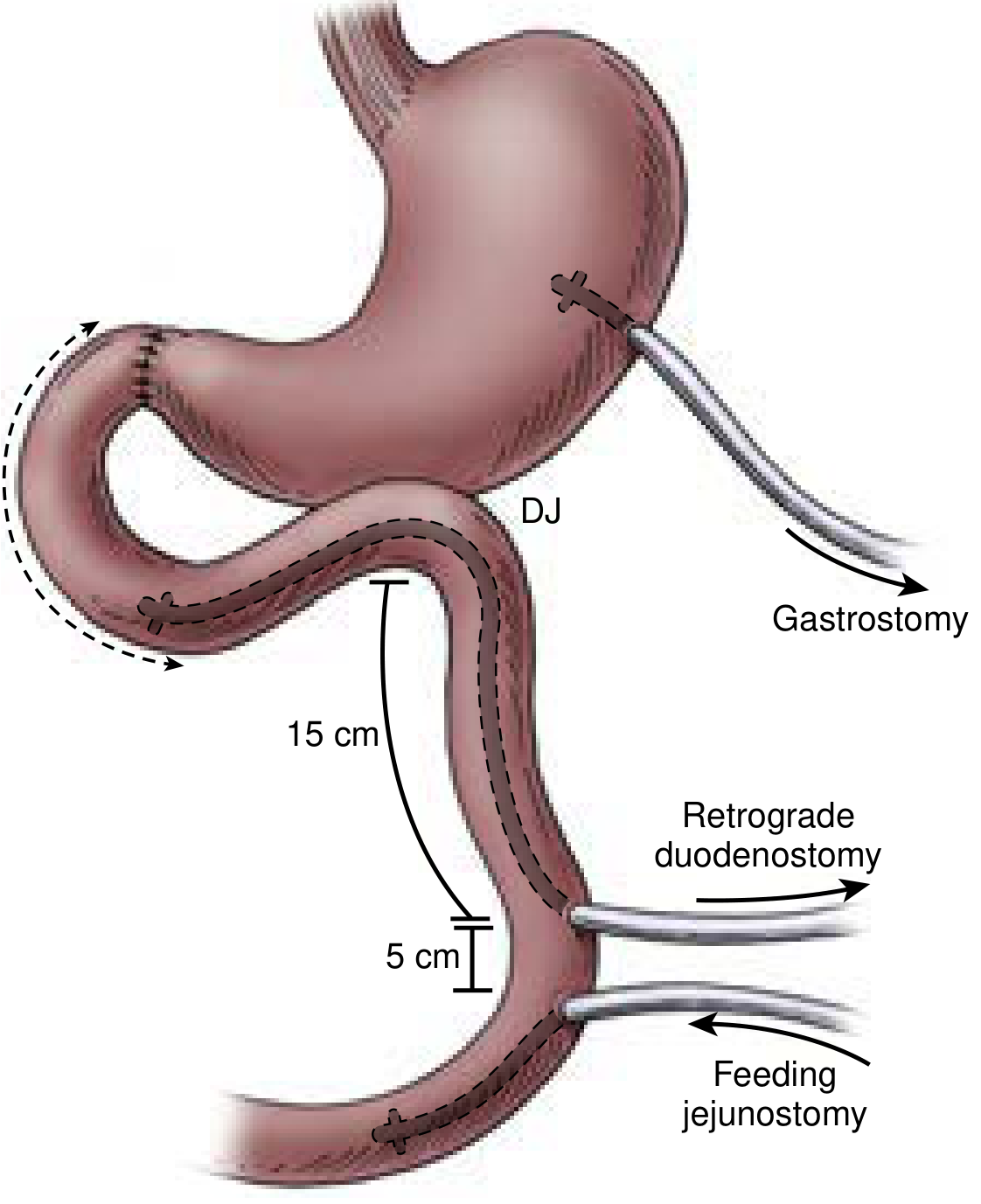
Figure: Triple tube technique - gastrostomy (gastric decompression), retrograde duodenostomy (duodenal decompression via jejunum), and feeding jejunostomy (enteral nutrition). - Current Surgical Therapy 14e
This technique is strongly recommended as an adjunct in all high-risk, large perforations. It consists of:
- Gastrostomy tube - decompresses the stomach and reduces acid/content load on the repair.
- Retrograde duodenostomy tube - a jejunostomy tube passed retrogradely through the jejunum into the duodenum, providing controlled duodenal decompression and a controlled fistula if the repair leaks.
- Antegrade feeding jejunostomy - enables early enteral nutrition.
This avoids the morbidity of lateral duodenostomy or transpyloric intubation and is quick to perform. Leakage from a large D1 repair is not uncommon, and having a controlled fistula via the retrograde tube is far safer than an uncontrolled duodenal fistula.
6. Pyloric Exclusion
For the most tenuous closures, pyloric exclusion is considered:
- The pylorus is closed with a heavy absorbable suture (which will recanalize in 3-6 weeks), diverting gastric contents away from the repair.
- A dependent loop gastrojejunostomy is fashioned to restore gastric outflow.
- This protects the repair by reducing luminal pressure and acid exposure during healing.
7. Definitive Ulcer Surgery
Consider in stable, low-risk patients (ASA 1 or 2) where the perforation is large (>2 cm) or the patient has a documented history of peptic ulcer disease, and provided peritonitis is not severe/exudative. Options:
- Truncal vagotomy + gastrojejunostomy (with or without temporary pyloric closure) after repair.
- Truncal vagotomy + antrectomy (Billroth II): Only if the perforated duodenum can be safely resected with the antrum and a secure duodenal stump created. If ampullar involvement is a risk, protect with a biliary Fogarty catheter passed via the cystic duct. Never attempt resection if a tenuous duodenal stump or ampullary injury is likely.
In the era of PPIs and H. pylori eradication, most surgeons limit themselves to repair + washout, reserving definitive acid-reduction surgery for a small minority of patients.
8. Drains and Closure
- Place at least one (preferably two) closed-suction peritoneal drains near the repair site - repair site leakage is not uncommon with large perforations.
- NG tube remains in situ postoperatively for decompression and for contrast studies if leak is suspected.
- Abdominal closure per standard technique.
9. Post-operative Management
- IV PPI (high-dose) continued until oral intake established; then switch to oral PPI.
- Continue IV antibiotics per culture sensitivity results.
- H. pylori testing (CLO test on intraoperative biopsy or serology) and eradication therapy on resuming oral intake - most important step in preventing recurrence.
- NG tube removed once bowel function returns; enteral nutrition via jejunostomy tube if triple-tube technique used.
- Contrast study through NG tube or water-soluble swallow at 5-7 days to confirm repair integrity before oral diet.
- DVT prophylaxis; early mobilisation.
- Drain output monitored - if bile/intestinal fluid suggests fistula, the controlled retrograde duodenostomy tube provides a safe conduit.
Summary Table
| Feature | Consideration |
|---|---|
| Size | 4 cm = large perforation; standard Graham patch insufficient alone |
| Location | D1 (first part) - away from ampulla, Kocher manoeuvre aids exposure |
| Priority repair | Primary closure + omental buttress OR omental plug |
| Adjunct (high-risk) | Triple-tube technique (gastrostomy + retrograde duodenostomy + jejunostomy) |
| Unstable/damage control | Suture/staple closure + multiple drains; return for definitive repair |
| Diversion (tenuous repair) | Pyloric exclusion + gastrojejunostomy |
| Definitive ulcer surgery | Selected stable low-risk patients only |
| Post-op essential | H. pylori eradication, high-dose PPI |
Sources: Current Surgical Therapy 14e (pp. 128-131); Fischer's Mastery of Surgery 8e (pp. 7753-7758); Schwartz's Principles of Surgery 11e (pp. 1279-1280)
This is a shared conversation. Sign in to Orris to start your own chat.