Hey, so my customer has, my patient has a stomach ache. What should I offer to this patient? Or look for in this patient? Sorry.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Now I have enough information for a solid, structured clinical answer. Here it is:
Approach to a Patient with Abdominal Pain ("Stomach Ache")
Abdominal pain is one of the broadest presentations in medicine. It can be benign and self-limited, or the first sign of a life-threatening emergency. Your job is to systematically narrow the differential.
Step 1: History - the most important tool
Ask about these key features:
| Feature | What to ask | Why it matters |
|---|---|---|
| Onset | Sudden/explosive vs. gradual? | Sudden = perforation, AAA rupture, ischemia; gradual = appendicitis, cholecystitis |
| Location | Where exactly? Does it move? | Guides your differential (see below) |
| Character | Sharp, crampy, burning, steady, colicky? | Colicky = obstructed viscus; steady = inflammation/ischemia |
| Severity | Scale 1-10 | Severe out-of-proportion to exam = ischemia |
| Radiation | Does it spread anywhere? | Epigastric to back = pancreatitis; RUQ to right scapula = cholecystitis |
| Timing | Constant vs. intermittent? Duration? | Chronic (>6 months) vs. acute vs. subacute |
| Aggravating/relieving | Food, movement, position, BMs, antacids? | Eating worsens pancreatitis; eating may relieve PUD |
| Associated symptoms | Nausea, vomiting, fever, diarrhea, constipation, bloody stool, jaundice, dysuria, weight loss | Fever + RLQ = appendicitis; jaundice = biliary/liver |
| Last menstrual period | In women of reproductive age | Ectopic pregnancy is a must-not-miss |
Red flag features suggesting an organic/serious process: fever, night sweats, weight loss, appetite change, or nocturnal awakening from pain.
Step 2: Location-based differential
| Region | Top diagnoses to consider |
|---|---|
| Epigastric | PUD, GERD, acute pancreatitis, gastritis, early MI |
| RUQ | Cholecystitis, hepatitis, biliary colic |
| LUQ | Splenic pathology, gastric ulcer |
| Periumbilical | Early appendicitis, small bowel obstruction, intestinal ischemia, AAA |
| RLQ | Appendicitis, ovarian cyst/torsion (women), Crohn's disease |
| LLQ | Diverticulitis, ovarian cyst/torsion (women), constipation |
| Suprapubic | UTI, pelvic pathology, bladder |
| Diffuse | Peritonitis, ischemia, IBS, early obstruction |
Step 3: Physical Examination
- Inspection: Distension, visible peristalsis, surgical scars
- Auscultation: High-pitched or absent bowel sounds (obstruction vs. ileus)
- Percussion: Tympany (gas/obstruction), dullness (fluid/mass), loss of liver dullness (free air)
- Palpation: Tenderness location, guarding (voluntary vs. involuntary), rigidity, rebound tenderness
- Special signs: Murphy's sign (cholecystitis), McBurney's point (appendicitis), Rovsing's, psoas/obturator signs
- Don't miss: Hernial orifices (strangulated hernia), costovertebral angle tenderness (pyelonephritis), pelvic exam in women
Involuntary guarding + rebound + rigidity = peritonitis = surgical emergency
Step 4: Immediate triage - does this need urgent surgery?
Conditions requiring urgent surgical evaluation include:
- Bowel perforation
- Acute appendicitis
- Strangulated hernia
- Intestinal ischemia/obstruction
- Ruptured ectopic pregnancy
- Severe colitis with perforation risk
- Acute cholecystitis (may need intervention)
Step 5: Investigations (guided by history/exam)
- Labs: CBC (WBC elevation with infection/inflammation), CMP (liver enzymes, bilirubin), lipase/amylase (pancreatitis), urinalysis (UTI, kidney stone), beta-hCG in women
- Imaging: Abdominal X-ray (obstruction, free air), Ultrasound (gallbladder, ovaries, appendix in thin patients), CT abdomen/pelvis (gold standard for most acute causes), MRI if concerned about radiation
- ECG: In older patients - inferior MI can present as epigastric pain
Common diagnoses at a glance
| Diagnosis | Key clue |
|---|---|
| PUD | Epigastric burning, H. pylori risk, NSAID/aspirin use |
| Acute pancreatitis | Epigastric radiating to back, elevated lipase, alcohol/gallstones |
| Cholecystitis | RUQ pain after fatty meal, Murphy's sign, fever |
| Appendicitis | Periumbilical pain migrating to RLQ, anorexia, fever |
| Diverticulitis | LLQ pain, fever, older adult, elevated WBC |
| IBS | Chronic crampy pain, relieved by BM, no alarm features |
| GERD | Burning epigastric/substernal, worse lying down or after meals |
| Ectopic pregnancy | Women of reproductive age, pelvic pain + amenorrhea = emergency |
| Intestinal ischemia | Severe pain out of proportion to exam, cardiac risk factors |
The key takeaway is: start with a thorough history and physical exam - those will direct your workup more than any single test. And always ask yourself first: "Does this patient need surgery or urgent intervention right now?"
(Goldman-Cecil Medicine, Chapter 118; Sleisenger & Fordtran's GI and Liver Disease, Chapter 12)
alopcia arreata images
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive visual overview of Alopecia Areata from the medical textbook library:
Alopecia Areata - Clinical Images
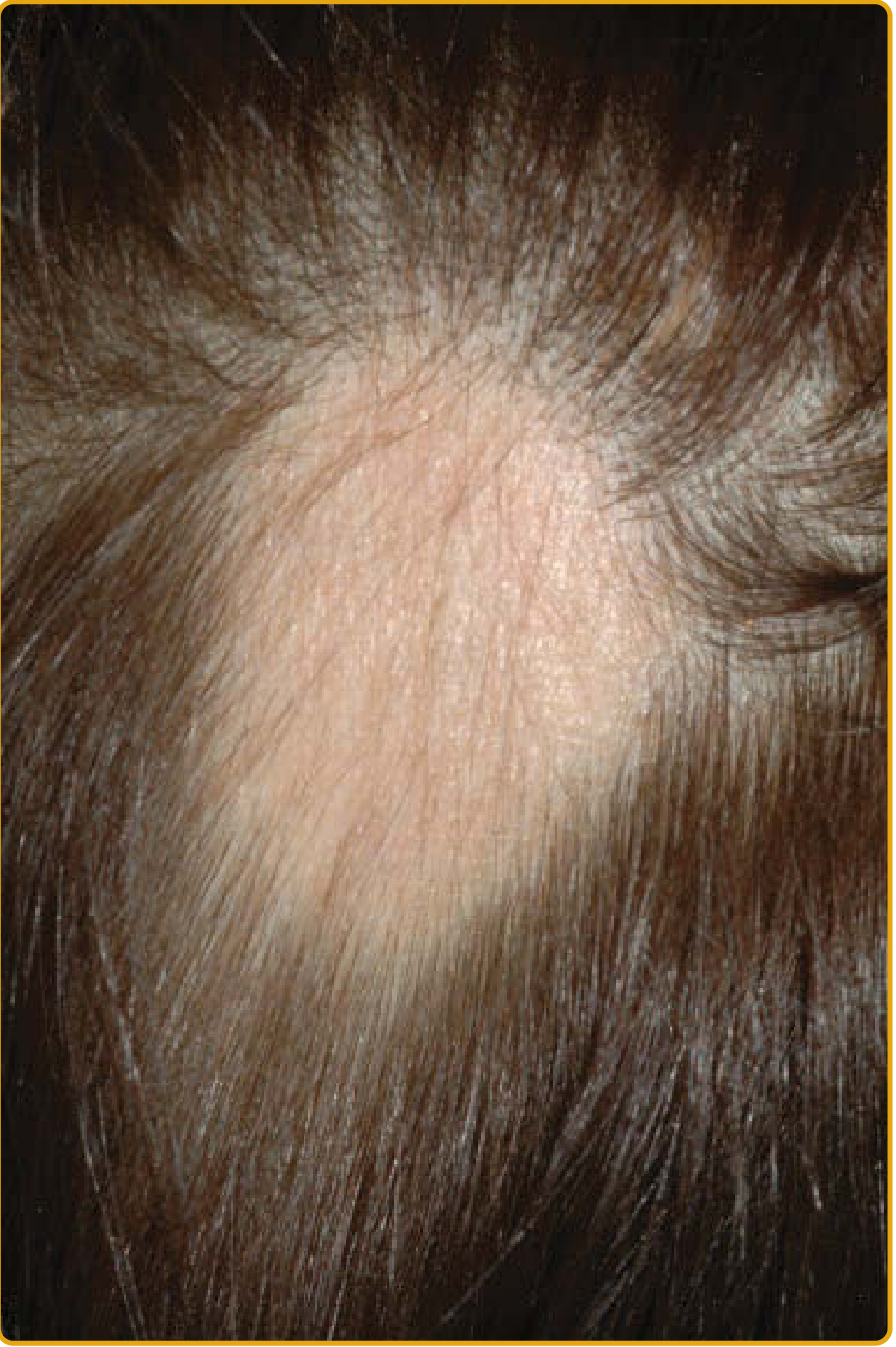
1. Classic Patchy Alopecia Areata (Scalp)
A single well-circumscribed, smooth oval patch of hair loss on the scalp - the most common presentation:
2. Patchy Alopecia Areata (Multiple Confluent Patches)
Multiple patches coalescing across the scalp, with white/gray hairs typically spared:

3. Alopecia Areata with Exclamation Point Hairs
Close-up showing residual broken short hairs at the patch edge - the pathognomonic "exclamation point" hairs (tapered proximally, blunt distally):

4. Alopecia Totalis
Complete loss of all scalp hair:

5. Eyebrow Involvement
Loss of eyebrows - a characteristic extra-scalp manifestation:

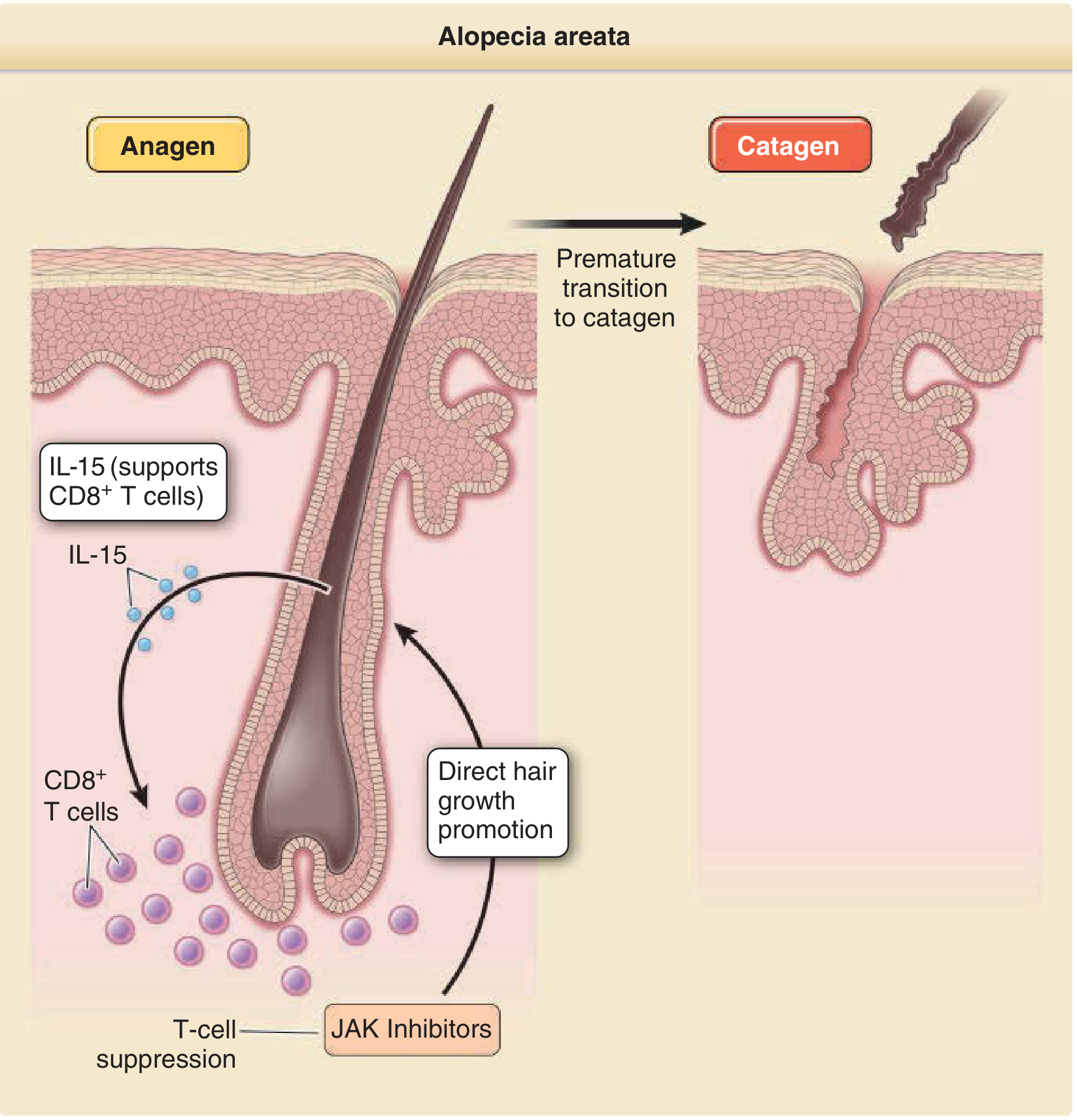
6. Pathogenesis Diagram
The underlying mechanism - CD8+ T cells attack the hair bulb, causing premature catagen transition (and why JAK inhibitors work):
Key Clinical Clues at a Glance
| Feature | Description |
|---|---|
| Patch shape | Round/oval, well-demarcated, smooth scalp |
| Exclamation point hairs | Short, tapered at base - at patch borders |
| Black dots | Broken-off hair stubs in follicular openings (dermoscopy) |
| Yellow dots | Empty follicles filled with keratin/sebum (dermoscopy) |
| Nail pitting | Grid-like pitting in ~10% of patients |
| White hair sparing | Pigmented hairs targeted; white/gray hairs often spared |
| Variants | Patchy → Ophiasis → Totalis → Universalis |
(Sources: Fitzpatrick's Dermatology, Andrews' Diseases of the Skin, Dermatology 2-Volume Set 5e)
This is a shared conversation. Sign in to Orris to start your own chat.