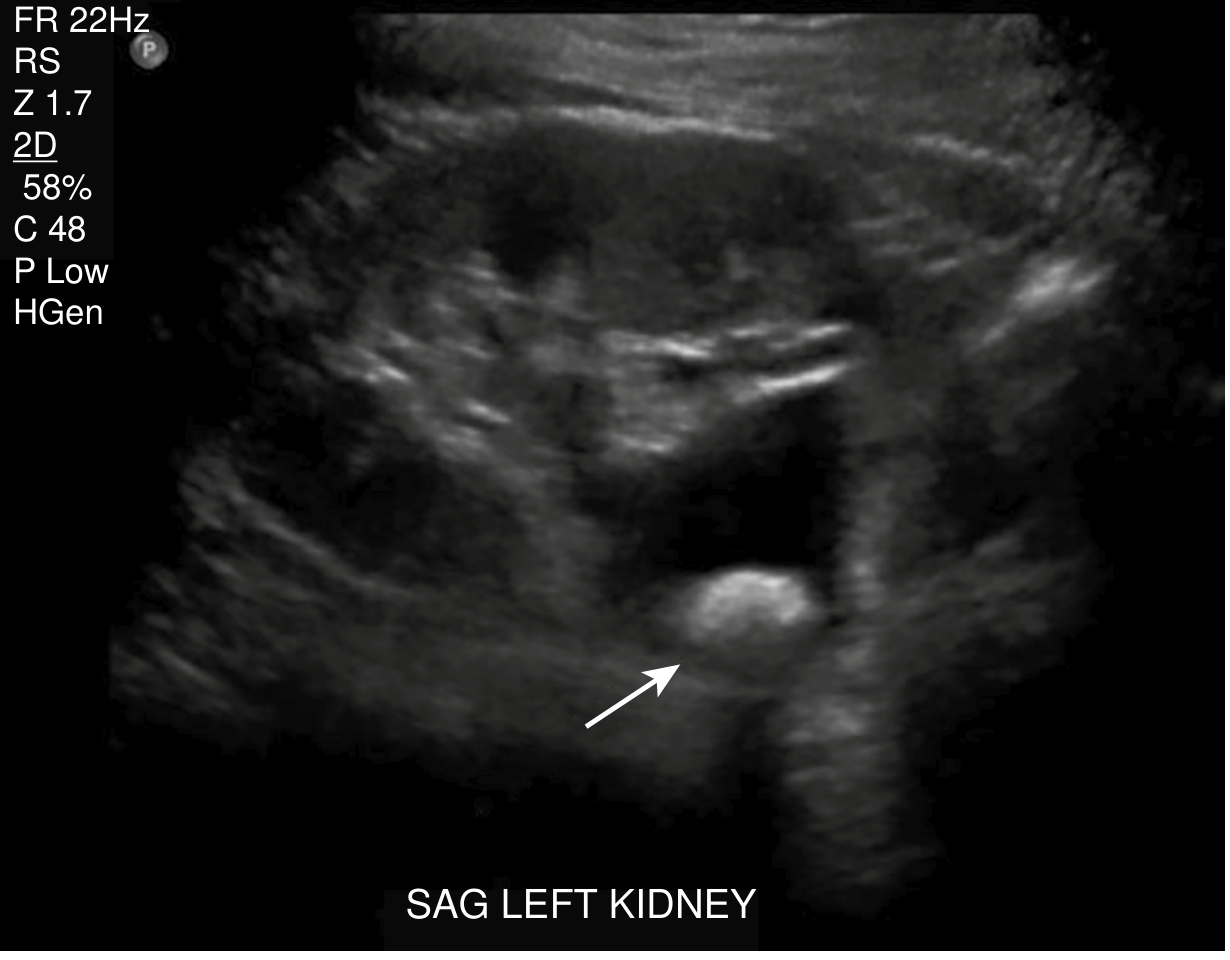
A 30-40 year old, shop keeper, with no known comorbids presented to the ER with *Anuria for 2 days.* Two days back he experienced right sided colicky pain that radiated to the back for which he went to a local hospital in Kashmir. He received unknown treatment that brought him relief. The next day he went to a doctor who did a ultrasound which showed mild hydronephrosis. Then he went to IKD where he was given lasix however no urine output still. O/E patient was vitally
bilateral ureteral obstruction anuria calculus acute kidney injury management
Clinical Analysis: Anuria Secondary to Obstructive Uropathy (Postrenal AKI)
Most Likely Diagnosis: Postrenal AKI due to Ureteral Stone Obstruction
| Feature | Interpretation |
|---|---|
| Right-sided colicky pain radiating to the back | Classic renal/ureteric colic from a calculus |
| Pain relieved (at local hospital) | Likely analgesia (NSAIDs/opioids) - stone not passed |
| Day 2: mild hydronephrosis on USG | Stone causing right ureteric obstruction |
| Day 2: Anuria begins | Either bilateral stones, OR right stone in a functionally/anatomically solitary kidney, OR contralateral obstruction developing |
| Lasix (furosemide) with NO response | Confirms postrenal obstruction - a loop diuretic cannot work if there is a mechanical block |
| Vitally stable | Reassuring - no sepsis, volume depletion, or hemodynamic shock |
Pathophysiology
- Bilateral ureteral obstruction (stone on each side)
- Unilateral obstruction in a patient with a solitary functioning kidney (e.g., congenital single kidney, contralateral chronic non-functioning kidney)
- Bladder outflow obstruction (less likely given the unilateral colic presentation)
"While often the primary imaging study because of low cost and lack of ionizing radiation, kidney ultrasound will be normal in about 50% of cases of acute urinary obstruction."
- NKF Primer on Kidney Diseases, 8e
Why Lasix Failed - And Why It Was the Wrong Move
- It can cause volume depletion in a patient who is already not making urine
- It delays definitive treatment
- It can worsen renal tubular injury from pressure-induced ischemia
Immediate Investigations Required
| Investigation | Purpose |
|---|---|
| Non-contrast CT KUB (NCCT) | Gold standard - identifies stone location, size, and degree of obstruction on both sides. Also rules out other causes |
| Serum creatinine, urea, electrolytes | Quantify AKI severity (K⁺, bicarbonate critical) |
| CBC | Rule out infection/leukocytosis |
| Urine output monitoring | Foley catheter to rule out bladder outlet obstruction |
| Blood cultures (if febrile) | Infected obstructed kidney = life-threatening emergency |
Definitive Management
"Relief of obstruction is crucial to reverse kidney impairment and preserve remaining kidney function... in upper tract obstruction, a double-J (DJ) stent is preferable, when possible. The most straightforward approach is endoscopic retrograde placement under fluoroscopy, with PCN (percutaneous nephrostomy) reserved for patients in whom the procedure fails."
- Foley catheter - First and fastest step to rule out bladder outlet obstruction
- Urgent urology referral - This is a surgical emergency
- NCCT abdomen/pelvis - Confirm stone burden and bilateral vs. unilateral status
- Retrograde DJ stenting (bilateral if bilateral obstruction) - Preferred endoscopic approach under fluoroscopy/GA
- Percutaneous nephrostomy (PCN) - If stenting fails, or if patient has infected system (pyonephrosis), PCN is done as emergency drainage
- In bilateral obstruction, draining the kidney with better-preserved parenchyma (by CT/USG) may be sufficient to restore function
- Correct electrolytes: Hyperkalemia is the immediate life threat - check K⁺ now and treat if >6.0 mEq/L (calcium gluconate, insulin+dextrose, sodium bicarbonate, kayexalate, consider HD if refractory)
- Hydration: Adequate IV fluids, but avoid overload in a patient with no urine output
Post-Decompression: Anticipate "Post-Obstructive Diuresis"
- Careful hourly urine output monitoring
- Electrolyte replacement (Na⁺, K⁺)
- Matching IV fluid replacement to avoid hypovolemia
Prognosis
- Duration of obstruction (48 hours in this case is relatively short - favorable)
- Degree of obstruction (complete vs. partial)
- Presence of infection (infected obstructed system worsens prognosis dramatically)
- Pre-existing renal reserve
"Because the extent of recovery of renal function in obstructive nephropathy is related inversely to the extent and duration of obstruction, prompt diagnosis and relief of obstruction are essential for effective management."
- Brenner and Rector's The Kidney
Red Flags to Watch For
- Fever + anuria + flank pain = infected obstructed kidney (pyonephrosis) - This is a septic emergency requiring emergency PCN within hours, not waiting for stenting
- Hyperkalemia (K⁺ >6.5) with ECG changes - needs immediate treatment
- Pulmonary edema from fluid overload without urine output
Summary
| Diagnosis | Postrenal AKI - bilateral ureteral obstruction from nephrolithiasis (or unilateral obstruction of a solitary kidney) |
| Why anuria | Complete mechanical block - no tubular flow possible |
| Why Lasix failed | Diuretics are useless against mechanical obstruction |
| Immediate priority | NCCT KUB + Foley + urgent urology for DJ stenting or PCN |
| Biggest immediate threat | Hyperkalemia and infected obstructed kidney |
| Prognosis | Excellent if decompressed promptly |
- NKF Primer on Kidney Diseases, 8e, p. 79
- Comprehensive Clinical Nephrology, 7th Edition
- Brenner and Rector's The Kidney, 2-Volume Set
- Harrison's Principles of Internal Medicine 22E
- Henry's Clinical Diagnosis and Management by Laboratory Methods
A 30-40 year old, shop keeper, with no known comorbids presented to the ER with *Anuria for 2 days.* Two days back he experienced right sided colicky pain that radiated to the back for which he went to a local hospital in Kashmir. He received unknown treatment that brought him relief. The next day he went to a doctor who did a ultrasound which showed mild hydronephrosis. Then went to IKD where he was given Lasix 120mg however no urine output still. O/E patient was vitally stable. Catheter was passed. No urine output. This patient has only one kidney. The other was removed due to fire arm injury. O/E patient was vitally
Clinical Analysis: Obstructing Calculus in a Solitary Kidney - Complete Postrenal AKI
The Diagnosis is Now Unequivocal
| Clinical Event | Explanation |
|---|---|
| Right colicky pain radiating to back | Calculus passing into the right ureter of his solitary kidney |
| Pain relief at local hospital | Analgesia administered - stone not passed |
| Day 2: Mild hydronephrosis on USG | Stone lodged in ureter causing proximal dilatation |
| Complete anuria begins | Stone fully occludes the single functioning ureter - no other kidney to compensate |
| Catheter passed - no urine | Bladder is empty because no urine is being produced - confirms upper tract (ureteral) obstruction, not bladder outlet obstruction |
| Lasix 120 mg - no response | Diuretics are categorically useless here - there is nothing to "push" through a blocked ureter |
| Vitally stable | No sepsis, no hemodynamic compromise yet - a window of opportunity |
Why This is a Urological Emergency - Not a Nephrology Problem
"Patients with a solitary kidney with obstruction" are listed explicitly as mandatory admission criteria for nephrolithiasis.
- Rosen's Emergency Medicine
"Complete obstruction with infection can lead to total destruction of the kidney within days. Partial return of GFR may follow relief of complete obstruction of 1 and 2 weeks' duration, but after 8 weeks of obstruction, recovery is unlikely."
- Harrison's Principles of Internal Medicine, 22E
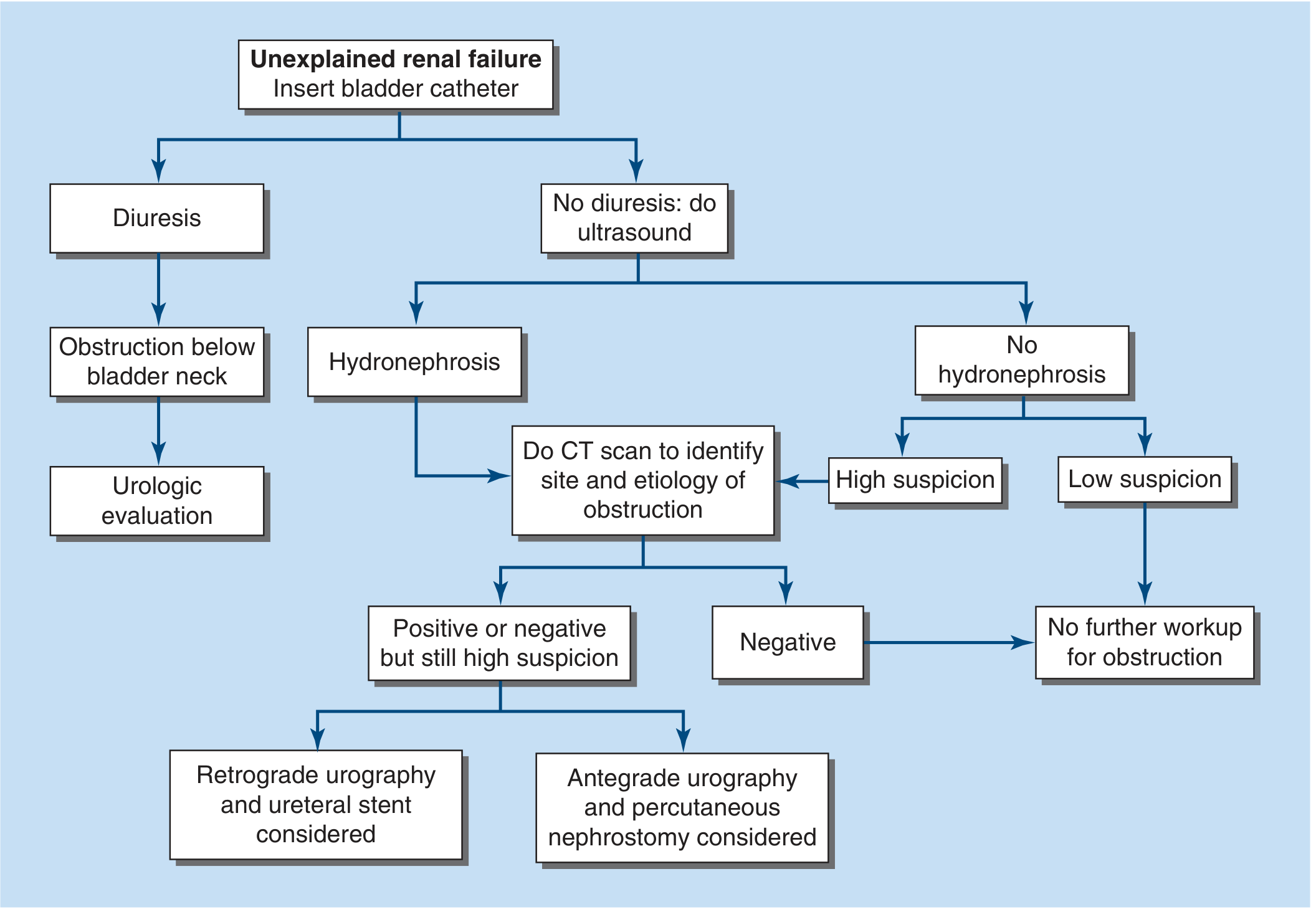
The Algorithmic Approach (Per Harrison's)
Immediate Priority: Investigations Right Now
| Investigation | Why Needed | Priority |
|---|---|---|
| Non-contrast CT KUB | Confirms stone site, size, degree of obstruction. Superior to USG (USG misses 50% of acute obstructions). Required before urological procedure | STAT |
| Serum creatinine, BUN, electrolytes | K⁺ is the most dangerous immediate threat. Creatinine quantifies AKI severity | STAT |
| ABG or venous blood gas | Assess metabolic acidosis (pH, HCO₃⁻) | STAT |
| CBC | WBC - rule out infected obstructed kidney (pyonephrosis) | STAT |
| Urine dipstick/culture | Nitrites, leukocytes - infection in an obstructed system = septic emergency | STAT |
| ECG | If K⁺ suspected high - peaked T-waves, wide QRS mean imminent arrhythmia | STAT |
Definitive Management: A Time-Sensitive Decision Tree
-
YES (infected obstructed kidney = pyonephrosis): This is a septic surgical emergency. Do emergency PCN (percutaneous nephrostomy) tonight. Do not wait for stenting under GA. Concurrent broad-spectrum IV antibiotics (e.g., piperacillin-tazobactam). Delay = septic shock + irreversible kidney loss within hours.
-
NO (afebrile, vitally stable - as stated here): Proceed to definitive decompression:
"When infection is not present, surgery is often delayed until acid-base, fluid, and electrolyte status is restored. Nevertheless, the site of obstruction should be ascertained as soon as feasible."
- Harrison's Principles of Internal Medicine, 22E
| Method | Details |
|---|---|
| Retrograde DJ (double-J) ureteral stenting | First choice. Cystoscopy under fluoroscopy, retrograde catheterization of the right ureter, guidewire past the stone, stent placed. Bypasses the stone, restores urine drainage immediately. Requires operative setup/GA or spinal |
| Percutaneous Nephrostomy (PCN) | If DJ stenting fails or patient cannot tolerate GA. Interventional radiology places a tube directly into the renal pelvis under USG/fluoroscopy guidance. Immediate drainage. Preferred in infection/sepsis. Success rate >90% |
| Both combined | If stent fails retrograde, antegrade stenting via nephrostomy track achieves >90% success |
"The retrograde approach involves catheterization of the involved ureter under cystoscopic control, whereas the antegrade technique necessitates percutaneous placement of a catheter into the renal pelvis. Although the antegrade approach may provide immediate decompression, many urologists initially attempt the retrograde approach unless catheterization is unsuccessful."
- Harrison's Principles of Internal Medicine, 22E
Managing the Immediate Metabolic Threats (While Awaiting Urology)
| K⁺ Level | Action |
|---|---|
| >5.5 with ECG changes (peaked T, widened QRS) | IV Calcium gluconate (membrane stabilizer) + Insulin/dextrose + Sodium bicarbonate + Salbutamol nebulization. Emergency HD if refractory |
| >6.5 regardless of ECG | Treat aggressively as above. Nephrology/HD on standby |
| Metabolic acidosis (HCO₃⁻ <15) | IV sodium bicarbonate infusion |
- IV fluids (NS or Ringer's) at maintenance - do NOT over-hydrate a patient with no urine output. Avoid fluid overload/pulmonary edema
- Once decompression is achieved, aggressive but monitored IV hydration to flush tubular debris and support urine flow
- Avoid NSAIDs (nephrotoxic in AKI)
- Opioid analgesia with caution (accumulation risk in renal failure)
- IV paracetamol is the safest analgesic here
Post-Decompression: Post-Obstructive Diuresis
"Relief of bilateral, but not unilateral, complete obstruction commonly results in polyuria, which may be massive. The urine is usually hypotonic and may contain large amounts of sodium chloride, potassium, phosphate, and magnesium... When extracellular volume and composition return to normal, the diuresis usually abates spontaneously."
- Harrison's Principles of Internal Medicine, 22E
- Hourly urine output measurement
- Replace ~50-75% of urine output with IV fluids to avoid both over and under-replacement
- Electrolyte monitoring every 4-6 hours (Na⁺, K⁺, Mg²⁺, PO₄²⁻)
- The diuresis is largely physiological and will self-limit
Definitive Stone Management (After Acute Phase Resolves)
- Ureteroscopy (URS) with laser lithotripsy - gold standard for ureteral stones in a solitary kidney; direct visualization, fragmentation, and extraction
- ESWL (extracorporeal shock wave lithotripsy) - option for smaller proximal stones; avoid in acute setting
- Stone analysis - sent for composition (calcium oxalate, uric acid, struvite, cystine) to guide long-term prevention
- Metabolic workup - 24-hour urine (calcium, oxalate, citrate, uric acid) after recovery, given the particular importance of stone prevention in a solitary kidney patient
Prognosis
- Favorable in this case: 48 hours of obstruction, young patient, no pre-existing comorbids, vitally stable, no infection
- Recovery of GFR is expected to be substantial with prompt decompression
- Risk of permanent AKI increases sharply after 1-2 weeks of complete obstruction; after 8 weeks it is unlikely to recover
- This patient must be counseled on the lifelong imperative of stone prevention - he has only one kidney and cannot afford recurrence
Summary in One Sentence
- Harrison's Principles of Internal Medicine, 22E - Chapter 331: Urinary Tract Obstruction
- Rosen's Emergency Medicine - Nephrolithiasis, Admission Criteria
- Comprehensive Clinical Nephrology, 7th Edition - Acute Management of Obstruction
- NKF Primer on Kidney Diseases, 8e - Obstructive Uropathy
Is it obstructive uropathy?
Definition Check
This Patient Meets Every Criterion
| Criterion | This Patient |
|---|---|
| Mechanical obstruction to urine flow | Calculus lodged in the right ureter |
| Upstream consequences | Mild hydronephrosis on USG (pelvicalyceal dilation from back-pressure) |
| Functional consequence | Complete anuria - zero urine output for 48 hours |
| AKI as result | Presumed elevated creatinine/uremia |
| Catheter with no output | Confirms bladder is empty - obstruction is at ureteral level, not bladder outlet |
| Lasix failure | No urine despite 120mg furosemide - the tubules have nothing to work with |
Where Exactly is the Obstruction?
Renal calyx → Renal pelvis → Ureter ← STONE HERE → Bladder → Urethra
↑
Obstruction point
(hydronephrosis developing above this)
Obstructive Uropathy vs. Obstructive Nephropathy - The Distinction
- Obstructive uropathy = the mechanical obstruction itself (the stone in the ureter)
- Obstructive nephropathy = the renal parenchymal damage resulting from that obstruction (what is happening to his solitary kidney right now as back-pressure builds and GFR falls)
The Only Caveat Worth Mentioning
- Bilateral ureteral obstruction, OR
- Obstruction of a solitary functioning kidney
What investigations and treatment i should do for this patient now? Its Sunday and it's 6 am
Do These Simultaneously - Right Now
1. Bloods - STAT
| Test | What You're Looking For |
|---|---|
| Serum Creatinine + Urea | Quantify AKI severity |
| Serum Electrolytes (Na⁺, K⁺) | K⁺ is the killer. >6.5 = treat before anything else |
| ABG or VBG | pH, HCO₃⁻ - degree of metabolic acidosis |
| CBC | WBC - is there infection brewing? (pyonephrosis) |
| Blood cultures x2 | If any fever, even low-grade |
| Serum uric acid, calcium | Stone metabolic workup (secondary priority) |
2. ECG - Right Now, Takes 2 Minutes
- Peaked T-waves = K⁺ likely >6.0
- Wide QRS = K⁺ likely >7.0, cardiac arrest imminent
- If any ECG changes: treat hyperkalemia before you do anything else
3. Non-Contrast CT KUB - STAT
- Exact location of the stone in the ureter (upper, mid, lower third)
- Size of the stone (determines if it can pass spontaneously or needs intervention)
- Degree of hydronephrosis
- Whether there is perinephric fat stranding (infection/inflammation)
- Whether the stone is impacted
4. Urine - Whatever Drains Into the Catheter Bag
- Dipstick: nitrites/leukocytes (infection?)
- Microscopy, culture and sensitivity
Treat Simultaneously While Awaiting Results
IV Access - Two Large-Bore Cannulas
IV Fluids
If K⁺ comes back >6.0 or ECG shows changes - treat immediately:
| Drug | Dose | Purpose | Onset |
|---|---|---|---|
| Calcium Gluconate 10% | 10 mL IV over 10 min | Cardiac membrane stabilizer - buys time | 1-3 min |
| Insulin (Actrapid) + 50% Dextrose | 10 units + 50 mL IV | Shifts K⁺ intracellularly | 15-30 min |
| Sodium Bicarbonate 8.4% | 50-100 mL IV | Shifts K⁺, corrects acidosis | 30 min |
| Salbutamol | 10-20 mg nebulized | Shifts K⁺ intracellularly | 15-30 min |
| Calcium Resonium | 15g orally or PR | Eliminates K⁺ from gut | Hours |
If K⁺ >7.0 or refractory: emergency dialysis. Call the nephrologist now, regardless of the hour.
Pain Management
- IV Paracetamol 1g - safest in AKI
- Avoid NSAIDs - nephrotoxic, absolutely contraindicated in AKI with a solitary kidney
- Tramadol/morphine small dose with caution - accumulates in renal failure
The Most Important Call You Make Today
Call the On-Call Urologist NOW
"I have a patient with a solitary kidney, right ureteral calculus, complete anuria for 48 hours, catheter draining nothing. He needs urgent urological decompression. CT is being done now."
- Retrograde DJ stenting (cystoscopy, preferably first-line)
- Percutaneous Nephrostomy / PCN (if no cystoscopy available at 6am on Sunday, or if stenting fails)
If There is ANY Fever or Signs of Infection
- IV Piperacillin-Tazobactam 4.5g (or Meropenem if septic/penicillin allergic)
- Call urology for emergency PCN tonight - do not wait
Decision Timeline
RIGHT NOW (0-30 min)
├── ECG
├── IV access + bloods sent
├── NCCT KUB ordered
├── Treat hyperkalemia if present
└── Call on-call urologist
30-60 min
├── Results back - reassess K⁺, pH
├── CT images available
└── Urologist reviews and plans decompression
As soon as urologist available
└── DJ stenting OR PCN
→ Urine output should begin within minutes of decompression
→ Watch for post-obstructive diuresis (replace fluids accordingly)
What You Do NOT Do
- ❌ Give more Lasix - it will not work and wastes time
- ❌ Wait until Monday for urology
- ❌ Aggressively fluid-load
- ❌ Give NSAIDs for pain
- ❌ Discharge or observe conservatively
A 30-40 year old, shop keeper, with no known comorbids presented to the ER with *Anuria for 2 days.* Two days back he experienced right sided colicky pain that radiated to the back for which he went to a local hospital in Kashmir. He received unknown treatment that brought him relief. The next day he went to someone who did a ultrasound which showed mild hydronephrosis and nephrolithiasis. However, the person told them it is a gastric issue. He straight away travelled from kashmir to IKD where he received Lasix 120mg however he didn't produce any urine output. So, he decided to come to the ER. O/E patient was vitally and clinically stable. Neither dehydrated nor overloaded. Abdomen soft, non-tender, non palpable bladder, gut sounds audible. *Its worth mentioning that this patient has removed left kidney due to a fire arm injury in 2014* I have only started on maintenance fluids 80ml/hr and punched basic labs and a CT-KUB.
While You Wait for Results - What to Watch
- Any arrhythmia - AF, bradycardia, wide-complex rhythms = hyperkalemia until proven otherwise
- BP trending down - unlikely given he's stable, but watch
- Any temperature spike - changes everything (see pyonephrosis below)
When the Labs Come Back
The K⁺ Result is Your Most Urgent Number
| K⁺ | Action |
|---|---|
| <5.5 | Good. Continue monitoring. Focus shifts entirely to decompression |
| 5.5 - 6.0 | Start calcium resonium 15g orally. Repeat K⁺ in 2 hours. Alert urology urgently |
| 6.0 - 6.5 | IV insulin/dextrose + sodium bicarbonate + nebulized salbutamol. Call urology emergently |
| >6.5 or ECG changes | Calcium gluconate 10 mL IV immediately + full treatment above. Get nephrology/dialysis on standby. This is a cardiac emergency |
Creatinine
- Will almost certainly be markedly elevated after 48 hours of anuria in a solitary kidney
- The number itself doesn't change immediate management - decompression is needed regardless
- But it establishes a baseline and helps nephrology decide if HD is needed post-decompression
CBC
- WBC elevated? = Suspect infected obstructed kidney even if afebrile. Start IV antibiotics immediately and escalate urgency of decompression
- Normal WBC + afebrile = proceed with elective-urgent decompression
When the CT-KUB Comes Back
| Location | Implication |
|---|---|
| Upper ureter / UPJ | Harder to stent retrogradely, may need PCN first |
| Mid ureter | Moderate difficulty for stenting |
| Lower ureter / VUJ | Most accessible retrogradely, easiest to stent |
| Size | Implication |
|---|---|
| <6mm | Could potentially pass spontaneously with alpha-blockers (tamsulosin) - BUT NOT in a solitary kidney with anuria. Do not observe. Decompress. |
| 6-10mm | Unlikely to pass on its own. Needs intervention |
| >10mm | Will not pass. Definitive urological intervention required |
- Stranding around the kidney = inflammation/early infection = escalate urgency, consider antibiotics
- Mild (as on USG) suggests relatively recent or partial obstruction - kidney likely salvageable
- Severe = more urgent, longer standing
The Call You Need to Make Now
- Right solitary kidney (left nephrectomy 2014 - firearm injury)
- Ureteral calculus at [location from CT] measuring [size]
- Complete anuria 48 hours
- Hemodynamically and clinically stable, afebrile
- K⁺: [result]
- Creatinine: [result]
Option A: Retrograde DJ Stenting
- Cystoscopy under spinal/GA
- Pass guidewire past the stone, deploy double-J stent
- Preferred if stone is mid/lower ureter and theatre is accessible
Option B: Percutaneous Nephrostomy (PCN)
- More feasible at odd hours on a Sunday
- Done under USG/fluoroscopy by interventional radiology or a trained urologist
- Local anaesthesia - does not need GA
- Directly decompresses the renal pelvis within minutes
- Most practical option right now given the time
One Scenario That Changes Everything
- Fever >38°C, OR
- Rigors, OR
- Rising WBC with left shift, OR
- Hypotension
- Start IV Piperacillin-Tazobactam 4.5g immediately
- Emergency PCN tonight
- This can kill within hours
After Decompression - Anticipate Massive Diuresis
- Match ~50-75% of hourly urine output with IV fluids
- Monitor electrolytes every 4-6 hours (K⁺ can drop precipitously as it washes out)
- The diuresis will self-limit once retained solutes are cleared
- Avoid both over-replacing (prolongs diuresis) and under-replacing (hypovolemia)
Your Current Management Score
| Action | Status |
|---|---|
| Maintenance IV fluids 80 mL/hr | ✅ Correct |
| Basic labs sent | ✅ Correct |
| CT-KUB ordered | ✅ Correct |
| Catheter passed | ✅ (confirmed no bladder outlet obstruction) |
| Monitor vitals continuously | ✅ Do this if not already |
| ECG | Do this now if not done |
| On-call urologist alerted | Do this as soon as CT is ready |
TLC is 11.4, CRP is 3.4. Should I start antibiotics? Which antibiotics?
Interpreting These Results in Context
| Result | Value | Interpretation |
|---|---|---|
| TLC 11.4 | Mildly elevated (normal <11.0) | Borderline. Barely above normal |
| CRP 3.4 | Mildly elevated (normal <5 mg/L typically) | Low-level inflammation |
- Stress response - he's been in pain, travelled from Kashmir, anxious
- Pain itself - cortisol-mediated demargination of neutrophils
- The obstructive process - tissue inflammation from back-pressure
- Early infection - possible but not confirmed
Should You Start Antibiotics Now?
- ✅ Afebrile
- ✅ Hemodynamically stable
- ✅ Clinically stable
- ✅ TLC only marginally elevated
- ✅ CRP barely elevated
- Many antibiotics are nephrotoxic or require dose adjustment in renal failure
- Premature antibiotics can mask evolving sepsis without treating it properly
- You want to send cultures before starting antibiotics
What You Must Do Before Antibiotics
The Trigger Points for Starting Antibiotics
| Trigger | Antibiotic |
|---|---|
| Fever >38°C | Yes - start now |
| Temperature <36°C (hypothermia) | Yes - sepsis equivalent |
| Tachycardia >100 that is new | Reassess, likely start |
| Hypotension (SBP <90) | Yes - septic shock protocol |
| WBC >15 with left shift (bands) | Yes |
| CT shows perinephric stranding + fat infiltration | Strong indication to start |
| CT shows air in collecting system | Emergency - pyonephrosis |
If You Do Decide to Start (or CT shows stranding)
- IV Ceftriaxone 1g OD - excellent gram-negative cover, renally dosed, widely available, safe
- IV Piperacillin-Tazobactam 4.5g TDS - broader cover including Pseudomonas
- ❌ Aminoglycosides (gentamicin) - nephrotoxic, avoid in AKI
- ❌ NSAIDs for any reason
- ❌ Nitrofurantoin - ineffective in upper tract infection and contraindicated in renal failure