Aspergilloma for md exams 10 marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive material to write a thorough 10-mark answer. Let me compile everything:
Aspergilloma
Definition
Aspergilloma (also called mycetoma or fungus ball) is the saprophytic colonization of a pre-existing pulmonary cavity by Aspergillus species, most commonly A. fumigatus. The fungal hyphae, mucus, cellular debris, and fibrin accumulate within the cavity to form a rounded mass. It is now classified as a form of Chronic Pulmonary Aspergillosis (CPA).
- Fishman's Pulmonary Diseases and Disorders, p. 2329
Etiology and Predisposing Factors
Aspergillomas are broadly divided into:
Secondary aspergilloma (common) - colonization of a pre-existing cavity:
- Tuberculosis is the most common predisposing condition globally. Aspergilloma occurs in 11-17% of post-TB cavities; 20% of patients recovering from cavitary TB develop it within 3 years. In developing countries, TB accounts for >90% of cases.
- Sarcoidosis
- Histoplasmosis, blastomycosis
- Bronchiectasis, pulmonary fibrosis, asbestosis
- Lung abscess, pneumonia
- Pulmonary cysts
- Ankylosing spondylitis
- AIDS (especially atypical Pneumocystis jirovecii pneumonia)
- Pulmonary infarction, adenocarcinoma, rheumatoid nodules
Primary aspergilloma (rare) - Aspergillus itself initiates cavity formation via:
- Invasive Pulmonary Aspergillosis (IPA) with neutrophil recovery
- Chronic Necrotizing Pulmonary Aspergillosis (CNPA)
- ABPA causing bronchiectasis with distal fungal growth (aspergillomas found in ~7% of ABPA patients)
Note: A. niger is particularly implicated in diabetic patients; it produces oxalic acid crystals visible in sputum.
- Fishman's, p. 2329
Pathophysiology
The fungus proliferates within the cavity as a biofilm. Typical biofilm structures have been demonstrated in aspergillomas both in human specimens and in murine IPA models. The biofilm architecture critically limits penetration by antifungal agents, making medical treatment difficult.
The fungal mass is held within the cavity by gravity and moves with positional change - this forms the basis of the classical radiological sign. The cavity wall develops hypertrophic bronchial arteries, which are the source of hemoptysis.
Spontaneous resolution occurs in 7-10% of cases, often associated with bacterial superinfection of the cavity. Aspergillomas only rarely increase in size.
- Fishman's, p. 2329
Clinical Features
| Feature | Detail |
|---|---|
| Hemoptysis | Most characteristic; present in 50-90% of patients. Usually mild and recurrent but can be massive and life-threatening |
| Cough | Common, productive |
| Dyspnea | Reflects underlying lung disease |
| Weight loss, fatigue | Constitutional features |
| Chest pain | Pleuritic if pleural involvement |
| Fever | Usually absent unless secondary infection |
| Asymptomatic | A significant proportion discovered incidentally |
Hemoptysis is the dominant clinical concern. It results from mechanical friction of the fungal ball against the cavity wall eroding hypertrophic bronchial arteries, release of mycotoxins and proteolytic enzymes, and endotoxin-mediated vascular injury.
Diagnosis
1. Radiology
Chest X-ray: A solid, rounded mass (3-5 cm diameter) within a cavity, partially surrounded by a crescent of air - the Monod's sign (air-crescent sign). Marked pleural thickening is often present.
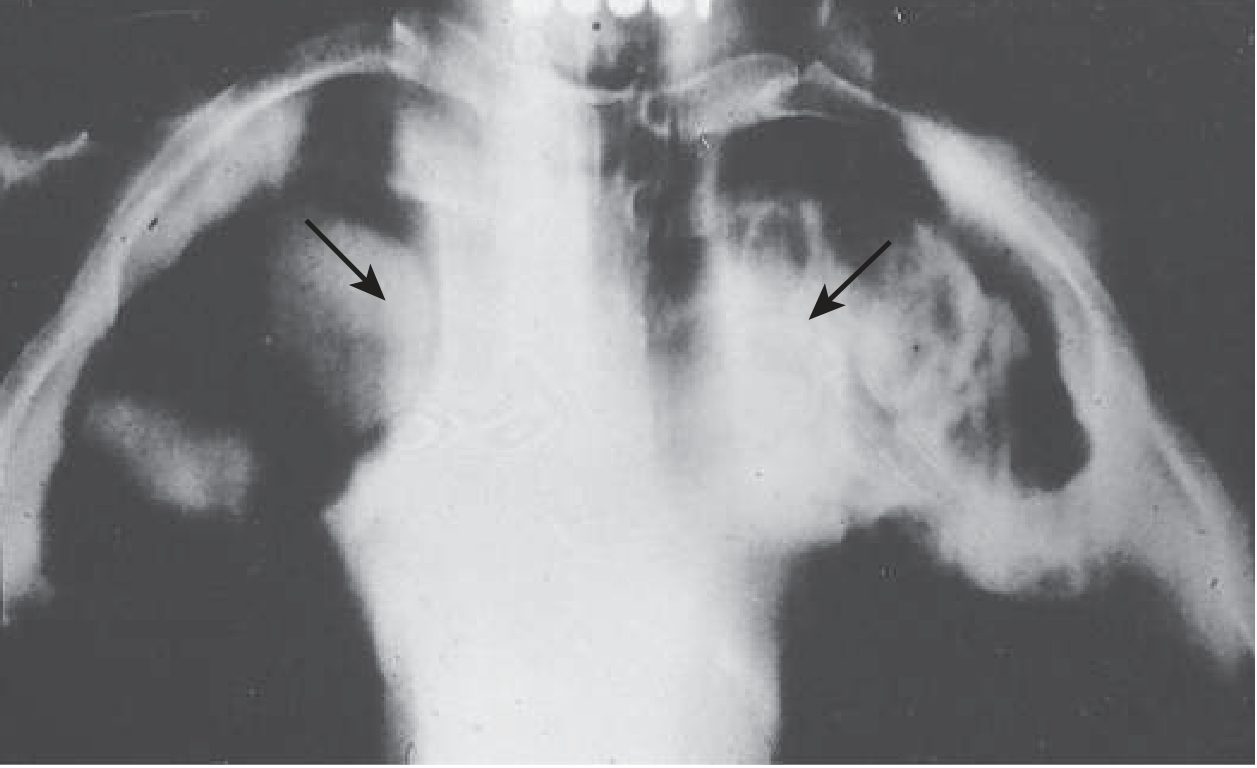
Chest radiograph showing bilateral apical aspergillomas with the air-crescent (Monod's) sign (arrows). Goldman-Cecil Medicine.
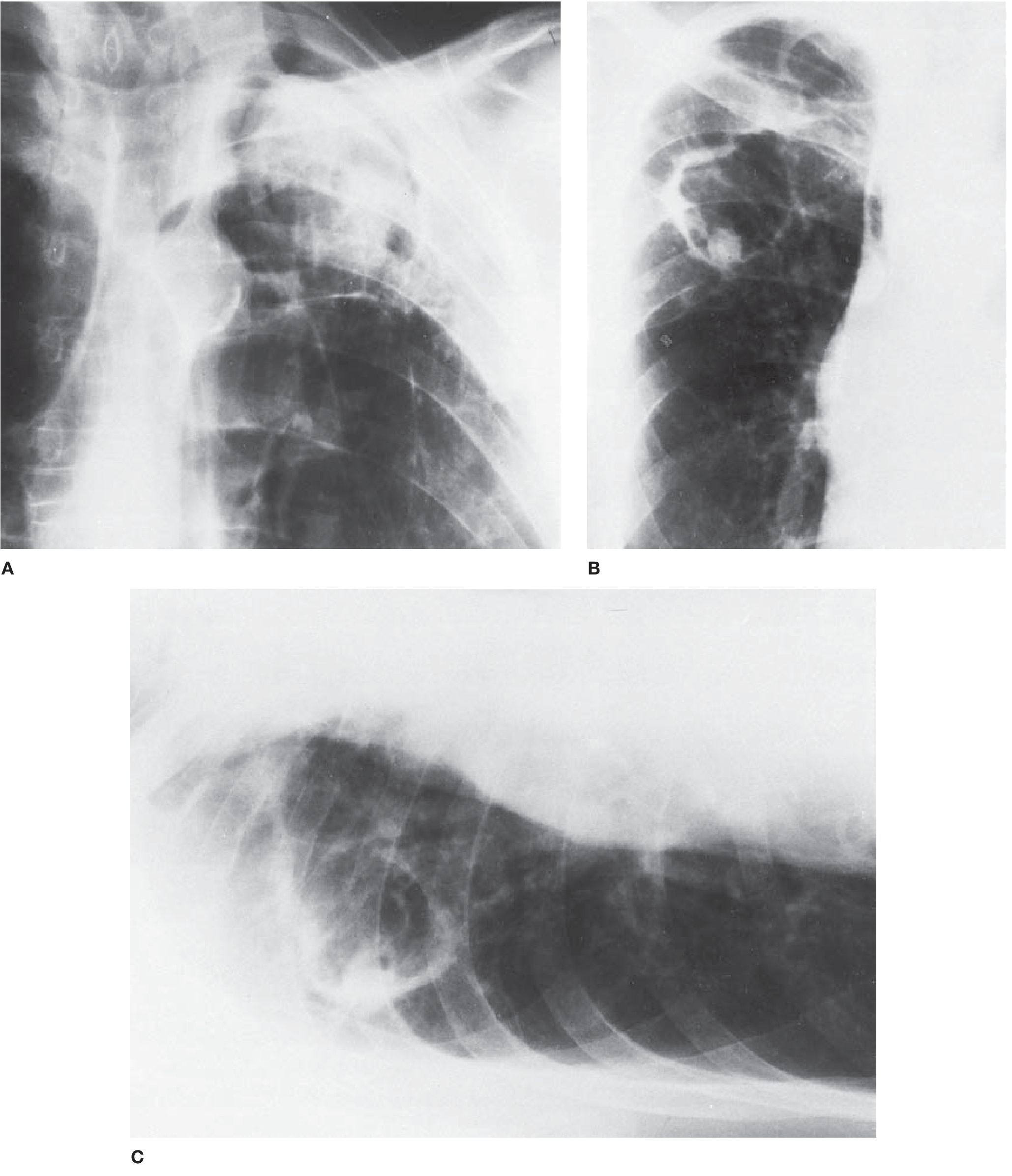
Fig. A: Post-TB aspergilloma with classic Monod's sign and pleural thickening. B: Thin-walled cavity aspergilloma in ankylosing spondylitis. C: Decubitus film demonstrating mobility of the fungus ball (positional change). - Fishman's Pulmonary Diseases
Key radiological points:
- Upper lung field predominance (reflecting TB cavity distribution)
- Lesion moves in decubitus position (mobile fungus ball)
- CT scan confirms features not apparent on X-ray; globules of gas visible within the hyphal mass; CT angiography identifies hypertrophic bronchial arteries supplying the cystic wall - important for planning bronchial artery embolization (BAE)
2. Microbiology
- Sputum culture positive for Aspergillus in >50% of patients but lacks sensitivity and specificity
- BAL culture may be used in atypical cases
3. Serology (most important diagnostic test)
- Precipitating antibodies (precipitins/IgG) to Aspergillus antigens: present in >95% of patients with aspergilloma - the most reliable diagnostic marker
- Patients on corticosteroids may be seronegative
- Eosinophilia and elevated IgE suggest allergy but are inconsistent
4. Histopathology / Biopsy
- May be needed in atypical cases
- Shows septate hyphae with characteristic 45-degree angle branching
Poor Prognostic Indicators
- Progressive increase in size or number of aspergillomas
- Severe underlying lung disease with poor lung reserve
- Immunosuppressive therapy or AIDS
- Sarcoidosis as the predisposing condition
- Rising Aspergillus-specific IgG titer
- Repeated episodes of severe hemoptysis
Treatment
There is no consensus on treatment due to lack of controlled studies. Management must be individualized based on the severity of symptoms, underlying lung reserve, and operative fitness.
1. Conservative Management
- Asymptomatic patients: careful observation with periodic chest X-rays, without specific medical or surgical intervention.
2. Control of Hemoptysis
Bronchial Artery Embolization (BAE):
- First-line emergency measure for acute massive hemoptysis
- Temporary control in most cases; recurrence is common
- CT angiography helps identify the culprit bronchial arteries
Intracavitary instillation of antifungal agents:
- CT-guided percutaneous instillation of Amphotericin B (AMB-D) - effective for massive hemoptysis in poor surgical candidates
- Resolution of hemoptysis has been documented in several cases
Radiation therapy:
- Shown to be effective even in massive hemoptysis
- Recommended for recurrence of life-threatening hemoptysis after BAE
3. Medical (Antifungal) Therapy
- Itraconazole (oral, 200-400 mg/day): The most studied antifungal for aspergilloma. Non-controlled studies show variable efficacy; capsule formulation used in several series. Limited penetration due to biofilm is the main drawback.
- Voriconazole: Used for CPA; data for simple aspergilloma less robust
- Overall, systemic antifungals are used, particularly in non-surgical candidates, but response rates are modest
4. Surgical Treatment
Surgical resection is the definitive treatment but carries significant morbidity:
- Indications: Life-threatening hemoptysis, progressive increase in size, failure of conservative management
- Procedure: Lobectomy is the standard; pneumonectomy rarely required
- Complications: Bronchopleural fistula, pleural Aspergillus infection, prolonged air leak - limiting its use
- Cavernostomy (under local anesthesia) is an alternative for unfit patients; should be a last resort due to associated mortality and mediocre results
| Approach | Indication |
|---|---|
| Observation | Asymptomatic, small, stable |
| BAE | Acute massive hemoptysis |
| Intracavitary AMB | Poor surgical candidate, hemoptysis |
| Itraconazole | Non-surgical management |
| Surgery (lobectomy) | Life-threatening hemoptysis, progressive disease |
| Cavernostomy | Last resort in surgical high-risk |
Complications
- Massive / fatal hemoptysis - the main cause of death
- Pleural aspergillosis - may complicate surgical resection or develop via bronchopleural fistula
- Pneumothorax - rare, reported in hematologic malignancies
- Secondary bacterial infection of the cavity
- ABPA perpetuation - aspergilloma may sustain the allergic cycle in ABPA
Key Exam Points (Summary Table)
| Feature | Key Fact |
|---|---|
| Causative organism | Aspergillus fumigatus (most common); A. niger in diabetics |
| Commonest predisposing cause | Post-tubercular cavity |
| Pathology | Fungus ball in pre-existing cavity; biofilm structure |
| Classic symptom | Hemoptysis (50-90%) |
| Classic X-ray sign | Monod's sign / air crescent sign |
| Best serological test | Precipitins (IgG) to Aspergillus - positive in >95% |
| Spontaneous resolution | 7-10% of cases |
| Treatment of massive hemoptysis | Bronchial artery embolization (BAE) |
| Definitive treatment | Surgical resection (lobectomy) |
| Oral antifungal of choice | Itraconazole |
| Classification | Form of Chronic Pulmonary Aspergillosis (CPA) |
Sources: Fishman's Pulmonary Diseases and Disorders (pp. 2329-2330); Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E; Murray & Nadel's Textbook of Respiratory Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.