Steps in small incision cataract surgery
manual small incision cataract surgery MSICS steps scleral tunnel nucleus expression
Manual Small-Incision Cataract Surgery (MSICS)
Step 1 — Patient Preparation & Anaesthesia
- Topical, peribulbar, or sub-Tenon's anaesthesia is administered.
- The eye is cleaned and draped; a lid speculum is inserted.
- Pupil is maximally dilated with mydriatic drops.
Step 2 — Conjunctival Flap
- A fornix-based conjunctival flap is created at the superior limbus, exposing the bare sclera.
- Wet-field cautery is applied to achieve haemostasis.
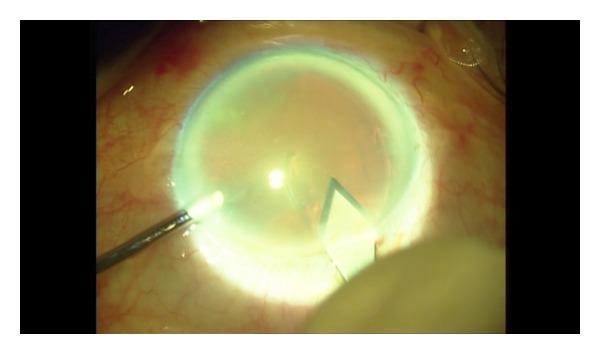
Step 3 — Scleral Groove (Incision)
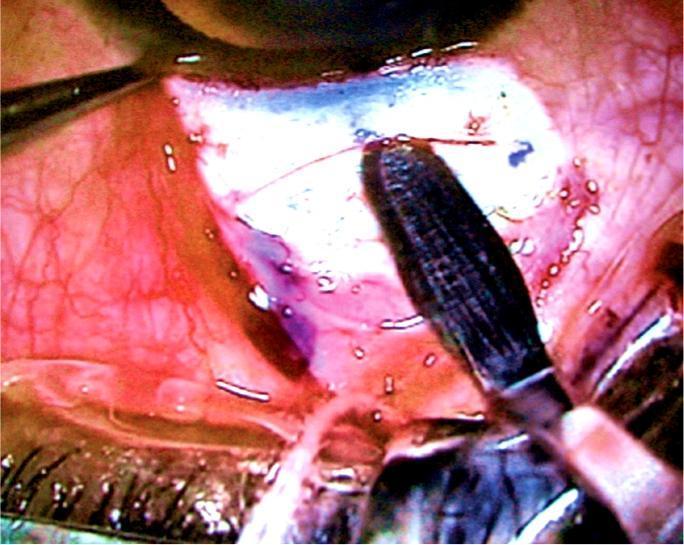
- A partial-thickness (approximately 300 µm deep) frown-shaped or straight scleral groove is made ~1–2 mm behind the limbus using a crescent blade.
- The groove spans ~6–7 mm — wide enough to allow nucleus delivery without phacoemulsification.
Step 4 — Sclero-Corneal Tunnel Dissection
- A crescent blade dissects a lamellar tunnel forward into clear cornea, creating a self-sealing sclerocorneal tunnel.
- The tunnel must be of uniform depth — too shallow risks button-holing; too deep risks perforation.
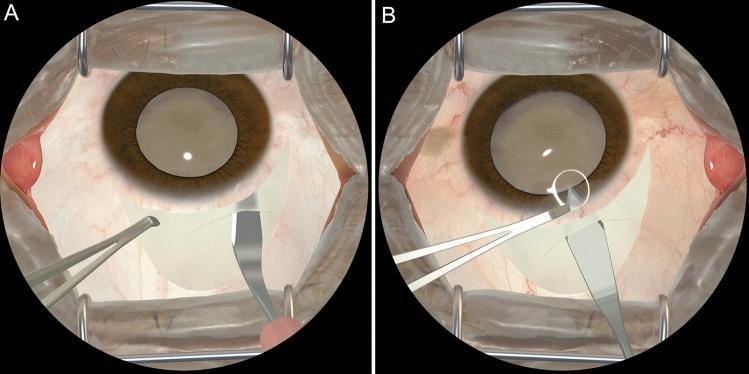
- A keratome then enters the anterior chamber through the internal lip of the tunnel.
Step 5 — Anterior Capsulotomy (Capsulorhexis)
- Trypan blue (0.06%) is injected to stain the anterior capsule, aiding visibility — especially important with white/mature cataracts.
- An ophthalmic viscosurgical device (OVD/viscoelastic) fills the anterior chamber to maintain depth.
- A continuous curvilinear capsulorhexis (CCC) is performed using a needle or capsulorhexis forceps, creating a circular opening in the anterior capsule.
Step 6 — Hydrodissection & Hydrodelineation
- Balanced salt solution (BSS) is injected under the anterior capsule to free the lens nucleus from its cortical attachments (hydrodissection) and to delineate the nucleus from the epinucleus (hydrodelineation).
- This allows free rotation and subsequent delivery of the nucleus.
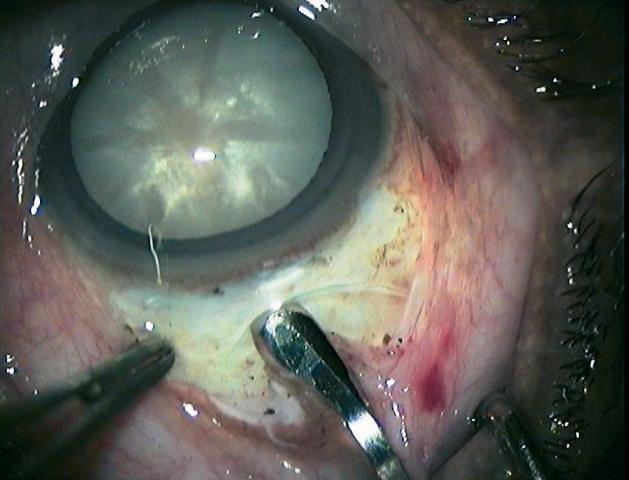
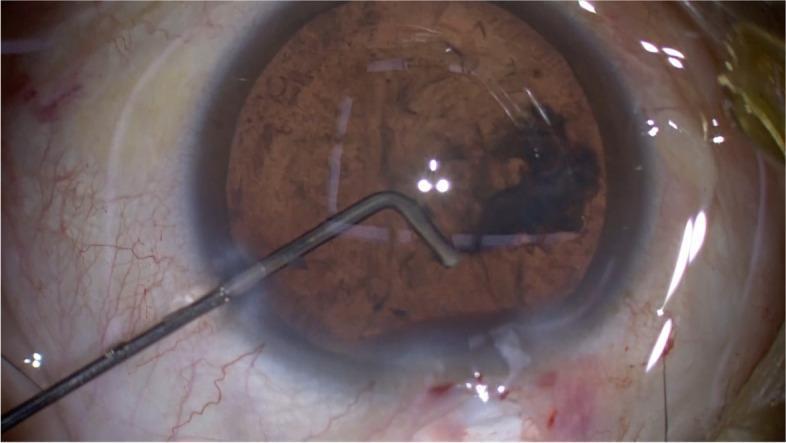
Step 7 — Nucleus Prolapse & Expression
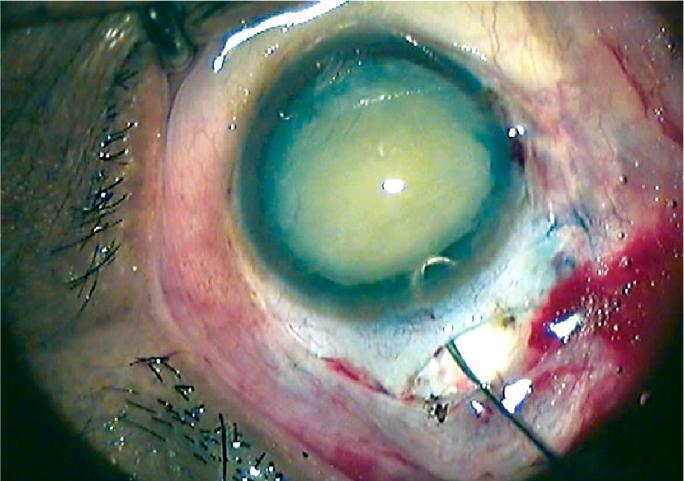
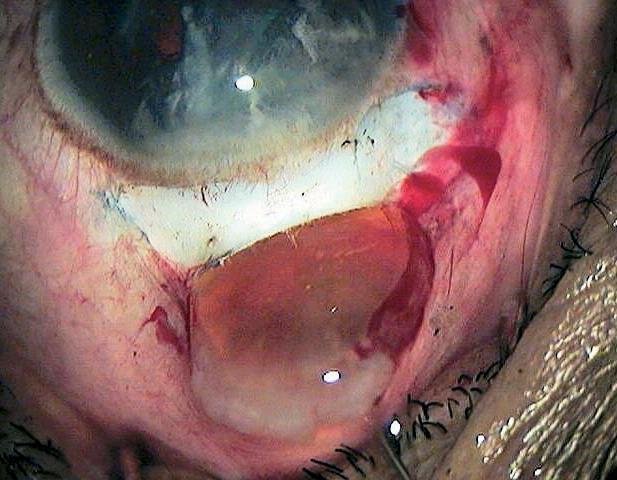
- The nucleus is tilted and prolapsed into the anterior chamber using instruments (e.g., Sinskey hook, lens dialer, or a vectis).
- A lens vectis (wire loop) or an irrigating vectis is inserted beneath the nucleus in the anterior chamber.
- The nucleus is manually expressed out through the scleral tunnel by gentle posterior pressure at the limbus combined with upward lift of the vectis — the "sandwich" or "tumbling" technique.
- OVD protects the corneal endothelium throughout this step.
Step 8 — Cortical Aspiration
- Residual cortex is removed using a Simcoe cannula (two-way irrigation-aspiration cannula).
- Irrigation maintains anterior chamber depth while aspiration removes lens remnants from the capsular bag.
- Thorough cortex removal prevents posterior capsule opacification (PCO).
Step 9 — IOL Implantation
- The capsular bag is refilled with OVD.
- A posterior chamber intraocular lens (PCIOL) — typically a rigid PMMA lens — is implanted into the capsular bag.
- PMMA lenses are used because they can be delivered through the larger (6–7 mm) MSICS tunnel without folding; foldable IOLs can also be used.
Step 10 — OVD Removal & Wound Closure
- OVD is thoroughly irrigated and aspirated from the anterior chamber.
- The anterior chamber is reformed with BSS.
- The self-sealing tunnel architecture usually makes suturing unnecessary; however, a 10-0 nylon suture may be placed if the wound is not watertight.
- The conjunctival flap is repositioned and secured (often with cautery or a single suture).
Step 11 — Postoperative
- Subconjunctival antibiotic/steroid injection or topical drops instilled.
- Eye pad and shield applied.
Key Advantages of MSICS vs. Conventional ECCE vs. Phacoemulsification
| Feature | ECCE | MSICS | Phaco |
|---|---|---|---|
| Incision size | 8–10 mm | 6–7 mm (self-sealing) | 2–3 mm |
| Sutures required | Yes | Usually no | No |
| Nucleus handling | Expression | Manual expression via tunnel | Ultrasonic fragmentation |
| Cost/equipment | Low | Low | High |
| Astigmatism induced | High | Low–moderate | Minimal |
| Dense cataracts | Suitable | Ideal | Challenging |
Photos of haemostasis in MSICS
haemostasis cautery MSICS manual small incision cataract surgery scleral bleeding
wet field cautery bipolar cautery ophthalmic surgery conjunctival bleeding
1. Bipolar diathermy forceps applied to conjunctival vessels
2. General vs. modified scleral incision — haemostasis comparison
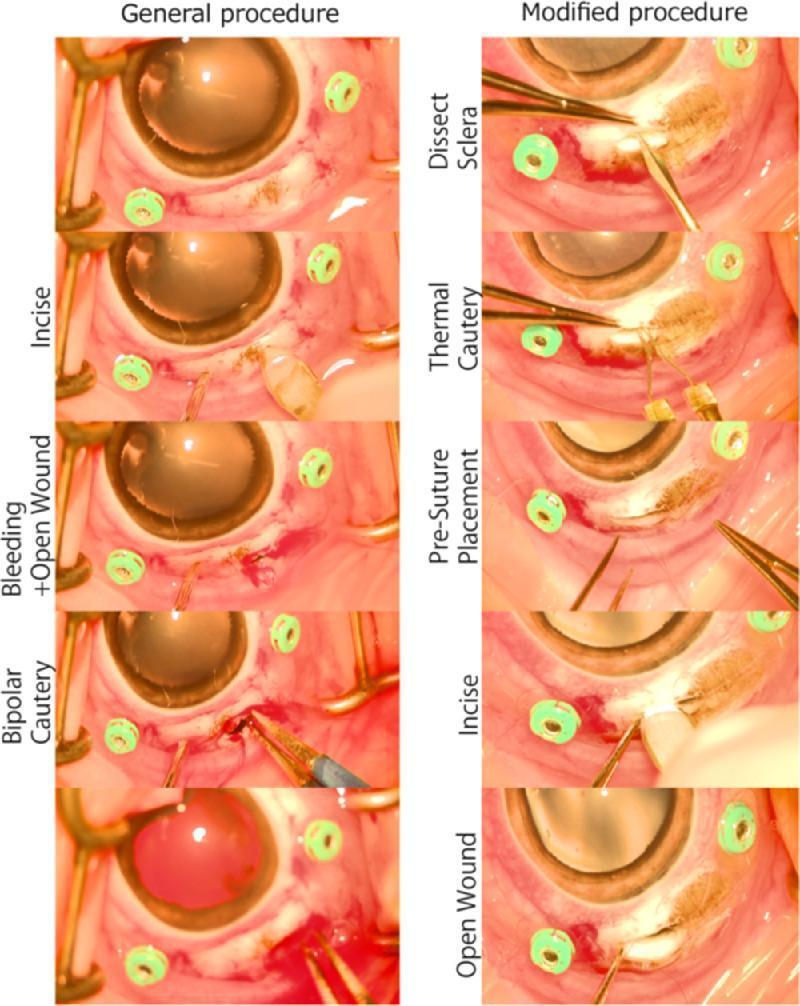
- Left column (general): Sclera is incised first → bleeding occurs → bipolar cautery is applied reactively to the bleeding wound.
- Right column (modified/preferred): Sclera is partially dissected → thermal cautery is applied prophylactically to the exposed bed → pre-suture is placed → full-thickness incision is then made → the open wound is nearly bloodless.
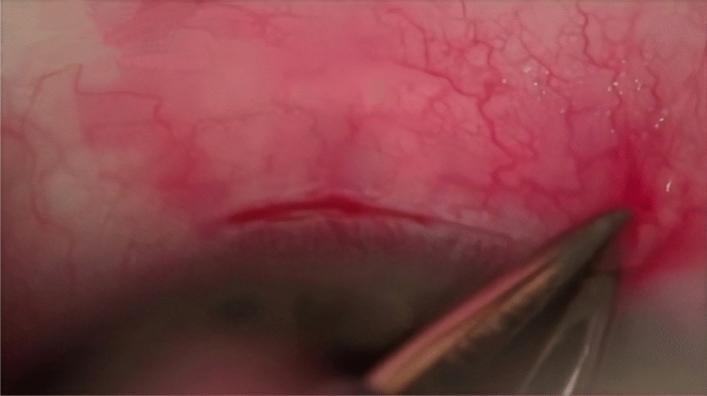
3. Exposed sclera after conjunctival flap — pre-haemostasis field
Clinical notes on haemostasis in MSICS
| Method | Use |
|---|---|
| Wet-field (bipolar) cautery | Primary tool; applied to episcleral bleeders after conjunctival flap reflection |
| Monopolar/thermal cautery | Used in some settings; applied to the scleral bed before the groove |
| Direct pressure | Gentle tamponade with a sponge while preparing instruments |
| Adrenaline-soaked sponge | Occasionally used on episcleral vessels to induce vasoconstriction |
Make this into aa ppt
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_39fd2c06d07d8a35e399e887d6b117e45796d7c548ae79cb50e227f8d1f107c6.jpg" \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_e786ca87c47a91e47c81ca4905dfe83e85ef1ea39135e082775fec07d450f248.jpg" \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_217dfc19f8ad0dff37f579527bb2599ad43535590fa51c05efe7abbc4256e480.jpg" \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_ef37296fbd9b17f557d1fcb0cb3dfd3422da9c96bbf03b5af62361ebef8017ee.jpg" \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_d869b7a97961e9261fecaf818ef925efb95a6228836b24d3ba5615693fc5dcac.jpg" \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_86899785e985375b9e09010dabc3717f7e737921b06d9bb77e54fb7f3f00a6db.jpg" \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_b814788b80435b88497e1f8d3cfa94f633c8239e386da3dc4d4910b1a87e87cf.jpg" \ 2>/dev/null | node -e "const d=require('fs').readFileSync('/dev/stdin','utf8'); const arr=JSON.parse(d); arr.forEach((x,i)=>{ if(x.error) console.log(i,'ERROR',x.error); else console.log(i,'OK len=',x.base64.length); });"
mkdir -p /home/daytona/workspace/msics-ppt
~/msics-ppt/build.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// ── Fetch all images ──────────────────────────────────────────────────────────
const urls = [
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_39fd2c06d07d8a35e399e887d6b117e45796d7c548ae79cb50e227f8d1f107c6.jpg", // 0: scleral tunnel VR diagram
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_e786ca87c47a91e47c81ca4905dfe83e85ef1ea39135e082775fec07d450f248.jpg", // 1: frown incision crescent blade
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_217dfc19f8ad0dff37f579527bb2599ad43535590fa51c05efe7abbc4256e480.jpg", // 2: nucleus delivery
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_ef37296fbd9b17f557d1fcb0cb3dfd3422da9c96bbf03b5af62361ebef8017ee.jpg", // 3: fish-hook nucleus
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_d869b7a97961e9261fecaf818ef925efb95a6228836b24d3ba5615693fc5dcac.jpg", // 4: bipolar diathermy conjunctiva
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_86899785e985375b9e09010dabc3717f7e737921b06d9bb77e54fb7f3f00a6db.jpg", // 5: haemostasis general vs modified
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_b814788b80435b88497e1f8d3cfa94f633c8239e386da3dc4d4910b1a87e87cf.jpg", // 6: exposed sclera pre-haemostasis
];
const raw = execSync(
`node /home/daytona/skills/shared/scripts/fetch_images.js ${urls.map(u => `"${u}"`).join(" ")}`
).toString();
const imgs = JSON.parse(raw);
// ── Colour palette ────────────────────────────────────────────────────────────
// Deep navy dominant, teal accent, white text, amber highlight
const C = {
navy: "0D1B2A",
navyMid: "1A2E42",
teal: "1E8A8A",
tealLt: "2ABFBF",
amber: "E8A030",
white: "FFFFFF",
offWhite:"E8EDF2",
muted: "8FA8BF",
};
// ── Helper: slide header bar ──────────────────────────────────────────────────
function addHeader(slide, title, stepLabel) {
// Full-width navy background
slide.addShape("rect", { x: 0, y: 0, w: 10, h: 1.05, fill: { color: C.navy }, line: { color: C.navy } });
// Teal left accent stripe
slide.addShape("rect", { x: 0, y: 0, w: 0.08, h: 1.05, fill: { color: C.teal }, line: { color: C.teal } });
if (stepLabel) {
slide.addText(stepLabel, {
x: 0.18, y: 0.08, w: 1.4, h: 0.38,
fontSize: 9, bold: true, color: C.amber, fontFace: "Calibri", margin: 0,
});
}
slide.addText(title, {
x: 0.18, y: stepLabel ? 0.42 : 0.22, w: 9.6, h: 0.55,
fontSize: stepLabel ? 20 : 24, bold: true, color: C.white, fontFace: "Calibri", margin: 0,
});
}
// ── Helper: footer ────────────────────────────────────────────────────────────
function addFooter(slide, text) {
slide.addShape("rect", { x: 0, y: 5.32, w: 10, h: 0.3, fill: { color: C.navyMid }, line: { color: C.navyMid } });
slide.addText(text, {
x: 0.2, y: 5.33, w: 9.6, h: 0.25,
fontSize: 7.5, color: C.muted, fontFace: "Calibri", margin: 0,
});
}
// ── Helper: info card (dark rounded rect) ─────────────────────────────────────
function addCard(slide, x, y, w, h, color) {
slide.addShape("roundRect", {
x, y, w, h,
fill: { color: color || C.navyMid },
line: { color: C.teal, pt: 1 },
rectRadius: 0.08,
});
}
// ── Helper: step number badge ─────────────────────────────────────────────────
function addBadge(slide, num, x, y) {
slide.addShape("ellipse", { x, y, w: 0.42, h: 0.42, fill: { color: C.teal }, line: { color: C.teal } });
slide.addText(String(num), {
x, y, w: 0.42, h: 0.42,
fontSize: 14, bold: true, color: C.white, fontFace: "Calibri",
align: "center", valign: "middle", margin: 0,
});
}
// ─────────────────────────────────────────────────────────────────────────────
let pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Manual Small-Incision Cataract Surgery (MSICS)";
pres.author = "Orris Medical";
// ══════════════════════════════════════════════════════════════════
// SLIDE 1 — Title slide
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
s.addShape("rect", { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: C.teal }, line: { color: C.teal } });
s.addShape("rect", { x: 0, y: 4.5, w: 10, h: 1.125, fill: { color: C.navyMid }, line: { color: C.navyMid } });
s.addText("Manual Small-Incision", {
x: 0.5, y: 1.0, w: 9, h: 0.9,
fontSize: 38, bold: true, color: C.white, fontFace: "Calibri",
align: "center", charSpacing: 1,
});
s.addText("Cataract Surgery", {
x: 0.5, y: 1.85, w: 9, h: 0.9,
fontSize: 38, bold: true, color: C.tealLt, fontFace: "Calibri",
align: "center", charSpacing: 1,
});
s.addText("(MSICS)", {
x: 0.5, y: 2.65, w: 9, h: 0.5,
fontSize: 22, color: C.amber, fontFace: "Calibri", align: "center", bold: false,
});
s.addText("Step-by-Step Surgical Technique", {
x: 0.5, y: 3.2, w: 9, h: 0.4,
fontSize: 14, color: C.offWhite, fontFace: "Calibri", align: "center", italic: true,
});
s.addText("Source: Kanski's Clinical Ophthalmology, 10th ed.", {
x: 0.5, y: 4.6, w: 9, h: 0.25,
fontSize: 9, color: C.muted, fontFace: "Calibri", align: "center",
});
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 2 — What is MSICS?
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
addHeader(s, "What is MSICS?");
const points = [
["Variant of ECCE", "Manual small-incision cataract surgery is a refined form of extracapsular cataract extraction (ECCE)."],
["Self-sealing tunnel", "Creates a 6–7 mm sclero-corneal tunnel — no sutures typically needed."],
["High-volume settings", "Designed for resource-limited environments; faster and cheaper than phacoemulsification."],
["Ideal for dense cataracts", "Particularly suited for mature, brunescent, and white cataracts."],
["Comparable outcomes", "Visual rehabilitation equivalent to phacoemulsification."],
];
points.forEach(([title, body], i) => {
const y = 1.2 + i * 0.82;
addBadge(s, i + 1, 0.2, y + 0.06);
addCard(s, 0.72, y, 9.1, 0.68);
s.addText(title, { x: 0.85, y: y + 0.04, w: 2.2, h: 0.28, fontSize: 11, bold: true, color: C.amber, fontFace: "Calibri", margin: 0 });
s.addText(body, { x: 0.85, y: y + 0.3, w: 8.7, h: 0.32, fontSize: 10, color: C.offWhite, fontFace: "Calibri", margin: 0 });
});
addFooter(s, "Kanski's Clinical Ophthalmology, 10th ed.");
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 3 — Steps overview (flow)
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
addHeader(s, "Surgical Steps — Overview");
const steps = [
"Patient Prep & Anaesthesia",
"Conjunctival Flap",
"Haemostasis",
"Scleral Groove",
"Tunnel Dissection",
"Capsulotomy",
"Hydrodissection",
"Nucleus Expression",
"Cortical Aspiration",
"IOL Implantation",
"Wound Closure",
];
// Two columns
const col1 = steps.slice(0, 6);
const col2 = steps.slice(6);
col1.forEach((step, i) => {
const y = 1.18 + i * 0.68;
addBadge(s, i + 1, 0.18, y);
s.addText(step, { x: 0.68, y: y + 0.04, w: 4.3, h: 0.35, fontSize: 11.5, color: C.offWhite, fontFace: "Calibri", bold: i === 2, margin: 0 });
if (i === 2) {
s.addShape("rect", { x: 0.68, y: y + 0.39, w: 4.3, h: 0.02, fill: { color: C.teal }, line: { color: C.teal } });
}
});
col2.forEach((step, i) => {
const y = 1.18 + i * 0.68;
addBadge(s, i + 7, 5.2, y);
s.addText(step, { x: 5.7, y: y + 0.04, w: 4.1, h: 0.35, fontSize: 11.5, color: C.offWhite, fontFace: "Calibri", margin: 0 });
});
// Vertical divider
s.addShape("rect", { x: 4.98, y: 1.15, w: 0.04, h: 4.1, fill: { color: C.teal }, line: { color: C.teal } });
addFooter(s, "Step 3 (Haemostasis) is expanded in detail in subsequent slides.");
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 4 — Steps 1 & 2: Prep + Conjunctival Flap
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
addHeader(s, "Patient Preparation & Conjunctival Flap", "STEPS 1–2");
// Step 1 card
addCard(s, 0.2, 1.2, 4.55, 3.9);
addBadge(s, 1, 0.28, 1.28);
s.addText("Patient Preparation & Anaesthesia", { x: 0.78, y: 1.28, w: 3.8, h: 0.38, fontSize: 12, bold: true, color: C.amber, fontFace: "Calibri", margin: 0 });
s.addText([
{ text: "• Topical, peribulbar, or sub-Tenon's anaesthesia", options: { breakLine: true } },
{ text: "• Lid speculum inserted; eye cleaned and draped", options: { breakLine: true } },
{ text: "• Pupil fully dilated with mydriatic drops", options: { breakLine: true } },
{ text: "• Informed consent; biometry completed pre-op", options: { breakLine: true } },
{ text: "• Penicillin allergy status; antibiotic drops started", options: {} },
], { x: 0.35, y: 1.75, w: 4.2, h: 2.6, fontSize: 10.5, color: C.offWhite, fontFace: "Calibri" });
// Step 2 card
addCard(s, 5.1, 1.2, 4.65, 3.9);
addBadge(s, 2, 5.18, 1.28);
s.addText("Conjunctival Flap", { x: 5.68, y: 1.28, w: 3.9, h: 0.38, fontSize: 12, bold: true, color: C.amber, fontFace: "Calibri", margin: 0 });
s.addText([
{ text: "• Fornix-based conjunctival flap raised superiorly", options: { breakLine: true } },
{ text: "• Tenon's capsule dissected to expose bare sclera", options: { breakLine: true } },
{ text: "• Bridle suture (4-0 silk) placed through superior rectus for globe control", options: { breakLine: true } },
{ text: "• Exposes the limbal zone for scleral incision", options: { breakLine: true } },
{ text: "• Haemostasis achieved with wet-field cautery (Step 3)", options: {} },
], { x: 5.25, y: 1.75, w: 4.3, h: 2.6, fontSize: 10.5, color: C.offWhite, fontFace: "Calibri" });
addFooter(s, "Kanski's Clinical Ophthalmology, 10th ed.");
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 5 — Step 3: Haemostasis (with images)
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
addHeader(s, "Haemostasis", "STEP 3");
// Left: text
addCard(s, 0.2, 1.15, 3.95, 4.15);
s.addText([
{ text: "Wet-field bipolar cautery applied to episcleral vessels after conjunctival flap is raised.", options: { breakLine: true } },
{ text: " ", options: { breakLine: true } },
{ text: "Why it matters:", options: { bold: true, color: C.amber, breakLine: true } },
{ text: "• Bleeding into AC during nucleus expression → expulsive haemorrhage risk", options: { breakLine: true } },
{ text: "• Blood-stained field reduces visibility for subsequent steps", options: { breakLine: true } },
{ text: " ", options: { breakLine: true } },
{ text: "Methods:", options: { bold: true, color: C.amber, breakLine: true } },
{ text: "• Wet-field (bipolar) cautery — primary tool", options: { breakLine: true } },
{ text: "• Prophylactic thermal cautery to scleral bed", options: { breakLine: true } },
{ text: "• Adrenaline-soaked sponge (vasoconstriction)", options: { breakLine: true } },
{ text: "• Direct pressure with dry sponge", options: {} },
], { x: 0.32, y: 1.25, w: 3.65, h: 3.9, fontSize: 9.5, color: C.offWhite, fontFace: "Calibri" });
// Centre: bipolar cautery image
if (!imgs[4].error) {
s.addImage({ data: imgs[4].base64, x: 4.28, y: 1.18, w: 2.55, h: 2.0 });
s.addText("Bipolar diathermy forceps\ncoagulating conjunctival vessels", {
x: 4.28, y: 3.22, w: 2.55, h: 0.45, fontSize: 7.5, color: C.muted, fontFace: "Calibri", align: "center",
});
}
// Right: general vs modified haemostasis
if (!imgs[5].error) {
s.addImage({ data: imgs[5].base64, x: 6.98, y: 1.18, w: 2.82, h: 3.7 });
s.addText("General vs. modified procedure:\nprophylactic cautery reduces intraoperative bleeding", {
x: 6.98, y: 4.92, w: 2.82, h: 0.45, fontSize: 7.5, color: C.muted, fontFace: "Calibri", align: "center",
});
}
addFooter(s, "Adequate haemostasis before the scleral groove is mandatory for a clear surgical field.");
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 6 — Step 3b: Pre-haemostasis field (exposed sclera)
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
addHeader(s, "Exposed Sclera — Before Haemostasis", "STEP 3 — CLINICAL VIEW");
if (!imgs[6].error) {
s.addImage({ data: imgs[6].base64, x: 0.3, y: 1.2, w: 5.5, h: 3.85 });
}
addCard(s, 6.0, 1.2, 3.75, 3.85);
s.addText("What this image shows:", { x: 6.15, y: 1.3, w: 3.45, h: 0.35, fontSize: 11, bold: true, color: C.amber, fontFace: "Calibri", margin: 0 });
s.addText([
{ text: "• Conjunctival flap reflected, bare sclera exposed", options: { breakLine: true } },
{ text: "• Perilimbal vascularity clearly visible", options: { breakLine: true } },
{ text: "• Focal bleeding points present — cautery not yet applied", options: { breakLine: true } },
{ text: "• Toothed forceps stabilising the globe", options: { breakLine: true } },
{ text: "• Mature white cataract visible through dilated pupil", options: { breakLine: true } },
{ text: " ", options: { breakLine: true } },
{ text: "Key point:", options: { bold: true, color: C.tealLt, breakLine: true } },
{ text: "Cautery must be applied NOW — before the scleral groove is made — to achieve a dry, clear field for tunnel dissection.", options: {} },
], { x: 6.15, y: 1.72, w: 3.45, h: 3.1, fontSize: 9.5, color: C.offWhite, fontFace: "Calibri" });
addFooter(s, "Intraoperative photo — exposed bare sclera with perilimbal bleeding points before cautery.");
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 7 — Steps 4–5: Scleral Groove + Tunnel
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
addHeader(s, "Scleral Groove & Tunnel Dissection", "STEPS 4–5");
// Image: frown incision
if (!imgs[1].error) {
s.addImage({ data: imgs[1].base64, x: 0.2, y: 1.18, w: 4.6, h: 3.5 });
s.addText("Frown incision: crescent blade creating sclerocorneal tunnel;\nTrypan Blue highlights tunnel path", {
x: 0.2, y: 4.72, w: 4.6, h: 0.45, fontSize: 7.5, color: C.muted, fontFace: "Calibri", align: "center",
});
}
// Right: text
addCard(s, 5.0, 1.18, 4.8, 2.0);
addBadge(s, 4, 5.08, 1.26);
s.addText("Scleral Groove", { x: 5.6, y: 1.26, w: 4.0, h: 0.35, fontSize: 11.5, bold: true, color: C.amber, fontFace: "Calibri", margin: 0 });
s.addText([
{ text: "• Partial-thickness (~300 µm) frown or straight groove", options: { breakLine: true } },
{ text: "• 6–7 mm wide, 1–2 mm behind limbus", options: { breakLine: true } },
{ text: "• Made with a #15 blade or crescent knife", options: {} },
], { x: 5.15, y: 1.65, w: 4.5, h: 1.35, fontSize: 10, color: C.offWhite, fontFace: "Calibri" });
addCard(s, 5.0, 3.3, 4.8, 2.0);
addBadge(s, 5, 5.08, 3.38);
s.addText("Tunnel Dissection", { x: 5.6, y: 3.38, w: 4.0, h: 0.35, fontSize: 11.5, bold: true, color: C.amber, fontFace: "Calibri", margin: 0 });
s.addText([
{ text: "• Crescent blade dissects lamellar tunnel forward into clear cornea", options: { breakLine: true } },
{ text: "• Uniform depth essential — too shallow risks button-hole; too deep risks perforation", options: { breakLine: true } },
{ text: "• Keratome enters anterior chamber through internal lip", options: {} },
], { x: 5.15, y: 3.77, w: 4.5, h: 1.35, fontSize: 10, color: C.offWhite, fontFace: "Calibri" });
addFooter(s, "The self-sealing architecture of the tunnel is the key innovation of MSICS over conventional ECCE.");
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 8 — Steps 6 & 7: Capsulorhexis + Hydrodissection (VR image)
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
addHeader(s, "Capsulotomy & Hydrodissection", "STEPS 6–7");
// VR simulator image (tunnel creation)
if (!imgs[0].error) {
s.addImage({ data: imgs[0].base64, x: 0.2, y: 1.18, w: 4.6, h: 2.9 });
s.addText("Keratome entry into anterior chamber (VR simulator view):\nA — tunnel dissection; B — AC entry with keratome", {
x: 0.2, y: 4.12, w: 4.6, h: 0.45, fontSize: 7.5, color: C.muted, fontFace: "Calibri", align: "center",
});
}
addCard(s, 5.0, 1.18, 4.8, 2.05);
addBadge(s, 6, 5.08, 1.26);
s.addText("Anterior Capsulotomy (CCC)", { x: 5.6, y: 1.26, w: 4.0, h: 0.35, fontSize: 11.5, bold: true, color: C.amber, fontFace: "Calibri", margin: 0 });
s.addText([
{ text: "• Trypan blue 0.06% stains anterior capsule", options: { breakLine: true } },
{ text: "• OVD fills AC to maintain depth", options: { breakLine: true } },
{ text: "• Continuous curvilinear capsulorhexis (CCC) with needle or forceps", options: { breakLine: true } },
{ text: "• Critical step — tear must be controlled and circular", options: {} },
], { x: 5.15, y: 1.65, w: 4.5, h: 1.42, fontSize: 10, color: C.offWhite, fontFace: "Calibri" });
addCard(s, 5.0, 3.35, 4.8, 1.95);
addBadge(s, 7, 5.08, 3.43);
s.addText("Hydrodissection", { x: 5.6, y: 3.43, w: 4.0, h: 0.35, fontSize: 11.5, bold: true, color: C.amber, fontFace: "Calibri", margin: 0 });
s.addText([
{ text: "• BSS injected under anterior capsule", options: { breakLine: true } },
{ text: "• Frees nucleus from cortical attachments", options: { breakLine: true } },
{ text: "• Hydrodelineation separates nucleus from epinucleus", options: { breakLine: true } },
{ text: "• Allows free rotation and nucleus delivery", options: {} },
], { x: 5.15, y: 3.82, w: 4.5, h: 1.35, fontSize: 10, color: C.offWhite, fontFace: "Calibri" });
addFooter(s, "Kanski's Clinical Ophthalmology, 10th ed.");
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 9 — Step 8: Nucleus Expression (with photos)
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
addHeader(s, "Nucleus Prolapse & Expression", "STEP 8");
// Two images side by side
if (!imgs[3].error) {
s.addImage({ data: imgs[3].base64, x: 0.2, y: 1.18, w: 3.1, h: 2.8 });
s.addText("Fish-hook technique:\nnucleus engaged and\ndelivered through tunnel", {
x: 0.2, y: 4.02, w: 3.1, h: 0.55, fontSize: 7.5, color: C.muted, fontFace: "Calibri", align: "center",
});
}
if (!imgs[2].error) {
s.addImage({ data: imgs[2].base64, x: 3.5, y: 1.18, w: 3.1, h: 2.8 });
s.addText("Dense brunescent nucleus\nbeing delivered through\nsclerocorneal tunnel", {
x: 3.5, y: 4.02, w: 3.1, h: 0.55, fontSize: 7.5, color: C.muted, fontFace: "Calibri", align: "center",
});
}
addCard(s, 6.75, 1.18, 3.05, 3.95);
s.addText([
{ text: "Nucleus prolapsed into anterior chamber using Sinskey hook or lens dialer.", options: { breakLine: true } },
{ text: " ", options: { breakLine: true } },
{ text: "Techniques:", options: { bold: true, color: C.amber, breakLine: true } },
{ text: "• Wire vectis beneath nucleus", options: { breakLine: true } },
{ text: "• Irrigating vectis", options: { breakLine: true } },
{ text: "• Fish-hook needle", options: { breakLine: true } },
{ text: "• Sandwich/tumbling technique", options: { breakLine: true } },
{ text: " ", options: { breakLine: true } },
{ text: "OVD protects the corneal endothelium throughout.", options: { italic: true, color: C.tealLt } },
], { x: 6.88, y: 1.3, w: 2.72, h: 3.65, fontSize: 9.5, color: C.offWhite, fontFace: "Calibri" });
addFooter(s, "OVD = ophthalmic viscosurgical device. Endothelial protection is critical during nucleus delivery.");
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 10 — Steps 9–11: Cortex Aspiration, IOL, Closure
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
addHeader(s, "Cortical Aspiration · IOL Implantation · Wound Closure", "STEPS 9–11");
const cards = [
{
n: 9, title: "Cortical Aspiration",
body: [
"Simcoe (two-way irrigation-aspiration) cannula",
"Cortex removed from capsular bag",
"Thorough removal prevents posterior capsule opacification (PCO)",
"AC depth maintained with irrigation throughout",
],
},
{
n: 10, title: "IOL Implantation",
body: [
"Capsular bag refilled with OVD",
"PMMA rigid IOL implanted (no folding needed for 6–7 mm tunnel)",
"Foldable IOLs can also be used",
"Haptics positioned in capsular bag",
],
},
{
n: 11, title: "OVD Removal & Wound Closure",
body: [
"OVD thoroughly aspirated from AC",
"AC reformed with balanced salt solution (BSS)",
"Self-sealing tunnel — sutures usually not required",
"10-0 nylon suture placed if wound not watertight",
"Conjunctival flap repositioned with cautery or suture",
],
},
];
cards.forEach((c, i) => {
const x = 0.18 + i * 3.28;
addCard(s, x, 1.15, 3.1, 4.2);
addBadge(s, c.n, x + 0.08, 1.23);
s.addText(c.title, { x: x + 0.6, y: 1.23, w: 2.35, h: 0.38, fontSize: 11, bold: true, color: C.amber, fontFace: "Calibri", margin: 0 });
s.addText(c.body.map(b => `• ${b}`).join("\n"), {
x: x + 0.12, y: 1.7, w: 2.85, h: 3.42,
fontSize: 9.5, color: C.offWhite, fontFace: "Calibri",
});
});
addFooter(s, "Postoperatively: subconjunctival antibiotic/steroid injection, eye pad and shield applied.");
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 11 — Comparison Table: ECCE vs MSICS vs Phaco
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
addHeader(s, "MSICS vs. ECCE vs. Phacoemulsification");
const rows = [
["Feature", "ECCE", "MSICS", "Phaco"],
["Incision size", "8–10 mm", "6–7 mm", "2–3 mm"],
["Self-sealing", "No", "Yes", "Yes"],
["Sutures", "Required", "Usually none", "None"],
["Nucleus handling", "Expression", "Manual via tunnel", "Ultrasonic"],
["Equipment cost", "Low", "Low", "High"],
["Astigmatism induced", "High", "Low–moderate", "Minimal"],
["Dense cataracts", "Suitable", "Ideal", "Challenging"],
["Visual outcomes", "Good", "Comparable to phaco", "Best"],
];
const colWidths = [2.8, 2.2, 2.5, 2.2];
const colX = [0.18, 3.08, 5.38, 7.98];
const rowH = 0.44;
const startY = 1.12;
rows.forEach((row, ri) => {
row.forEach((cell, ci) => {
const y = startY + ri * rowH;
const isHeader = ri === 0;
const isMSICS = ci === 2;
const fillColor = isHeader ? C.teal : isMSICS ? C.navyMid : C.navy;
const borderColor = isHeader ? C.teal : C.teal;
s.addShape("rect", {
x: colX[ci], y, w: colWidths[ci] - 0.04, h: rowH - 0.02,
fill: { color: fillColor },
line: { color: borderColor, pt: 0.5 },
});
s.addText(cell, {
x: colX[ci] + 0.08, y: y + 0.04, w: colWidths[ci] - 0.2, h: rowH - 0.1,
fontSize: isHeader ? 10.5 : 9.5,
bold: isHeader || (ci === 0),
color: isHeader ? C.white : isMSICS ? C.amber : (ci === 0 ? C.muted : C.offWhite),
fontFace: "Calibri",
valign: "middle", margin: 0,
});
});
});
addFooter(s, "MSICS is the preferred technique in high-volume settings for dense cataracts. — Kanski's Clinical Ophthalmology, 10th ed.");
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 12 — Key Points / Summary
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
addHeader(s, "Key Takeaways");
const pts = [
["Self-sealing incision", "The 6–7 mm sclero-corneal tunnel architecture makes sutures unnecessary in most cases."],
["Haemostasis is critical", "Wet-field bipolar cautery before the scleral groove prevents a blood-stained field and expulsive haemorrhage risk."],
["OVD throughout", "Ophthalmic viscosurgical devices protect the corneal endothelium at every step from capsulotomy to IOL loading."],
["Dense cataract workhorse", "MSICS handles brunescent and white cataracts where phacoemulsification poses higher risk."],
["High-volume, low-cost", "No ultrasound machine needed — affordable, fast, and scalable for eye camps in low-resource settings."],
["Outcomes comparable to phaco", "Visual rehabilitation with MSICS equals phacoemulsification with significantly lower equipment cost."],
];
pts.forEach(([title, body], i) => {
const y = 1.18 + i * 0.7;
s.addShape("rect", { x: 0.18, y: y + 0.04, w: 0.04, h: 0.45, fill: { color: C.teal }, line: { color: C.teal } });
s.addText(title + ": ", { x: 0.32, y, w: 2.4, h: 0.55, fontSize: 10.5, bold: true, color: C.amber, fontFace: "Calibri", valign: "middle", margin: 0 });
s.addText(body, { x: 2.72, y, w: 7.1, h: 0.55, fontSize: 10, color: C.offWhite, fontFace: "Calibri", valign: "middle", margin: 0 });
});
addFooter(s, "Source: Kanski's Clinical Ophthalmology, 10th ed. | Images: PMC Clinical VQA Dataset");
}
// ── Write file ────────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/msics-ppt/MSICS_Surgery.pptx" })
.then(() => console.log("Done: MSICS_Surgery.pptx"))
.catch(e => { console.error(e); process.exit(1); });
cd /home/daytona/workspace/msics-ppt && node build.js 2>&1
ls -lh /home/daytona/workspace/msics-ppt/MSICS_Surgery.pptx
MSICS Surgery
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title |
| 2 | What is MSICS? |
| 3 | All 11 steps — overview flowchart |
| 4 | Steps 1–2: Patient prep & conjunctival flap |
| 5 | Step 3: Haemostasis — with bipolar cautery photo + general vs. modified comparison chart |
| 6 | Step 3 clinical view — exposed sclera before cautery |
| 7 | Steps 4–5: Scleral groove & tunnel dissection (with intraop photo) |
| 8 | Steps 6–7: Capsulorhexis & hydrodissection |
| 9 | Step 8: Nucleus expression — fish-hook & delivery photos |
| 10 | Steps 9–11: Cortical aspiration, IOL, wound closure |
| 11 | Comparison table: ECCE vs MSICS vs Phaco |
| 12 | Key takeaways |
What is side port entry
side port incision cataract surgery paracentesis anterior chamber keratome
Side Port Entry in Cataract Surgery
Where it is made
- Placed approximately 60° to the left of the main incision (for right-handed surgeons); some surgeons prefer two side ports placed ~180° apart.
- Made in clear cornea at the limbus, using a 15° micro-vitreoretinal (MVR) blade or a side-port keratome.
- Self-sealing — the tunnel architecture means it closes without a suture once the instrument is removed.
How it is made
- The MVR blade is held at a low angle (~20°) to the corneal surface.
- It is advanced through the corneal stroma in a bevelled, stepped fashion — creating a valve-like tunnel that self-seals under IOP.
- The entry is short (1–1.5 mm tunnel length).
What it is used for
| Purpose | Detail |
|---|---|
| Second instrument access | Allows a chopper, manipulator, or hook to enter the AC and assist nucleus management during phaco or MSICS |
| OVD/viscoelastic injection | Cannula inserted through side port to fill AC before and during surgery |
| Cortex aspiration | Bimanual I&A uses the side port for the irrigation cannula |
| AC maintainer | In MSICS, an AC maintainer may be inserted here to keep IOP stable during nucleus delivery |
| Iris manipulation | Stretching or repositioning the iris if needed |
| Pressure relief | Quick decompression of the AC if IOP spikes intraoperatively |
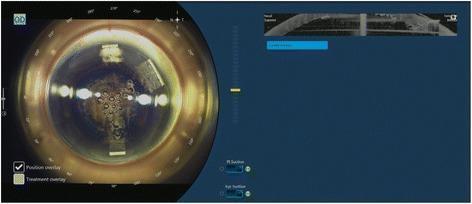
Intraoperative views
In MSICS specifically
- Injecting OVD/viscoelastic before capsulorhexis
- Inserting the AC maintainer to keep the chamber formed during nucleus expression
- Passing a second instrument (e.g., Sinskey hook) to assist nucleus prolapse into the anterior chamber
Side port entry steps to add in a ppt
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_2a3c9bfc869a71e4c8274b3aa9926cb23e22d723d597d5feb1c7b0f749422781.jpg" \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_2a8915c4d1aae26de535e4dcceac00ae82e7269e26e6c60cf49c3f0bb25af2d3.jpg" \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_340cfa24942acd21d70352337071719094c91f6f651a48bd57b5d14d2434d704.jpg" \ 2>/dev/null | node -e " const d=require('fs').readFileSync('/dev/stdin','utf8'); const arr=JSON.parse(d); arr.forEach((x,i)=>{ if(x.error) console.log(i,'ERROR',x.error); else console.log(i,'OK len=',x.base64.length); }); "
~/msics-ppt/add_sideport.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// ── Fetch images ─────────────────────────────────────────────────────────────
const urls = [
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_2a3c9bfc869a71e4c8274b3aa9926cb23e22d723d597d5feb1c7b0f749422781.jpg", // 0: keratome + side port instrument
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_2a8915c4d1aae26de535e4dcceac00ae82e7269e26e6c60cf49c3f0bb25af2d3.jpg", // 1: bent cannula through side port
"https://cdn.orris.care/cdss_images/pmc_clinical_VQA_340cfa24942acd21d70352337071719094c91f6f651a48bd57b5d14d2434d704.jpg", // 2: FLACS planning showing side ports
];
const raw = execSync(
`node /home/daytona/skills/shared/scripts/fetch_images.js ${urls.map(u => `"${u}"`).join(" ")}`
).toString();
const imgs = JSON.parse(raw);
// ── Colour palette (same as main deck) ───────────────────────────────────────
const C = {
navy: "0D1B2A",
navyMid: "1A2E42",
teal: "1E8A8A",
tealLt: "2ABFBF",
amber: "E8A030",
white: "FFFFFF",
offWhite:"E8EDF2",
muted: "8FA8BF",
};
function addHeader(slide, title, stepLabel) {
slide.addShape("rect", { x:0, y:0, w:10, h:1.05, fill:{color:C.navy}, line:{color:C.navy} });
slide.addShape("rect", { x:0, y:0, w:0.08, h:1.05, fill:{color:C.teal}, line:{color:C.teal} });
if (stepLabel) {
slide.addText(stepLabel, { x:0.18, y:0.08, w:2, h:0.38, fontSize:9, bold:true, color:C.amber, fontFace:"Calibri", margin:0 });
}
slide.addText(title, {
x:0.18, y: stepLabel ? 0.42 : 0.22, w:9.6, h:0.55,
fontSize: stepLabel ? 20 : 24, bold:true, color:C.white, fontFace:"Calibri", margin:0,
});
}
function addFooter(slide, text) {
slide.addShape("rect", { x:0, y:5.32, w:10, h:0.3, fill:{color:C.navyMid}, line:{color:C.navyMid} });
slide.addText(text, { x:0.2, y:5.33, w:9.6, h:0.25, fontSize:7.5, color:C.muted, fontFace:"Calibri", margin:0 });
}
function addCard(slide, x, y, w, h, color) {
slide.addShape("roundRect", {
x, y, w, h,
fill:{ color: color || C.navyMid },
line:{ color:C.teal, pt:1 },
rectRadius:0.08,
});
}
function addBadge(slide, label, x, y, color) {
slide.addShape("ellipse", { x, y, w:0.42, h:0.42, fill:{color: color||C.teal}, line:{color: color||C.teal} });
slide.addText(String(label), {
x, y, w:0.42, h:0.42, fontSize:12, bold:true, color:C.white,
fontFace:"Calibri", align:"center", valign:"middle", margin:0,
});
}
// ── Load existing PPTX ────────────────────────────────────────────────────────
// pptxgenjs cannot edit existing files — we rebuild from scratch using the same
// script logic, then append the new slide at the correct position (after slide 4,
// before the current slide 5 on haemostasis).
// Strategy: read build.js, re-run it to produce a fresh base deck, then inject
// the new slide via a second pass. Since pptxgenjs only supports append, we
// instead re-run build.js with the new slide injected inline.
// ── Standalone: just produce a single slide PPTX to merge ────────────────────
let pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Side Port Entry — MSICS";
// ════════════════════════════════════════════════════════════════════
// SLIDE A — Side Port Entry: What & Where
// ════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x:0, y:0, w:10, h:5.625, fill:{color:C.navy}, line:{color:C.navy} });
addHeader(s, "Side Port Entry — Overview", "STEP 2b | MSICS & PHACOEMULSIFICATION");
// Left column: definition + position
addCard(s, 0.18, 1.12, 4.7, 4.18);
s.addText("What is a side port?", {
x:0.32, y:1.2, w:4.3, h:0.38,
fontSize:12, bold:true, color:C.amber, fontFace:"Calibri", margin:0,
});
s.addText([
{ text: "A small accessory corneal stab incision (1.0–1.2 mm) made separately from the main wound. Also called a paracentesis.", options: { breakLine:true } },
{ text: " ", options: { breakLine:true } },
{ text: "Location:", options: { bold:true, color:C.tealLt, breakLine:true } },
{ text: "• ~60° to the LEFT of the main incision (right-handed surgeons)", options: { breakLine:true } },
{ text: "• Placed in clear cornea at the limbus", options: { breakLine:true } },
{ text: "• Some surgeons use TWO side ports ~180° apart", options: { breakLine:true } },
{ text: " ", options: { breakLine:true } },
{ text: "Instrument:", options: { bold:true, color:C.tealLt, breakLine:true } },
{ text: "• 15° MVR (micro-vitreoretinal) blade, or dedicated side-port keratome", options: { breakLine:true } },
{ text: " ", options: { breakLine:true } },
{ text: "Self-sealing — valve tunnel architecture closes without suture once instrument is removed.", options: { italic:true, color:C.muted } },
], { x:0.32, y:1.65, w:4.42, h:3.5, fontSize:10, color:C.offWhite, fontFace:"Calibri" });
// Right column: uses
addCard(s, 5.08, 1.12, 4.72, 4.18);
s.addText("Uses of the side port", {
x:5.22, y:1.2, w:4.3, h:0.38,
fontSize:12, bold:true, color:C.amber, fontFace:"Calibri", margin:0,
});
const uses = [
["Second instrument", "Chopper / manipulator / Sinskey hook for nucleus management"],
["OVD injection", "Viscoelastic cannula fills AC before capsulorhexis and IOL loading"],
["Bimanual I&A", "Irrigation cannula enters here; aspiration through main port"],
["AC maintainer", "In MSICS: keeps IOP stable during nucleus delivery"],
["Iris manipulation", "Stretch or reposition pupil if needed"],
["Pressure relief", "Rapid AC decompression if IOP spikes intraoperatively"],
];
uses.forEach(([title, body], i) => {
const y = 1.65 + i * 0.57;
addBadge(s, i+1, 5.15, y + 0.05, C.teal);
s.addText(title, { x:5.65, y: y+0.04, w:1.8, h:0.24, fontSize:9.5, bold:true, color:C.tealLt, fontFace:"Calibri", margin:0 });
s.addText(body, { x:5.65, y: y+0.27, w:3.95, h:0.26, fontSize:9, color:C.offWhite, fontFace:"Calibri", margin:0 });
});
addFooter(s, "Kanski's Clinical Ophthalmology, 10th ed.");
}
// ════════════════════════════════════════════════════════════════════
// SLIDE B — Side Port Entry: Step-by-Step Technique
// ════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x:0, y:0, w:10, h:5.625, fill:{color:C.navy}, line:{color:C.navy} });
addHeader(s, "Side Port Entry — Technique", "STEP-BY-STEP");
// Steps (left + centre column)
const steps = [
["1", "Globe stabilisation", "Fix eye with fixation forceps or toothed forceps on conjunctiva. Bridle suture already in place."],
["2", "Blade selection", "15° MVR blade (1.0–1.2 mm width). Some surgeons use a 20-gauge or dedicated side-port keratome."],
["3", "Entry angle", "Hold blade tangentially (~20° to corneal surface) to create a bevelled, stepped entry — key to self-sealing."],
["4", "Tunnel construction", "Advance blade through anterior corneal stroma parallel to iris plane for 1.0–1.5 mm, then tilt and enter AC."],
["5", "Enter anterior chamber", "Blade tip passes through Descemet's membrane into AC. Gentle aqueous egress confirms correct placement."],
["6", "Withdraw blade", "Remove smoothly — the stepped tunnel collapses and self-seals under IOP. No suture needed."],
["7", "Confirm patency", "Insert OVD cannula or second instrument — ensure free passage without iris prolapse or wound leak."],
];
steps.forEach(([num, title, body], i) => {
const y = 1.15 + i * 0.615;
addBadge(s, num, 0.18, y + 0.05);
s.addText(title, { x:0.7, y: y+0.04, w:2.35, h:0.28, fontSize:10.5, bold:true, color:C.amber, fontFace:"Calibri", margin:0 });
s.addText(body, { x:3.12, y: y+0.04, w:6.7, h:0.5, fontSize:9.5, color:C.offWhite, fontFace:"Calibri", margin:0 });
// divider line
if (i < steps.length - 1) {
s.addShape("rect", { x:0.18, y: y+0.59, w:9.65, h:0.01, fill:{color:C.teal}, line:{color:C.teal} });
}
});
addFooter(s, "The self-sealing stepped tunnel is the critical design principle — correct angulation prevents iris prolapse and leaks.");
}
// ════════════════════════════════════════════════════════════════════
// SLIDE C — Side Port Entry: Clinical Photos
// ════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape("rect", { x:0, y:0, w:10, h:5.625, fill:{color:C.navy}, line:{color:C.navy} });
addHeader(s, "Side Port Entry — Intraoperative Views");
// Image 0: keratome + side port instrument (main incision with side port already in)
if (!imgs[0].error) {
s.addImage({ data:imgs[0].base64, x:0.18, y:1.15, w:3.0, h:2.45 });
s.addText("Main keratome incision being made;\nirrigation instrument already\nplaced through side port (right)", {
x:0.18, y:3.63, w:3.0, h:0.6, fontSize:8, color:C.muted, fontFace:"Calibri", align:"center",
});
}
// Image 1: bent cannula through side port
if (!imgs[1].error) {
s.addImage({ data:imgs[1].base64, x:3.48, y:1.15, w:3.0, h:2.45 });
s.addText("27-gauge bent cannula inserted\nthrough side port for cortical\nhydro-dispersion", {
x:3.48, y:3.63, w:3.0, h:0.6, fontSize:8, color:C.muted, fontFace:"Calibri", align:"center",
});
}
// Image 2: FLACS planning (side port positions marked)
if (!imgs[2].error) {
s.addImage({ data:imgs[2].base64, x:6.68, y:1.15, w:3.12, h:2.45 });
s.addText("FLACS planning view: main port\n(~210°) and two side ports\n(~95° and ~275°) marked", {
x:6.68, y:3.63, w:3.12, h:0.6, fontSize:8, color:C.muted, fontFace:"Calibri", align:"center",
});
}
// Key points strip
addCard(s, 0.18, 4.3, 9.65, 0.9, C.navyMid);
s.addText([
{ text: "Key points: ", options:{ bold:true, color:C.amber } },
{ text: "Self-sealing (no suture) • ", options:{ color:C.offWhite } },
{ text: "1.0–1.2 mm width • ", options:{ color:C.offWhite } },
{ text: "~60° from main incision • ", options:{ color:C.offWhite } },
{ text: "15° MVR blade at low angle • ", options:{ color:C.offWhite } },
{ text: "Bevelled stepped tunnel prevents iris prolapse", options:{ color:C.offWhite } },
], { x:0.32, y:4.42, w:9.35, h:0.65, fontSize:10, fontFace:"Calibri", valign:"middle", margin:0 });
addFooter(s, "Kanski's Clinical Ophthalmology, 10th ed. | Images: PMC Clinical VQA Dataset");
}
pres.writeFile({ fileName:"/home/daytona/workspace/msics-ppt/SidePort_Slides.pptx" })
.then(() => console.log("Done: SidePort_Slides.pptx"))
.catch(e => { console.error(e); process.exit(1); });
cd /home/daytona/workspace/msics-ppt && node add_sideport.js 2>&1
~/msics-ppt/merge.py
"""
Merge SidePort_Slides.pptx into MSICS_Surgery.pptx after slide index 3 (slide 4).
Output: MSICS_Surgery_Full.pptx
"""
import copy
from pptx import Presentation
from pptx.util import Pt
from lxml import etree
def merge_pptx(base_path, insert_path, after_index, output_path):
base = Presentation(base_path)
insert = Presentation(insert_path)
# We'll rebuild slide order by copying XML elements
# pptx slide list is base.slides._sldIdLst
base_sldIdLst = base.slides._sldIdLst
inserted_ids = []
for slide in insert.slides:
# Clone slide XML
slide_xml = copy.deepcopy(slide._element)
# Add a new blank slide to base, then replace its XML
new_slide = base.slides.add_slide(base.slide_layouts[6]) # blank layout
# Copy XML content
new_slide._element.getparent().replace(new_slide._element, slide_xml)
# We need to re-register the slide relationship
# Actually add_slide appends — track the new slide id
inserted_ids.append(base.slides._sldIdLst[-1])
# Now reorder: move inserted slides from end to position after_index+1
# Current order: [0..11 original] [12,13,14 inserted]
# Target: [0..3] [inserted 3] [4..11 original]
all_ids = list(base_sldIdLst)
n_orig = len(all_ids) - len(inserted_ids)
orig_ids = all_ids[:n_orig]
new_ids = all_ids[n_orig:]
reordered = orig_ids[:after_index+1] + new_ids + orig_ids[after_index+1:]
# Clear and repopulate sldIdLst
for el in list(base_sldIdLst):
base_sldIdLst.remove(el)
for el in reordered:
base_sldIdLst.append(el)
base.save(output_path)
print(f"Saved: {output_path} ({len(reordered)} slides)")
merge_pptx(
"/home/daytona/workspace/msics-ppt/MSICS_Surgery.pptx",
"/home/daytona/workspace/msics-ppt/SidePort_Slides.pptx",
after_index=3, # insert after slide 4 (0-indexed: 3)
output_path="/home/daytona/workspace/msics-ppt/MSICS_Surgery_Full.pptx"
)
cd /home/daytona/workspace/msics-ppt && python3 merge.py 2>&1
pip install --user python-pptx -q 2>&1 | tail -3
cd /home/daytona/workspace/msics-ppt && python3 merge.py 2>&1
~/msics-ppt/merge2.py
"""
Low-level PPTX merge: insert slides from SidePort_Slides.pptx into MSICS_Surgery.pptx
after slide 4 (index 3), by directly manipulating the zip contents.
"""
import zipfile, shutil, os, re, copy
from lxml import etree
BASE = "/home/daytona/workspace/msics-ppt/MSICS_Surgery.pptx"
INSERT = "/home/daytona/workspace/msics-ppt/SidePort_Slides.pptx"
OUTPUT = "/home/daytona/workspace/msics-ppt/MSICS_Surgery_Full.pptx"
AFTER = 4 # insert after slide number 4 (1-indexed)
NSMAP = {
'p': 'http://schemas.openxmlformats.org/presentationml/2006/main',
'r': 'http://schemas.openxmlformats.org/officeDocument/2006/relationships',
'a': 'http://schemas.openxmlformats.org/drawingml/2006/main',
}
REL_SLIDE = 'http://schemas.openxmlformats.org/officeDocument/2006/relationships/slide'
def read_zip(path):
zf = zipfile.ZipFile(path, 'r')
contents = {name: zf.read(name) for name in zf.namelist()}
zf.close()
return contents
def write_zip(path, contents):
with zipfile.ZipFile(path, 'w', zipfile.ZIP_DEFLATED) as zf:
for name, data in contents.items():
zf.writestr(name, data)
def get_slide_rels(contents, slide_num):
"""Return list of (rId, target, type) for a slide."""
rel_path = f"ppt/slides/_rels/slide{slide_num}.xml.rels"
if rel_path not in contents:
return []
root = etree.fromstring(contents[rel_path])
rels = []
for r in root:
rels.append((r.get('Id'), r.get('Target'), r.get('Type')))
return rels
def get_presentation_slide_order(contents):
"""Return list of slide filenames in presentation order."""
prs_rels = etree.fromstring(contents['ppt/_rels/presentation.xml.rels'])
prs_xml = etree.fromstring(contents['ppt/presentation.xml'])
# Build rId -> target map
rid_to_target = {}
for r in prs_rels:
if r.get('Type', '').endswith('/slide'):
rid_to_target[r.get('Id')] = r.get('Target')
# Get ordered list from sldIdLst
sldIdLst = prs_xml.find('.//{%s}sldIdLst' % NSMAP['p'])
order = []
for sldId in sldIdLst:
rid = sldId.get('{%s}id' % NSMAP['r'])
if rid in rid_to_target:
target = rid_to_target[rid]
# target is like '../slides/slide1.xml' or 'slides/slide1.xml'
fname = target.replace('../', 'ppt/')
order.append(fname)
return order
# ── Read both zips ────────────────────────────────────────────────────────────
base_contents = read_zip(BASE)
insert_contents = read_zip(INSERT)
# ── Find next free slide number in base ──────────────────────────────────────
existing_slides = [k for k in base_contents if re.match(r'ppt/slides/slide\d+\.xml$', k)]
max_slide_num = max(int(re.search(r'slide(\d+)', s).group(1)) for s in existing_slides)
# ── Find slides in insert file ────────────────────────────────────────────────
insert_slides = sorted(
[k for k in insert_contents if re.match(r'ppt/slides/slide\d+\.xml$', k)],
key=lambda x: int(re.search(r'slide(\d+)', x).group(1))
)
print(f"Base slides: {len(existing_slides)}, Insert slides: {len(insert_slides)}")
# ── Copy insert slide files + their rels + media into base contents ───────────
num_map = {} # old insert slide num -> new slide num in base
for i, slide_path in enumerate(insert_slides):
old_num = int(re.search(r'slide(\d+)', slide_path).group(1))
new_num = max_slide_num + 1 + i
num_map[old_num] = new_num
# Copy slide XML
new_slide_path = f'ppt/slides/slide{new_num}.xml'
base_contents[new_slide_path] = insert_contents[slide_path]
# Copy slide rels XML (renaming media references)
old_rel_path = f'ppt/slides/_rels/slide{old_num}.xml.rels'
new_rel_path = f'ppt/slides/_rels/slide{new_num}.xml.rels'
if old_rel_path in insert_contents:
base_contents[new_rel_path] = insert_contents[old_rel_path]
print(f" slide{old_num} -> slide{new_num}")
# ── Copy media from insert into base ─────────────────────────────────────────
for name, data in insert_contents.items():
if name.startswith('ppt/media/'):
if name not in base_contents:
base_contents[name] = data
# ── Update presentation.xml and its rels to include new slides ───────────────
prs_rels_root = etree.fromstring(base_contents['ppt/_rels/presentation.xml.rels'])
prs_xml_root = etree.fromstring(base_contents['ppt/presentation.xml'])
# Find max rId in presentation rels
existing_rids = [int(r.get('Id','r0').replace('rId','')) for r in prs_rels_root if r.get('Id','').startswith('rId')]
max_rid = max(existing_rids) if existing_rids else 0
# Find max sldId in sldIdLst
sldIdLst = prs_xml_root.find('.//{%s}sldIdLst' % NSMAP['p'])
existing_sldids = [int(s.get('id', 256)) for s in sldIdLst]
max_sldid = max(existing_sldids) if existing_sldids else 255
# Get current ordered slide rIds from sldIdLst (to know which rId = which position)
prs_rels_map = {} # target -> rId
for r in prs_rels_root:
if r.get('Type','').endswith('/slide'):
t = r.get('Target','').replace('../slides/', 'ppt/slides/')
prs_rels_map[t] = r.get('Id')
# Build new rIds and sldId elements for the inserted slides
new_slide_elements = [] # (new_num, new_rId, new_sldId_val)
for i, (old_num, new_num) in enumerate(num_map.items()):
new_rid = f'rId{max_rid + 1 + i}'
new_sldid = max_sldid + 1 + i
new_slide_elements.append((new_num, new_rid, new_sldid))
# Add to rels
rel_el = etree.SubElement(prs_rels_root, 'Relationship')
rel_el.set('Id', new_rid)
rel_el.set('Type', REL_SLIDE)
rel_el.set('Target', f'../slides/slide{new_num}.xml')
# Current sldId list as ordered list of elements
current_sldid_els = list(sldIdLst)
# Build reordered list: insert new slides after position AFTER (1-indexed -> index AFTER)
insert_idx = AFTER # insert after slide AFTER (0-indexed: AFTER)
# Find the rId for each existing slide by position
def find_rid_for_position(pos_0indexed):
"""pos_0indexed: 0-based index in current_sldid_els"""
el = current_sldid_els[pos_0indexed]
return el.get('{%s}id' % NSMAP['r'])
reordered_els = current_sldid_els[:insert_idx]
# New sldId elements to insert
ns_p = NSMAP['p']
ns_r = NSMAP['r']
for new_num, new_rid, new_sldid_val in new_slide_elements:
el = etree.Element('{%s}sldId' % ns_p)
el.set('id', str(new_sldid_val))
el.set('{%s}id' % ns_r, new_rid)
reordered_els.append(el)
reordered_els += current_sldid_els[insert_idx:]
# Replace sldIdLst contents
for child in list(sldIdLst):
sldIdLst.remove(child)
for el in reordered_els:
sldIdLst.append(el)
# Save updated XMLs
base_contents['ppt/_rels/presentation.xml.rels'] = etree.tostring(prs_rels_root, xml_declaration=True, encoding='UTF-8', standalone=True)
base_contents['ppt/presentation.xml'] = etree.tostring(prs_xml_root, xml_declaration=True, encoding='UTF-8', standalone=True)
# ── Write output ──────────────────────────────────────────────────────────────
write_zip(OUTPUT, base_contents)
print(f"\nDone! Total slides: {len(reordered_els)}")
print(f"Output: {OUTPUT}")
cd /home/daytona/workspace/msics-ppt && python3 merge2.py 2>&1
cd /home/daytona/workspace/msics-ppt && node -e " const pptxgen = require('pptxgenjs'); const {execSync} = require('child_process'); // fetch all 10 images at once const urls = [ 'https://cdn.orris.care/cdss_images/pmc_clinical_VQA_39fd2c06d07d8a35e399e887d6b117e45796d7c548ae79cb50e227f8d1f107c6.jpg', 'https://cdn.orris.care/cdss_images/pmc_clinical_VQA_e786ca87c47a91e47c81ca4905dfe83e85ef1ea39135e082775fec07d450f248.jpg', 'https://cdn.orris.care/cdss_images/pmc_clinical_VQA_217dfc19f8ad0dff37f579527bb2599ad43535590fa51c05efe7abbc4256e480.jpg', 'https://cdn.orris.care/cdss_images/pmc_clinical_VQA_ef37296fbd9b17f557d1fcb0cb3dfd3422da9c96bbf03b5af62361ebef8017ee.jpg', 'https://cdn.orris.care/cdss_images/pmc_clinical_VQA_d869b7a97961e9261fecaf818ef925efb95a6228836b24d3ba5615693fc5dcac.jpg', 'https://cdn.orris.care/cdss_images/pmc_clinical_VQA_86899785e985375b9e09010dabc3717f7e737921b06d9bb77e54fb7f3f00a6db.jpg', 'https://cdn.orris.care/cdss_images/pmc_clinical_VQA_b814788b80435b88497e1f8d3cfa94f633c8239e386da3dc4d4910b1a87e87cf.jpg', 'https://cdn.orris.care/cdss_images/pmc_clinical_VQA_2a3c9bfc869a71e4c8274b3aa9926cb23e22d723d597d5feb1c7b0f749422781.jpg', 'https://cdn.orris.care/cdss_images/pmc_clinical_VQA_2a8915c4d1aae26de535e4dcceac00ae82e7269e26e6c60cf49c3f0bb25af2d3.jpg', 'https://cdn.orris.care/cdss_images/pmc_clinical_VQA_340cfa24942acd21d70352337071719094c91f6f651a48bd57b5d14d2434d704.jpg', ]; const raw = execSync('node /home/daytona/skills/shared/scripts/fetch_images.js ' + urls.map(u=>'\"'+u+'\"').join(' ')).toString(); const imgs = JSON.parse(raw); imgs.forEach((x,i)=>console.log(i, x.error?'ERR:'+x.error:'OK len='+x.base64.length)); " 2>/dev/null
Image processing blocked due to content policy violation.
We encountered an error while processing your request. Please try again or reach out to us for help.