Sandifer like posturing images and explain
Reading File
Finding Sources
Searching the Web
Sandifer syndrome posturing images clinical photos infants
Loading Image
Loading Image
Reading File
Reading File
Searching the Web
Sandifer syndrome opisthotonus torticollis infant posturing clinical image
Reading File
Loading Image
Loading Image
Reading Web Page
https://emsj.ca/from-reflux-to-rocking-unravelling-sandifer-…
I now have comprehensive information and a clinical image. Let me compile the full response:
Sandifer Syndrome - Posturing & Explanation
Clinical Image
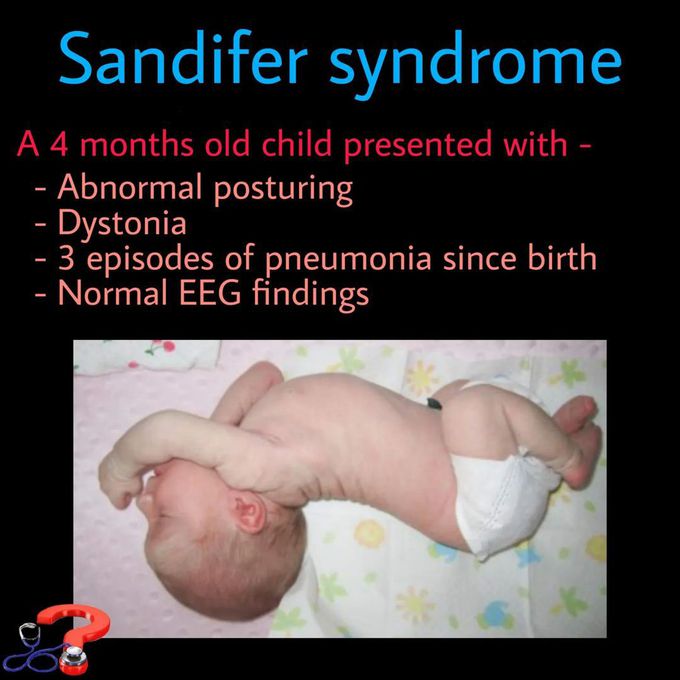
4-month-old with Sandifer syndrome: note the characteristic back-arching opisthotonic posture, with neck hyperextension. EEG was normal.
What is Sandifer Syndrome?
Sandifer syndrome (SS) is a condition in which gastroesophageal reflux disease (GERD) - or hiatal hernia - triggers paroxysmal dystonic posturing in infants and young children. Named after Dr. Paul Sandifer (described in 1964 by Sandifer and Kinsbourne), it is the classic GI-neurological mimic of a seizure disorder.
- Age: typically 2 months to 2 years
- More common in boys
- Associated with GERD, esophagitis, or hiatal hernia
The Classic Postures (What You See)
| Posture | Description |
|---|---|
| Opisthotonus | Severe arching of the back, rigid hyperextension of the spine |
| Retrocollis/Torticollis | Head and neck tilted/twisted; head tilted downward or laterally |
| Laterocollis | Lateral neck deviation |
| Elbow flexion | Elbows flexed and held posteriorly |
| Hip hyperextension | Hips extended during episodes |
| Staring/eye deviation | Blank stare or eye movement changes |
Episodes are typically:
- Brief (seconds to minutes)
- Paroxysmal - sudden onset and offset
- Post-prandial - occurring during or shortly after feeds
- Absent during sleep - a key distinguishing feature from epilepsy
- No loss of consciousness, no postictal state
Pathophysiology (Proposed Mechanism)
Esophageal irritation from acid reflux activates vagal afferents, which trigger abnormal motor responses via central neural pathways - particularly the nucleus tractus solitarius and related brainstem motor nuclei - resulting in dystonic posturing and torticollis.
An alternative hypothesis: the posturing is a voluntary protective reflex to alleviate esophageal discomfort. Evidence from Puntis et al. shows that the arching posture increases the amplitude and velocity of esophageal peristalsis, which may promote acid clearance and provide symptom relief. Either way, the posturing resolves when GERD is treated effectively.
Why It Mimics Seizures (The Diagnostic Trap)
| Feature | Sandifer Syndrome | Epileptic Seizure |
|---|---|---|
| Trigger | Feeding / reflux | Variable |
| Timing | Post-prandial | Any time |
| During sleep | Absent | May occur |
| Loss of consciousness | No | Often yes |
| Postictal state | No | Yes |
| EEG | Normal | Abnormal |
| Treatment response | Anti-reflux therapy | Anticonvulsants |
From Rosen's Emergency Medicine: "Infants with gastrointestinal reflux may have Sandifer syndrome and appear to have seizure-like movements with episodes of abnormal posturing, arching of the back, and torticollis."
From Localization in Clinical Neurology, 8e: "Sandifer syndrome refers to a spasmodic tilting downward of the head and neck after eating a meal, occurring mainly in boys as a result of gastroesophageal reflux."
Associated Clinical Features
- Regurgitation / vomiting
- Irritability (especially around feeds)
- Poor weight gain / failure to thrive
- Recurrent aspiration pneumonia (acid microaspiration)
- Iron-deficiency anemia (from occult esophageal blood loss)
- Hiatal hernia (in a subset)
Diagnosis
- Clinical diagnosis primarily
- EEG - normal (rules out epilepsy)
- Barium swallow / upper GI series - shows GERD, possible hiatal hernia
- Esophageal pH monitoring - gold standard to confirm acid reflux episodes correlate with dystonic events
- Upper endoscopy - may show esophagitis
Treatment
- Conservative (first line)
- Smaller, more frequent feedings
- Upright positioning after feeds (avoid car seat - worsens reflux)
- Thickened formula
- Medical
- Proton pump inhibitors (e.g., omeprazole 1 mg/kg/day in 2 divided doses) - episodes typically resolve within 3-4 weeks
- H2 blockers
- Surgical
- Nissen fundoplication for severe, refractory GERD unresponsive to medical therapy
Complete resolution of posturing with anti-reflux treatment confirms the diagnosis.
Key teaching point: In any infant presenting with "seizure-like" stiffening or arching - especially post-feed, with normal EEG, normal neurological exam - always consider Sandifer syndrome and actively look for GERD. - Tintinalli's Emergency Medicine, Table 138-3
This is a shared conversation. Sign in to Orris to start your own chat.