Dlitiazem vs verapamil
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a detailed comparison drawn from Katzung's Basic and Clinical Pharmacology (16th ed.), Lippincott Illustrated Reviews Pharmacology, and Tintinalli's Emergency Medicine.
Diltiazem vs Verapamil - Head-to-Head Comparison
Both are non-dihydropyridine (non-DHP) calcium channel blockers that block voltage-gated L-type calcium channels from the intracellular side, binding more effectively to open and inactivated channels.
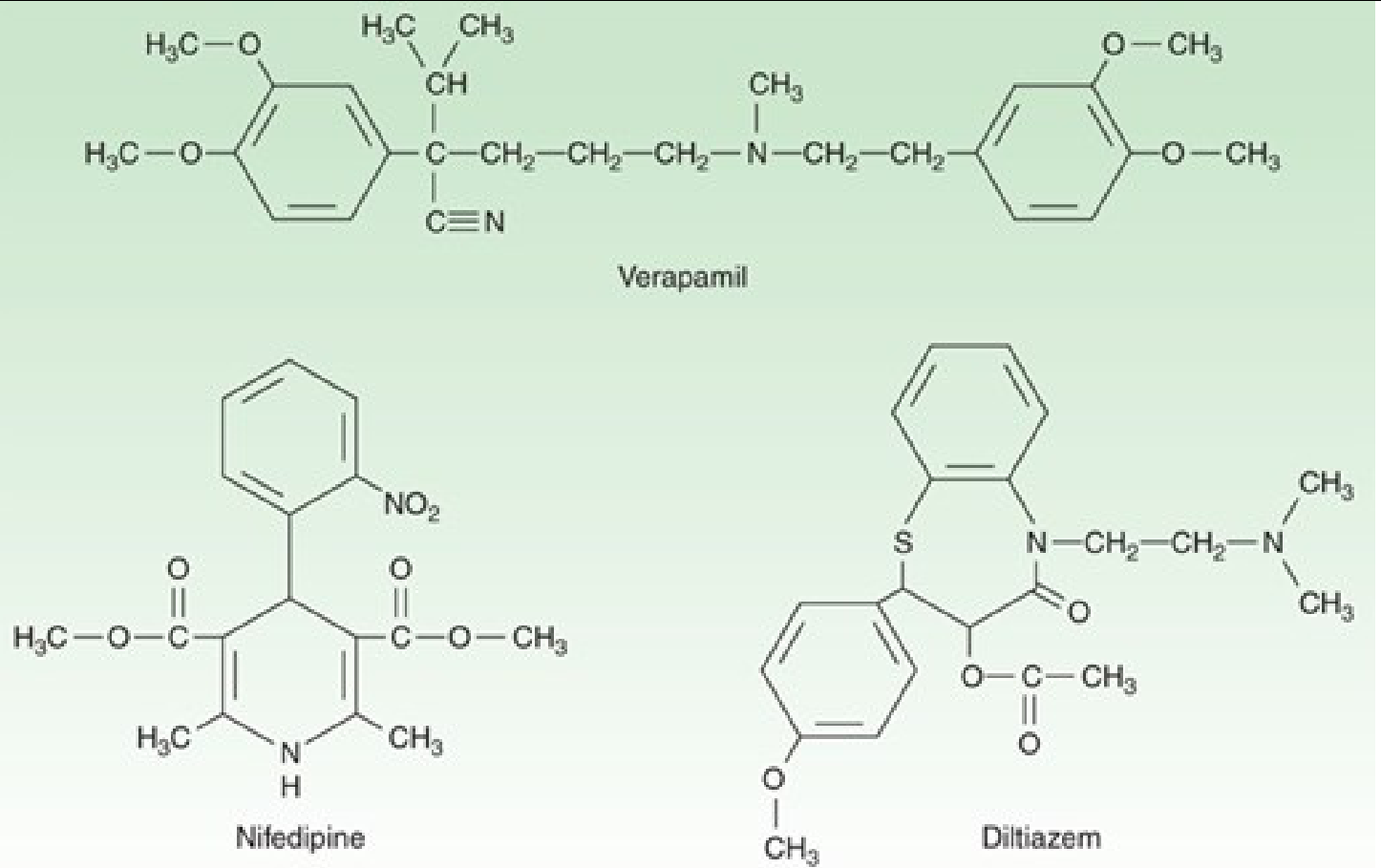
1. Drug Class / Chemistry
| Feature | Diltiazem | Verapamil |
|---|---|---|
| Chemical class | Benzothiazepine | Phenylalkylamine |
| Binding site on L-type channel | α1 subunit (diltiazem receptor site) | α1 subunit (verapamil receptor site - closely related but not identical) |
The two drugs bind to closely related but distinct receptor sites on the same α1 subunit. Binding at one site allosterically modulates the other. - Katzung, p. 316
2. Selectivity: Heart vs Vasculature
This is the most clinically important difference:
| Feature | Diltiazem | Verapamil |
|---|---|---|
| Cardiac depression | Moderate | Greater (more potent) |
| Vascular selectivity | Intermediate | Less vasodilatory than DHPs; also blocks vascular K+ channels (limits pure vasodilation) |
| AV nodal depression | Significant | More potent - greater AV nodal depression |
| Reflex tachycardia | Minimal | Minimal |
| Sodium channel block | Slight | Modest (more than diltiazem) |
Lippincott's puts it clearly: "Amlodipine (like nifedipine) is a peripheral vasodilator, diltiazem is intermediate with actions on both myocardial and peripheral calcium channels, and verapamil has the greatest effect on the myocardium." - Lippincott Pharmacology
3. Cardiac Electrophysiology
Both drugs slow SA node automaticity and AV node conduction, prolong PR interval, and increase AV nodal refractory period. However:
- Verapamil is more potent than diltiazem at AV nodal depression - Tintinalli's Emergency Medicine, p. 171
- Verapamil has modest sodium channel blocking activity; diltiazem has even less
- Both preferentially suppress tachycardias in calcium-dependent cells (SA and AV nodes) - this is the basis for their antiarrhythmic use (Class IV)
4. Pharmacokinetics
| Parameter | Diltiazem | Verapamil |
|---|---|---|
| Oral absorption | IR ~98%, ER ~93-95% | >90% |
| Oral bioavailability | ~40% (extensive first-pass) | 20-35% (extensive first-pass) |
| Plasma protein binding | 70-80% | ~90% |
| Volume of distribution | 3-13 L/kg | ~3.89 L/kg |
| Half-life (IR oral) | 3-4.5 h | 2.8-7.4 h (single dose); longer with repeat dosing |
| IV onset | 3 min | 3-5 min |
| IV duration | 1-3 h (bolus) | 0.5-6 h |
| Metabolism | Hepatic, CYP450 + conjugation; active metabolites | Hepatic, CYP450; active metabolites |
Data from Tintinalli's Emergency Medicine, Table 19-18
Key point: Diltiazem IR has a rapid oral onset (30-60 min), making transition from IV to oral relatively straightforward. Verapamil has lower oral bioavailability (~20-35% vs ~40% for diltiazem) due to even heavier first-pass metabolism.
5. Clinical Indications
| Indication | Diltiazem | Verapamil |
|---|---|---|
| PSVT (acute termination) | Yes (IV) | Preferred - conversion rate ~90%, similar to adenosine |
| Rate control in AF/Aflutter | Preferred (IV infusion) | Yes, but less common |
| Stable angina (effort) | Yes | Yes |
| Variant (Prinzmetal) angina | Yes | Yes |
| Hypertension | Yes | Yes |
| Hypertrophic cardiomyopathy | Yes | Preferred (greater cardiac depression reduces LVOT gradient) |
| Rate control in AF with bronchospasm | Yes (advantage over beta-blockers) | Yes |
From Katzung: "In patients with a history of atrial tachycardia, flutter, and fibrillation, verapamil and diltiazem provide a distinct advantage because of their antiarrhythmic effects." - p. 320
6. Contraindications (shared)
Both are contraindicated in:
- Wide complex tachyarrhythmias (risk of VF in pre-excitation/WPW)
- Sick sinus syndrome (without pacemaker)
- 2nd or 3rd degree AV block
- Severe hypotension / cardiogenic shock
- IV use within a few hours of IV beta-blockers (risk of complete AV block, asystole)
- Ventricular tachycardia
7. Adverse Effects
| Adverse Effect | Diltiazem | Verapamil |
|---|---|---|
| Bradycardia / AV block | Yes | Yes (more pronounced) |
| Hypotension | Yes | Yes |
| Heart failure exacerbation | Yes | Yes (greater concern) |
| Constipation | Mild | Prominent - most common GI complaint |
| Gingival hyperplasia | No | Yes (notable with chronic use) |
| Peripheral edema | Present | Present |
| Insulin secretion inhibition | No | Yes (at high doses - inhibits beta-cell Ca2+ influx) |
Constipation is particularly common with verapamil. - Katzung, p. 317
8. Drug Interactions (shared)
Both inhibit CYP3A4 and P-glycoprotein:
- Statins (atorvastatin, lovastatin, simvastatin): decreased elimination - myopathy risk
- Cyclosporine/tacrolimus/sirolimus: increased immunosuppressant levels
- Digoxin: decreased digoxin elimination - increased digoxin toxicity risk
- Colchicine: decreased colchicine elimination
Verapamil additionally: blocks P-glycoprotein (used experimentally to reverse multidrug resistance in cancer cells)
9. Dosing Summary
| Route | Diltiazem | Verapamil |
|---|---|---|
| IV bolus (AF/SVT) | 0.25 mg/kg over 2 min; repeat 0.35 mg/kg if needed | 5-10 mg (0.075-0.15 mg/kg) over 2 min; repeat 10 mg after 15-30 min |
| IV infusion | 5-15 mg/h | Continuous if bolus effective |
| Oral IR | 30-120 mg TID-QID | 80-120 mg TID |
| Oral ER | Once or twice daily formulations | Once or twice daily |
Quick Memory Summary
| Key Point | Winner |
|---|---|
| More potent AV node depression | Verapamil |
| Better for PSVT termination | Verapamil |
| Better for AF rate control (IV) | Diltiazem |
| More negative inotrope | Verapamil |
| Intermediate cardiac/vascular effects | Diltiazem |
| Worse constipation | Verapamil |
| Gingival hyperplasia | Verapamil only |
| Better tolerated overall | Diltiazem |
| Higher oral bioavailability | Diltiazem (~40% vs 20-35%) |
The bottom line: diltiazem sits in the middle ground - it has meaningful cardiac effects (AV nodal slowing, mild negative inotropy) while also producing good vasodilation. Verapamil leans more cardiac, with stronger AV nodal and myocardial effects but relatively less peripheral vasodilation, and carries a higher burden of side effects.
This is a shared conversation. Sign in to Orris to start your own chat.