Prepare me femur for my viva of anatomy first year mbbs university exams using animation diagram
femur bone anatomy labeled diagram first year MBBS viva
femur bone sides identification angle inclination torsion neck shaft MBBS anatomy viva questions
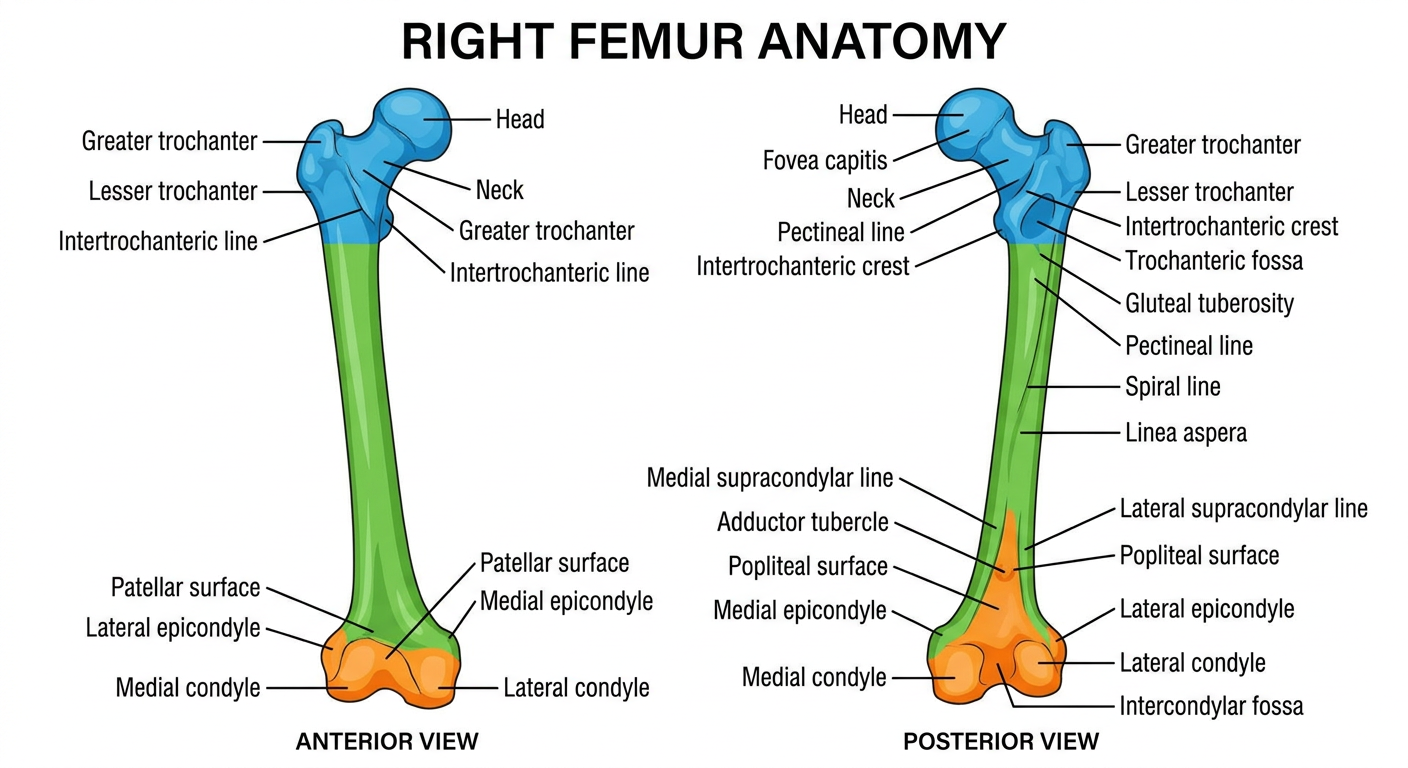
Detailed anatomical illustration of the right femur bone showing anterior and posterior views with all labeled parts: head, fovea capitis, neck, greater trochanter, lesser trochanter, intertrochanteric line (anterior), intertrochanteric crest (posterior), gluteal tuberosity, pectineal line, linea aspera, spiral line, medial and lateral supracondylar lines, adductor tubercle, popliteal surface, medial epicondyle, lateral epicondyle, medial condyle, lateral condyle, intercondylar fossa, patellar surface, trochanteric fossa. Educational medical diagram style, clean white background, color-coded regions for proximal end, shaft, and distal end, bright colors, clear labels with leader lines
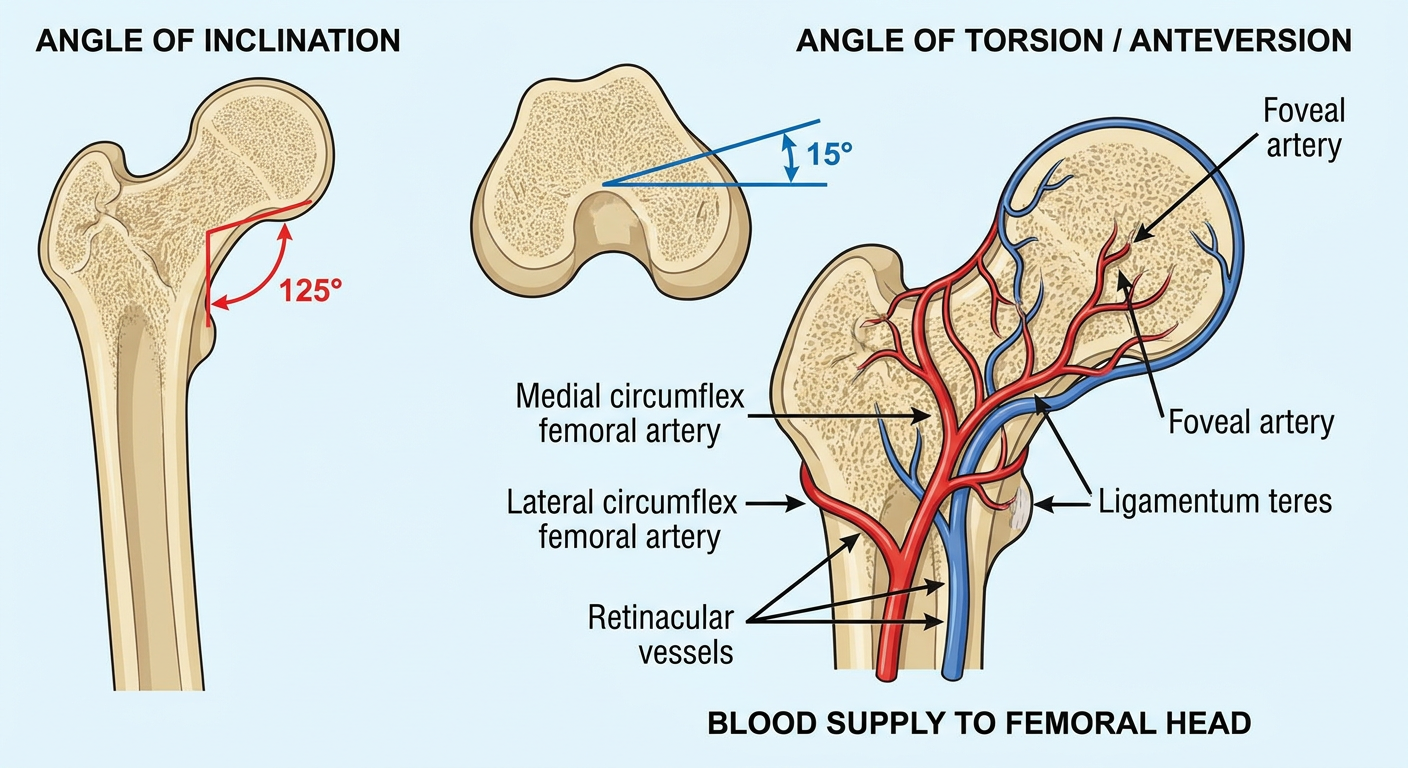
Cross-section diagram of femur neck showing angle of inclination (125 degrees) and angle of torsion/anteversion (15 degrees), with blood supply diagram showing medial and lateral circumflex femoral arteries, retinacular vessels, and foveal artery. Medical education illustration style, labeled, colorful, clear background
https://teachmeanatomy.info/lower-limb/bones/femur
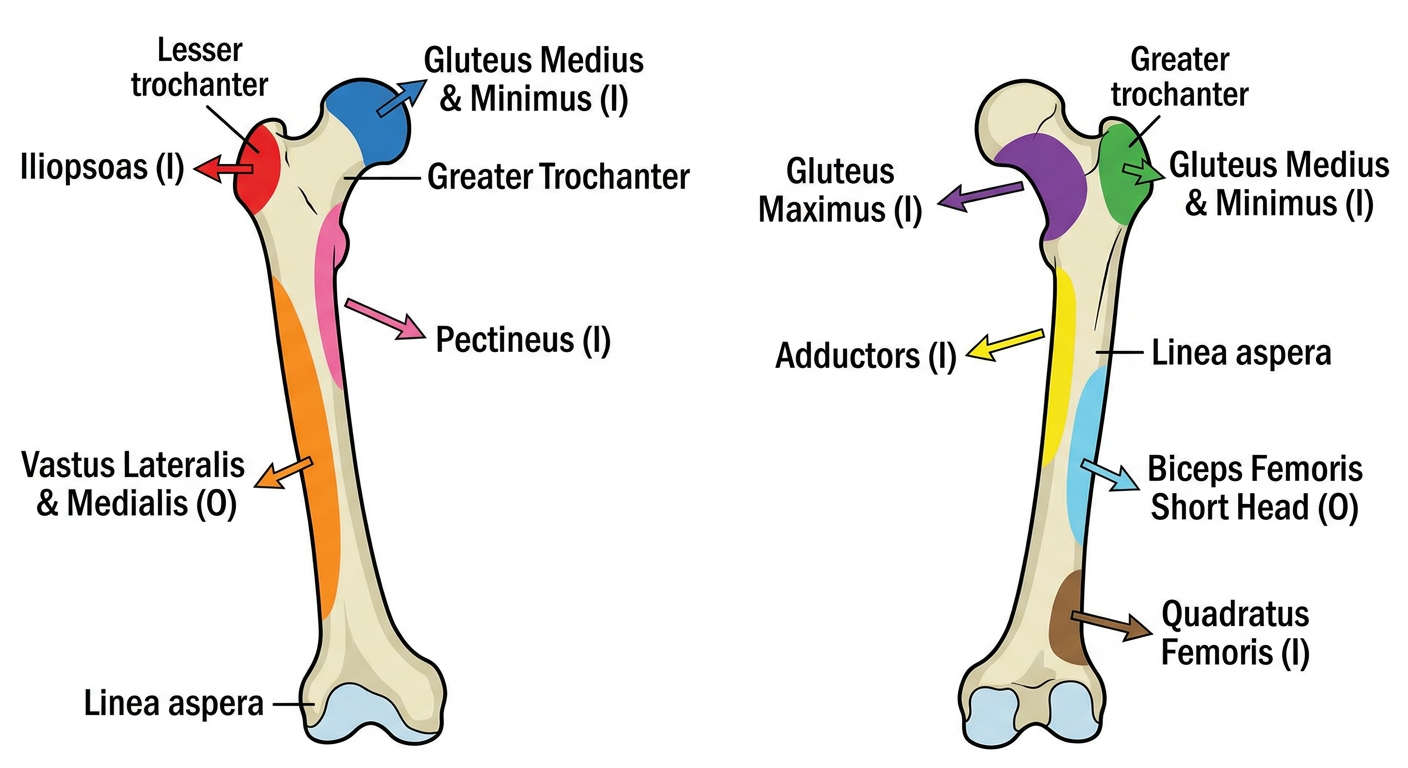
Muscle attachments diagram of femur bone, anterior and posterior views, color-coded muscles: iliopsoas on lesser trochanter, gluteus maximus on gluteal tuberosity, gluteus medius and minimus on greater trochanter, vastus lateralis and medialis on linea aspera, adductors on linea aspera, biceps femoris short head on linea aspera, pectineus on pectineal line, quadratus femoris on quadrate tubercle. Medical education style, bright distinct colors for each muscle, arrows indicating origin vs insertion, clean white background with labels
🦴 FEMUR - Complete First Year MBBS Anatomy Viva Guide
📍 DIAGRAM 1 - Bony Landmarks (Anterior & Posterior Views)

📍 DIAGRAM 2 - Angles & Blood Supply
📍 DIAGRAM 3 - Muscle Attachments
📌 INTRODUCTION
📌 SIDE DETERMINATION (Critical Viva Topic!)
- Head - faces medially, upward, and slightly forward
- Greater trochanter - lateral and posteriorly placed
- Lesser trochanter - medial and posterior
- Linea aspera - on the posterior surface
- Patellar surface (trochlear groove) - on the anterior aspect of distal end
Rule: Hold the bone upright with head upward. The head should point medially. The lesser trochanter should be on the posteromedial side. The side to which the head points = the side of the bone.
📌 PARTS OF THE FEMUR
1. PROXIMAL END
| Structure | Key Facts |
|---|---|
| Head | 2/3 of a sphere; covered with hyaline cartilage (except fovea capitis) |
| Fovea capitis | Small pit on head; attachment of ligamentum teres (round ligament) |
| Neck | Connects head to shaft; directed upward, medially, and anteriorly |
| Greater trochanter | Lateral projection; largest bony landmark of proximal femur |
| Lesser trochanter | Posteromedial projection; smaller |
| Intertrochanteric line | Anterior; connects greater and lesser trochanter anteriorly |
| Intertrochanteric crest | Posterior; connects the two trochanters posteriorly (with quadrate tubercle) |
| Trochanteric fossa | Depression on medial surface of greater trochanter (posterior); obturator externus attaches |
2. SHAFT (BODY)
| Feature | Details |
|---|---|
| Shape | Cylindrical; slightly convex anteriorly |
| Linea aspera | Prominent posterior ridge; medial and lateral lips |
| Pectineal line | Upward continuation of medial lip (pectineus attaches) |
| Gluteal tuberosity | Upward continuation of lateral lip; gluteus maximus attaches |
| Spiral line | Runs from lesser trochanter spirally to medial lip of linea aspera |
| Nutrient foramen | Usually in middle third; directed upward (away from knee) |
| Medial & Lateral supracondylar lines | Distal continuation of linea aspera lips |
| Popliteal surface | Flat triangular area posteriorly between the two supracondylar lines |
3. DISTAL END
| Structure | Key Facts |
|---|---|
| Medial condyle | Projects more inferiorly (compensates for oblique shaft) |
| Lateral condyle | Shorter but stouter; articulates with tibia |
| Intercondylar fossa | Posterior; attachment of cruciate ligaments (ACL - lateral wall; PCL - medial wall) |
| Medial epicondyle | Most prominent bony point on medial side; medial collateral ligament attaches |
| Lateral epicondyle | Lateral; lateral collateral ligament attaches |
| Adductor tubercle | Projection above medial epicondyle; adductor magnus (tendinous part) attaches |
| Patellar surface | Anteroinferior; articulates with patella |
📌 IMPORTANT ANGLES (High-Yield Viva!)
Angle of Inclination (Neck-Shaft Angle)
- Adult: 125-130° (average 126°)
- At birth: ~150°
- Coxa valga = angle > 130° (seen in rickets, polio)
- Coxa vara = angle < 120° (predisposes to neck of femur fractures)
Angle of Torsion / Anteversion
- The neck is twisted anteriorly relative to the shaft condylar axis
- Normal adult: ~15° anteriorly
- At birth: ~35°
- Increased anteversion = in-toeing gait
- Retroversion = out-toeing gait
📌 MUSCLE ATTACHMENTS (Viva Favourite!)
PROXIMAL END
| Muscle | Attachment Site |
|---|---|
| Iliopsoas | Lesser trochanter (insertion) |
| Gluteus medius | Greater trochanter - lateral surface (insertion) |
| Gluteus minimus | Greater trochanter - anterior surface (insertion) |
| Piriformis | Greater trochanter - medial surface/tip (insertion) |
| Obturator internus + 2 gemelli | Greater trochanter - medial surface (insertion) |
| Obturator externus | Trochanteric fossa (insertion) |
| Quadratus femoris | Quadrate tubercle on intertrochanteric crest (insertion) |
SHAFT - Linea Aspera (Medial Lip)
- Adductor longus, brevis, magnus
- Vastus medialis
- Pectineus (upper part)
SHAFT - Linea Aspera (Lateral Lip)
- Biceps femoris (short head) - only flexor arising from femur
- Vastus lateralis
- Gluteus maximus (lower fibers via iliotibial tract)
DISTAL END
- Medial collateral ligament - medial epicondyle
- Lateral collateral ligament - lateral epicondyle
- Adductor magnus (tendinous) - adductor tubercle
- Cruciate ligaments - intercondylar fossa
📌 BLOOD SUPPLY OF FEMORAL HEAD
- Medial circumflex femoral artery (MCFA) - most important; via retinacular vessels
- Lateral circumflex femoral artery (LCFA) - minor contribution
- Artery of ligamentum teres (foveal artery from obturator artery) - minor; important in children
Clinical: In neck of femur fractures, the retinacular vessels (mainly MCFA) are torn → avascular necrosis (AVN) of femoral head
📌 OSSIFICATION (VIVA ESSENTIAL!)
| Centre | Appears | Fuses |
|---|---|---|
| Shaft (primary) | 7th week of intrauterine life (IUL) | - |
| Head | Birth - 1st year | 18 years |
| Greater trochanter | 4th year | 18 years |
| Lesser trochanter | 13-14th year | 18 years |
| Lower end | 9th month of IUL (last to appear before birth; present at birth) | 20 years |
Important: Lower end ossification centre is present at birth = used to determine if the baby was born alive (medico-legal significance!)
📌 FRACTURES - CLINICAL CORRELATIONS
Neck of Femur Fractures
- Common in elderly females (post-menopausal osteoporosis)
- Presentation: shortened + externally rotated lower limb
- Intracapsular (subcapital/transcervical): risk of AVN
- Extracapsular (intertrochanteric/subtrochanteric): less AVN risk
Shaft Fractures
- Typically require significant force
- May damage profunda femoris artery → significant blood loss (up to 1-2L blood can be lost)
Garden Classification (Neck of Femur Fractures)
- Grade I: Incomplete/impacted
- Grade II: Complete, undisplaced
- Grade III: Complete, partially displaced
- Grade IV: Complete, fully displaced
📌 QUICK VIVA Q&A
| Q | A |
|---|---|
| Which is the longest bone in the body? | Femur |
| What is the angle of inclination? | 125-130° |
| What is the angle of torsion? | 15° anteriorly |
| Which muscle attaches to fovea capitis? | Ligamentum teres (round ligament) |
| Which is the only flexor arising from femur? | Biceps femoris short head (from linea aspera) |
| What is the nutrient foramen direction? | Directed upward (away from knee) |
| Ossification centre at birth? | Lower end (9th month IUL) |
| Blood supply of femoral head - main source? | Medial circumflex femoral artery (retinacular vessels) |
| Coxa vara angle? | < 120° |
| What attaches to adductor tubercle? | Adductor magnus (tendinous part) |
| What are the cruciate ligaments attached to? | Intercondylar fossa |
| What is the medico-legal significance of lower end ossification? | Confirms live birth (present at 9th month of IUL) |
📌 QUICK MEMORY TIPS
- LINEA ASPERA = "Rough Line" - remember 3 lines converge to form it proximally: Gluteal tuberosity (lateral) + Pectineal line (medial) + Spiral line
- Neck fracture = externally rotated - iliopsoas pulls the distal fragment, also the limb shortens
- "Last to appear, first to fuse" does NOT apply to femur - lower end appears 9th month IUL and fuses at 20 years
- "Go Left, Look Left" - to determine side, hold upright, head of femur points to that side