Anatomy of ear, with simpldiagram to draw
anatomy of the ear external middle inner structures
anatomy of the ear diagram labeled external middle inner
Anatomy of the Ear
1. External (Outer) Ear
| Structure | Description |
|---|---|
| Auricle (Pinna) | The visible, cartilage-based, funnel-shaped part that collects sound |
| External Auditory Canal (EAC) | ~2.5 cm S-shaped tube; lined with skin, ceruminous glands (wax) |
| Tympanic Membrane (Eardrum) | Thin, cone-shaped membrane; boundary between outer and middle ear; vibrates with sound |
2. Middle Ear (Tympanic Cavity)
| Structure | Description |
|---|---|
| Malleus (Hammer) | Ossicle attached directly to the tympanic membrane |
| Incus (Anvil) | Middle ossicle; connects malleus to stapes |
| Stapes (Stirrup) | Smallest bone in the body; footplate sits on the oval window |
| Oval Window | Membrane-covered opening to the inner ear; transmits vibrations from stapes |
| Round Window | Second membrane-covered opening; allows fluid pressure to dissipate |
| Eustachian Tube | Connects middle ear to nasopharynx; equalizes air pressure |
The ossicles act as a mechanical transformer, amplifying vibrations from air (low impedance) to fluid (high impedance) in the inner ear. (Bailey & Love, p. 771)
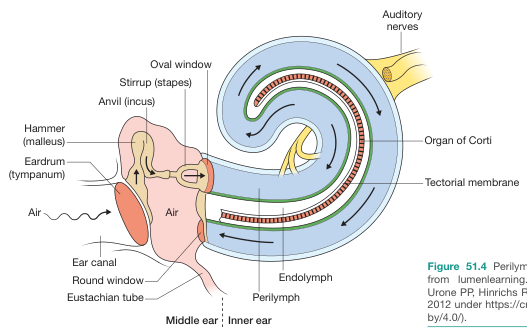
3. Inner Ear (Labyrinth)
- Spiral, snail-shaped structure; ~2.5 turns
- Contains three fluid-filled ducts:
- Scala vestibuli — filled with perilymph
- Scala tympani — filled with perilymph
- Scala media (cochlear duct) — filled with endolymph
- Organ of Corti — sits on the basilar membrane; contains inner and outer hair cells (mechanoreceptors)
- Tectorial membrane — overlies hair cells; deflects them during sound waves
- Auditory nerve (CN VIII) — carries signals to brainstem
- Semicircular canals (3 — anterior, posterior, lateral): detect rotational/angular movement
- Utricle and Saccule: detect linear acceleration and gravity (via otoliths)
Sound Transmission Pathway
Sound wave
↓
Pinna → EAC → Tympanic Membrane
↓
Malleus → Incus → Stapes
↓
Oval Window → Perilymph (scala vestibuli)
↓
Basilar Membrane vibration → Hair cells (Organ of Corti)
↓
Endolymph wave → Round Window (pressure relief)
↓
Auditory nerve (CN VIII) → Brainstem → Auditory Cortex
Simple Diagram to Draw
OUTER EAR MIDDLE EAR INNER EAR
________________ _______________ ___________
| | | | | |
| PINNA | | Malleus | | Cochlea |
| \ | | \ | | (snail |
| EAR |~~| Incus |~~| shape) |
| CANAL | | \ | | |
| | | Stapes ===|==| Oval Win |
|________________| | Eustachian | |___________|
↓ | Tube ↓ |
Eardrum | (throat) |
(tympanic |______________|
membrane)
- Draw a large C-shape (pinna) on the left
- Draw a short horizontal tube (EAC) going right
- Draw a slightly angled oval at the end = tympanic membrane
- Inside the middle ear box, sketch 3 tiny bones in an L/chain shape: hammer → anvil → stirrup
- The stirrup touches a small oval on the right wall = oval window
- To the right, draw a snail/spiral = cochlea
- Add a tube going down from the middle ear = Eustachian tube
- Label all parts
"MIS" — Malleus, Incus, Stapes (in order from eardrum inward) "3 S's" — Sound → Stirrup → Scala (cochlea)
Can you divide to surface anatomy, regional anatomy, gross anatomy, histology
ear surface anatomy auricle pinna landmarks
ear histology cochlea organ of corti hair cells tympanic membrane microscopic
ear surface anatomy auricle pinna labeled landmarks helix tragus
cochlea histology organ of Corti basilar membrane hair cells spiral ganglion
Anatomy of the Ear
1. Surface Anatomy
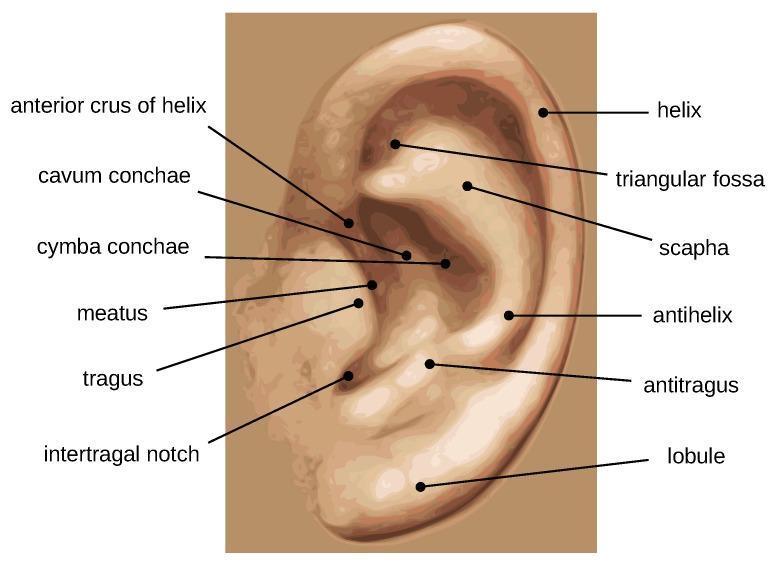
Auricle (Pinna) Landmarks
| Landmark | Description |
|---|---|
| Helix | Outer curved rim of the ear |
| Antihelix | Inner curved ridge, parallel to helix; divides into superior and inferior crura |
| Scapha | Groove/depression between helix and antihelix |
| Triangular Fossa | Depression between the two crura of the antihelix |
| Concha | Central bowl-shaped depression; divided into: Cymba conchae (upper) and Cavum conchae (lower) |
| Tragus | Small anterior projection overlying the ear canal opening |
| Antitragus | Small projection opposite the tragus |
| Intertragal Notch | Notch between tragus and antitragus |
| Lobule (Earlobe) | Inferior fleshy, non-cartilaginous part |
| External Auditory Meatus | The visible opening of the ear canal |
Simple Drawing Guide — Surface Anatomy
Helix (outer rim)
/
/ Triangular
| Fossa
| Antihelix
| /
|/ Scapha
( ) ← Concha (cymba above, cavum below)
|\
| Tragus Antitragus
|___|___|
Lobule
2. Regional Anatomy
A. External Ear
- Auricle: fibrocartilage skeleton (elastic cartilage) covered by skin; attached to skull by ligaments and muscles
- External Auditory Canal (EAC):
- Length: ~2.5 cm
- Outer 1/3: cartilaginous (soft), contains hair follicles + ceruminous (wax) glands
- Inner 2/3: bony (tympanic part of temporal bone), thinner skin, no glands
- Slightly S-shaped; straightened for otoscopy by pulling pinna up and back (adults) or down and back (children)
- Tympanic Membrane (Eardrum):
- Boundary between external and middle ear
- Diameter: ~9–10 mm; oriented obliquely (not perpendicular)
- Pars tensa (lower 2/3): taut, pearly grey — main functional part (Harrison's, p. 1036)
- Pars flaccida (upper 1/3): lax, above the short process of malleus — important site for cholesteatoma
B. Middle Ear (Tympanic Cavity)
- Air-filled cavity within the petrous part of temporal bone
- Walls (6 relations):
| Wall | Also Called | Key Content |
|---|---|---|
| Lateral | Membranous | Tympanic membrane |
| Medial | Labyrinthine | Oval window, round window, promontory |
| Anterior | Carotid | Eustachian tube opening, internal carotid artery |
| Posterior | Mastoid | Aditus to mastoid antrum, pyramid (stapedius) |
| Roof | Tegmental | Tegmen tympani (thin bone separating from middle cranial fossa) |
| Floor | Jugular | Internal jugular vein below |
- Ossicles: Malleus → Incus → Stapes (suspended by ligaments)
- Muscles: Tensor tympani (CN V3), Stapedius (CN VII — facial nerve)
- Eustachian Tube: 35–40 mm long; connects to nasopharynx; normally closed, opens on swallowing/yawning
- Chorda tympani: branch of CN VII crossing the middle ear; carries taste from anterior 2/3 tongue
C. Inner Ear (Bony & Membranous Labyrinth)
| Part | Sub-structures |
|---|---|
| Vestibule | Central chamber; connects cochlea anteriorly, semicircular canals posteriorly |
| Cochlea | 2.5 spiral turns around the modiolus; contains organ of hearing |
| Semicircular Canals | 3 canals (anterior, posterior, lateral) at right angles to each other; ampullae at one end |
- Utricle & Saccule (in vestibule): linear acceleration/gravity detection (otolith organs)
- Semicircular ducts (in canals): angular/rotational acceleration
- Cochlear duct (scala media): hearing
3. Gross Anatomy
Cochlea (Cross-Section — Gross)
___________
/ \
| Scala | ← Perilymph
| Vestibuli |
\___________/
/ \
| Scala | ← Endolymph (cochlear duct)
| Media |
\___________/
/ \
| Scala | ← Perilymph
| Tympani |
\___________/
- Modiolus: central bony axis of cochlea; carries the spiral ganglion and cochlear nerve fibers
- Helicotrema: apex of cochlea where scala vestibuli and scala tympani communicate
- Oval window: stapes footplate inserts here → scala vestibuli
- Round window: base of scala tympani; covered by secondary tympanic membrane; acts as pressure relief
Ossicles — Gross Features
| Bone | Gross Feature | Size |
|---|---|---|
| Malleus | Handle embedded in tympanic membrane; head articulates with incus | ~8 mm |
| Incus | Body + short process (posterior) + long process (medial, articulates with stapes) | — |
| Stapes | Head, two crura (anterior/posterior), footplate in oval window | ~3 mm — smallest bone in the body |
Tympanic Membrane — Gross
- Umbo: central cone-shaped depression; tip of malleus handle
- Light reflex: cone of light seen inferoanteriorly on otoscopy (5 o'clock in right, 7 o'clock in left)
- Annulus: fibrocartilaginous ring anchoring TM to temporal bone
Internal Acoustic Meatus (IAM)
- Canal in petrous bone transmitting:
- CN VIII (vestibulocochlear): cochlear + superior/inferior vestibular divisions
- CN VII (facial nerve)
- Labyrinthine artery (branch of AICA)
4. Histology
A. Tympanic Membrane — 3 Layers
| Layer | Tissue |
|---|---|
| Outer (epithelial) | Stratified squamous epithelium (continuation of EAC skin) |
| Middle (fibrous) | Radial + circular collagen fibers (pars tensa); absent in pars flaccida |
| Inner (mucosal) | Simple squamous/cuboidal epithelium (continuation of middle ear mucosa) |
B. External Auditory Canal
- Outer 1/3: keratinizing stratified squamous epithelium + hair follicles + sebaceous glands + ceruminous glands (modified apocrine sweat glands producing cerumen/wax)
- Inner 2/3: thin stratified squamous epithelium directly over periosteum; no glands
C. Eustachian Tube
- Pseudostratified ciliated columnar epithelium (respiratory type) with goblet cells
- Cilia beat toward nasopharynx → mucus clearance from middle ear
D. Cochlea — Key Histological Layers
ORGAN OF CORTI (on Basilar Membrane)
________________________________________
| Tectorial | ← Gelatinous membrane overlying hair cells
| Membrane |
|_____________|
| Outer Hair | ← 3 rows; active amplification (electromotility)
| Cells (3) |
|_____________|
| Inner Hair | ← 1 row; primary sensory transduction (~95% of afferent fibers)
| Cells (1) |
|_____________|
| Basilar | ← Stiff at base (high freq), flexible at apex (low freq)
| Membrane |
|_____________|
| Structure | Histology |
|---|---|
| Inner hair cells | Flask-shaped; 1 row; ~3,500; stereocilia on apical surface; synapse with 95% of cochlear nerve fibers |
| Outer hair cells | Cylindrical; 3 rows; ~12,000; electromotile (prestin motor protein); amplify basilar membrane movement |
| Tectorial membrane | Acellular gelatinous matrix (collagen + proteoglycans); overlies hair cell stereocilia |
| Basilar membrane | Fibrous; tonotopic: narrow/stiff at base (20,000 Hz) → wide/flexible at apex (20 Hz) |
| Stria vascularis | Lateral wall; highly vascularized; maintains endolymphatic potential (+80 mV) and endolymph ionic composition (high K⁺) |
| Spiral ganglion | Cell bodies of bipolar neurons in modiolus; Type I (95%, myelinated, IHC) and Type II (5%, unmyelinated, OHC) |
| Reissner's membrane | Single-cell layer separating scala vestibuli from scala media; ion/fluid transport |
E. Vestibular Sensory Epithelium
| Structure | Cell Type | Function |
|---|---|---|
| Crista ampullaris (semicircular canals) | Hair cells + supporting cells; covered by cupula (gelatinous mass) | Detects angular rotation |
| Macula utriculi & sacculi | Hair cells + supporting cells; covered by otolithic membrane (contains calcium carbonate crystals = otoliths/otoconia) | Detects linear acceleration & gravity |
Summary Table
| Division | Focus | Key Structures |
|---|---|---|
| Surface Anatomy | Visible external landmarks | Helix, antihelix, tragus, concha, lobule |
| Regional Anatomy | Spatial zones & relations | Outer/middle/inner ear; walls of tympanic cavity; IAM |
| Gross Anatomy | Macroscopic structure | Ossicles, cochlear turns, oval/round windows, umbo |
| Histology | Microscopic tissue | Organ of Corti, hair cells, stria vascularis, otoliths |
physiology, biochem, pathology, micro, clinical presentation, medine and pharma related to rar
ear physiology sound transduction cochlea vestibular mechanism hearing
ear pathology otitis media cholesteatoma otosclerosis Meniere's disease
ear biochemistry endolymph perilymph potassium ion channels prestin electromotility
ear microbiology otitis media organisms Pseudomonas Streptococcus otitis externa
otitis media tympanic membrane perforation pathology clinical
The Ear — Complete Multi-Disciplinary Overview
1. Physiology
A. Physiology of Hearing (Mechanotransduction)
| Step | Event |
|---|---|
| 1 | Sound enters EAC → vibrates tympanic membrane |
| 2 | Ossicles (malleus → incus → stapes) amplify and transmit vibration |
| 3 | Stapes footplate pushes oval window → pressure wave in perilymph (scala vestibuli) |
| 4 | Traveling wave propagates along basilar membrane |
| 5 | Basilar membrane displaces → stereocilia of hair cells bend against tectorial membrane |
| 6 | K⁺ channels open (mechanically gated) → depolarization of hair cells |
| 7 | Glutamate released → synapse with cochlear nerve (CN VIII) → auditory cortex |
- Without the ossicular chain, 99.9% of sound energy would be reflected at the air-fluid interface
- The eardrum + ossicles boost sound energy ~200-fold before it reaches the inner ear (Harrison's, p. 1019)
- Achieved by: Area ratio (TM vs. oval window = 17:1) + Lever action of ossicles
Base of cochlea → High frequency (20,000 Hz) → narrow, stiff
Apex of cochlea → Low frequency (20 Hz) → wide, flexible
- Loud sound → CN VIII → brainstem → CN VII (stapedius) + CN V3 (tensor tympani)
- Muscles stiffen ossicular chain → attenuates loud sounds → protects inner ear
B. Physiology of Balance (Vestibular System)
| Organ | Stimulus | Mechanism |
|---|---|---|
| Semicircular canals | Angular/rotational acceleration | Endolymph lags → cupula deflects → hair cells bend |
| Utricle | Horizontal linear acceleration | Otoliths shift → macula deforms |
| Saccule | Vertical linear acceleration + gravity | Otoliths shift → macula deforms |
- Head moves → vestibular signal → compensatory eye movement in opposite direction
- Keeps visual field stable during head movement
2. Biochemistry
A. Endolymph vs. Perilymph Composition
| Feature | Endolymph | Perilymph |
|---|---|---|
| Location | Scala media, membranous labyrinth | Scala vestibuli, scala tympani |
| K⁺ | High (~150 mEq/L) | Low (~5 mEq/L) |
| Na⁺ | Low (~1 mEq/L) | High (~140 mEq/L) |
| Resembles | Intracellular fluid | Extracellular fluid/CSF |
| Maintained by | Stria vascularis | Filtration from blood/CSF |
B. Endocochlear Potential (EP)
- Stria vascularis generates a +80 mV resting potential in endolymph
- This is the driving force for K⁺ to rush into hair cells when stereocilia channels open
- Essential for mechanotransduction — loss of EP = sensorineural deafness
C. Hair Cell Mechanotransduction — Ion Channels
Stereocilia deflect toward tallest → tip links stretch
→ MET channels (MYO7A, TMHS, LHFPL5) open
→ K⁺ + Ca²⁺ influx → depolarization
→ Voltage-gated Ca²⁺ channels open at base
→ Vesicle release (glutamate) → CN VIII
D. Prestin (SLC26A5) — Outer Hair Cell Motor
- Prestin is a piezoelectric motor protein in OHC lateral wall
- Changes cell length in response to voltage changes (electromotility)
- Amplifies basilar membrane movement up to 1000×
- Loss of prestin → 40–60 dB hearing loss
E. Cerumen (Earwax) Biochemistry
- Produced by ceruminous (apocrine) glands in outer EAC
- Composition: long-chain fatty acids, alcohols, squalene, lysozyme, IgA
- Functions: antimicrobial, lubricating, waterproofing, acidic pH (6.1) → inhibits bacterial/fungal growth
3. Pathology
A. Conductive Hearing Loss (CHL) — Outer/Middle Ear
| Disease | Pathology |
|---|---|
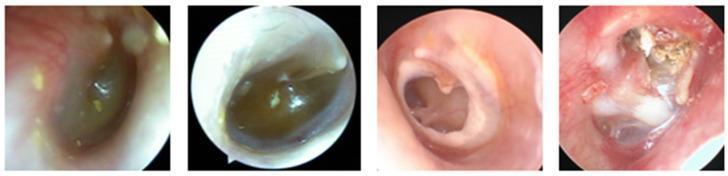
| Otitis Media with Effusion (OME) | Serous fluid in middle ear; Eustachian tube dysfunction; amber TM, air-fluid level |
| Acute Otitis Media (AOM) | Bacterial/viral infection; hyperemic, bulging, erythematous TM; purulent effusion |
| Chronic Suppurative OM (CSOM) | Persistent TM perforation + discharge >6 weeks |
| Cholesteatoma | Keratinizing squamous epithelium invades middle ear; produces collagenases → erodes ossicles and bone; pearly white mass |
| Otosclerosis | Abnormal remodeling of stapes footplate (new spongy bone); stapes fixation; autosomal dominant; worse in pregnancy |
| Tympanosclerosis | Calcification/hyalinization of TM fibrous layer; white plaques on TM |
| Ossicular erosion | Incus long process most commonly eroded (avascular) |
B. Sensorineural Hearing Loss (SNHL) — Inner Ear/Nerve
| Disease | Pathology |
|---|---|
| Presbycusis (ARHL) | Age-related; loss of outer hair cells at cochlear base first → high-frequency loss |
| Noise-induced | Mechanical damage to OHC stereocilia; 4 kHz notch on audiogram |
| Ménière's Disease | Endolymphatic hydrops (excess endolymph); hair cell and nerve damage |
| Acoustic Neuroma (Vestibular Schwannoma) | Benign Schwann cell tumor of CN VIII (vestibular division); progressive SNHL + tinnitus + vertigo |
| Ototoxicity | Drug-induced OHC death (see Pharmacology) |
C. Other Pathologies
| Disease | Pathology |
|---|---|
| Otitis Externa | Infection of EAC skin; "swimmer's ear" |
| Malignant (Necrotizing) OE | Pseudomonas osteomyelitis of temporal bone; in diabetics/immunocompromised |
| Barotrauma | Pressure injury to TM/middle ear; TM hemorrhage or perforation |
| Perilymph Fistula | Tear in oval/round window membranes; perilymph leaks; SNHL + vertigo |
4. Microbiology
Acute Otitis Media (AOM)
| Organism | Notes |
|---|---|
| Streptococcus pneumoniae | Most common cause overall; most severe |
| Haemophilus influenzae (non-typeable) | Common; often β-lactamase producing |
| Moraxella catarrhalis | Common; almost always β-lactamase positive |
| Viral (RSV, rhinovirus) | Precedes bacterial AOM; disrupts Eustachian tube |
Otitis Externa (Acute)
| Organism | Notes |
|---|---|
| Pseudomonas aeruginosa | Most common; associated with water exposure |
| Staphylococcus aureus | Second most common |
| Aspergillus / Candida | Otomycosis; seen post-antibiotic use |
Malignant Otitis Externa
- Pseudomonas aeruginosa almost exclusively
- Osteomyelitis of skull base; can involve CN VII → facial palsy
- Risk: Diabetics, elderly, HIV+
Chronic Suppurative OM
- Polymicrobial: Pseudomonas aeruginosa + S. aureus (including MRSA) + anaerobes
Fungal OE (Otomycosis)
| Organism | Appearance |
|---|---|
| Aspergillus niger | Black spores in canal |
| Candida albicans | White debris |
5. Clinical Presentation
Hearing Loss
| Type | Causes | Weber | Rinne |
|---|---|---|---|
| Conductive | OM, otosclerosis, wax, cholesteatoma | Lateralizes to affected ear | Negative (BC > AC) |
| Sensorineural | Presbycusis, noise, Ménière's | Lateralizes to normal ear | Positive (AC > BC, but reduced) |
| Mixed | CSOM with cochlear involvement | Variable | Negative |
Ménière's Disease — Triad
"VHT": Vertigo (episodic, 20 min–24 hrs) + Hearing loss (fluctuating, low-frequency SNHL) + Tinnitus (low-pitched roaring) ± aural fullness
Acute Otitis Media
- Ear pain (otalgia), fever, irritability (children)
- Otoscopy: red, bulging, opaque TM; loss of light reflex
- May progress to: TM perforation (pain relief), mastoiditis, meningitis
Otitis Externa
- Intense itching → pain → discharge
- Tragal tenderness and pain on jaw movement (pathognomonic)
- Canal edematous, erythematous, debris-filled
Acoustic Neuroma
- Unilateral SNHL + tinnitus + imbalance
- Absent corneal reflex (CN V involvement)
- Diagnosed on MRI with gadolinium (IAM)
Otosclerosis
- Progressive conductive hearing loss in young adult
- Family history; worsens in pregnancy (estrogen accelerates bone remodeling)
- Otoscopy: Schwartze sign (flamingo pink blush through TM — active otospongiosis)
- Audiogram: Carhart's notch at 2000 Hz
Cholesteatoma
- Foul-smelling discharge + hearing loss
- Otoscopy: pearly white mass in pars flaccida/posterior-superior quadrant
- Complications: ossicular erosion, labyrinthine fistula, facial palsy, meningitis, brain abscess
6. Medicine (Clinical Medicine)
Audiological Tests
| Test | What It Measures |
|---|---|
| Pure Tone Audiometry (PTA) | Hearing threshold across frequencies; air and bone conduction |
| Tympanometry | Middle ear compliance/pressure; detects effusion, perforation, otosclerosis |
| Otoacoustic Emissions (OAEs) | OHC function; used in neonatal screening |
| Auditory Brainstem Response (ABR) | Cochlear nerve + brainstem pathway integrity |
| Caloric testing | Vestibular function of each ear separately |
| VEMP (Vestibular Evoked Myogenic Potential) | Saccule (cVEMP) and utricle (oVEMP) function |
Tympanogram Types
| Type | Pattern | Meaning |
|---|---|---|
| A | Normal peak at 0 daPa | Normal middle ear |
| As | Shallow peak | Otosclerosis, tympanosclerosis |
| Ad | Tall/wide peak | TM flaccidity, ossicular discontinuity |
| B | Flat, no peak | Middle ear effusion, perforation |
| C | Peak shifted negative | Eustachian tube dysfunction |
Complications of OM
- Mastoiditis (most common)
- Facial palsy (CN VII in Fallopian canal)
- Labyrinthitis → SNHL
- Petrositis (Gradenigo's syndrome: deep ear pain + CN VI palsy + retro-orbital pain)
- Meningitis, brain abscess, lateral sinus thrombosis, subdural empyema
7. Pharmacology
A. Topical Ear Drops
| Drug | Use |
|---|---|
| Ciprofloxacin + hydrocortisone | Otitis externa; AOM with perforation (safe — non-ototoxic) |
| Gentamicin drops | Otitis externa; AVOID in TM perforation (ototoxic) |
| Clotrimazole / nystatin | Otomycosis |
| Acetic acid (2%) | OE; lowers pH, antibacterial/antifungal |
| Carbamide peroxide | Cerumenolysis (wax softening) |
B. Systemic Antibiotics for OM
| Drug | Indication |
|---|---|
| Amoxicillin (high dose 80–90 mg/kg/day) | First-line AOM |
| Amoxicillin-clavulanate | AOM failing amoxicillin; β-lactamase producing organisms |
| Cefdinir / Cefuroxime | Penicillin allergy (non-severe) |
| Azithromycin / Clindamycin | Severe penicillin allergy |
C. Ototoxic Drugs (Critical!)
| Drug Class | Examples | Mechanism | Effect |
|---|---|---|---|
| Aminoglycosides | Gentamicin, tobramycin, amikacin | ROS generation → OHC apoptosis | SNHL (irreversible); gentamicin also vestibulotoxic |
| Loop diuretics | Furosemide, ethacrynic acid | Disrupts stria vascularis ion transport | Usually reversible SNHL |
| Platinum chemotherapy | Cisplatin, carboplatin | ROS + OHC apoptosis | Irreversible SNHL; high-frequency first |
| Quinine / Chloroquine | Antimalarials | Unknown; hair cell damage | Reversible tinnitus + SNHL |
| Salicylates (high dose) | Aspirin | Reversible OHC dysfunction (prestin inhibition) | Reversible tinnitus; SNHL at >3 g/day |
| Vancomycin | Alone: low risk; with aminoglycosides: synergistic ototoxicity | — | Monitor levels |
Mnemonic — Ototoxic drugs: "AGAIN" Aminoglycosides · General anesthetics (loop diuretics) · Antimalarials · Indomethacin-like (salicylates) · Neoplastic agents (cisplatin)
D. Ménière's Disease Treatment
| Approach | Drug/Intervention |
|---|---|
| Acute vertigo | Betahistine, prochlorperazine, diazepam |
| Long-term prophylaxis | Betahistine (histamine H1 agonist/H3 antagonist; improves cochlear microcirculation) |
| Reduce endolymph | Low-sodium diet + hydrochlorothiazide/acetazolamide |
| Intratympanic | Gentamicin (ablates vestibular hair cells) or dexamethasone |
| Surgery | Endolymphatic sac decompression; labyrinthectomy; vestibular neurectomy |
E. Otosclerosis Treatment
- Sodium fluoride: slows active otospongiosis (inhibits osteoclast activity)
- Bisphosphonates: used investigationally
- Definitive: Stapedectomy / Stapedotomy — surgical removal/laser perforation of stapes
F. Vestibular Suppressants
| Drug | Class | Use |
|---|---|---|
| Meclizine / Dimenhydrinate | Antihistamine | Motion sickness, acute vertigo |
| Prochlorperazine | Phenothiazine | Acute vertigo, N&V |
| Diazepam / Lorazepam | Benzodiazepine | Acute severe vertigo (short-term only) |
| Scopolamine | Anticholinergic | Motion sickness (transdermal patch) |
Summary Overview Table
| Domain | Key Points |
|---|---|
| Physiology | Impedance matching (×200 amplification); tonotopy; K⁺-driven mechanotransduction; VOR |
| Biochemistry | Endolymph = high K⁺; EP = +80 mV; prestin motor; cerumen = antibacterial |
| Pathology | CHL (OM, otosclerosis, cholesteatoma) vs SNHL (presbycusis, noise, Ménière's) |
| Microbiology | AOM: S. pneumoniae; OE: Pseudomonas; malignant OE: Pseudomonas in diabetics |
| Clinical | Weber/Rinne tests; tympanogram types; Ménière's triad; Gradenigo's syndrome |
| Medicine | PTA, OAE, ABR, tympanometry; OM complications (intratemporal + intracranial) |
| Pharmacology | Ototoxins (aminoglycosides, cisplatin, loop diuretics); Betahistine for Ménière's; amoxicillin for AOM |
Canyou do same for nose
nose anatomy nasal cavity septum turbinates sinuses labeled diagram
nasal histology respiratory epithelium olfactory mucosa goblet cells
The Nose — Complete Multi-Disciplinary Overview
1. Surface Anatomy
External Nose Landmarks
| Landmark | Description |
|---|---|
| Root (Radix) | Most superior part; between the eyes |
| Dorsum | Bridge of the nose; bony upper 2/3 + cartilaginous lower 1/3 |
| Apex (Tip) | Inferiormost point |
| Ala (nasi) | Wing-shaped lateral walls of the nostril; fibro-fatty tissue (no cartilage) |
| Nostril (Naris) | External opening; oval-shaped |
| Columella | Skin-covered strip separating the two nostrils |
| Nasolabial fold | Crease between ala and upper lip |
| Nasion | Bony depression at nasal root (frontonasal junction) |
| Rhinion | Most anterior projecting point of the nasal dorsum |
| Subnasale | Junction of columella with upper lip |
Simple Drawing — External Nose
Nasion (top)
|
_____|_____
| Dorsum |
| |
|___ Tip __/
/ Columella \
/ \
Ala(L) Naris Ala(R)
|
Subnasale
2. Regional Anatomy
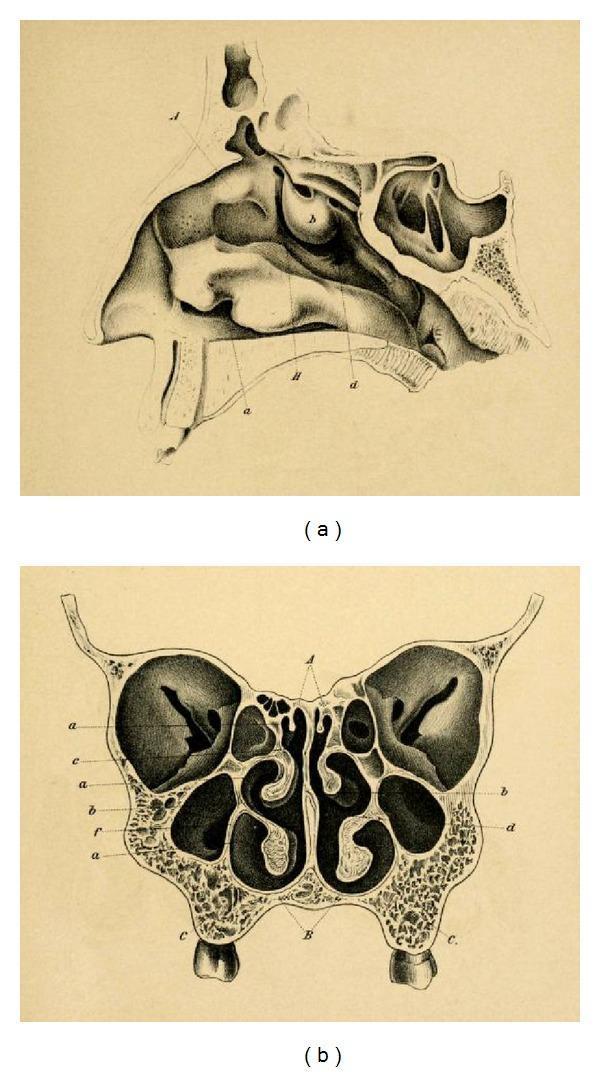
A. Nasal Cavity
| Wall | Structure |
|---|---|
| Roof | Cribriform plate of ethmoid (olfactory nerve fibers pass through) |
| Floor | Hard palate (palatine process of maxilla + horizontal plate of palatine bone) |
| Medial | Nasal septum (perpendicular plate of ethmoid + vomer + septal cartilage) |
| Lateral | Turbinates + lateral wall structures |
- Upper bony part: perpendicular plate of ethmoid
- Lower bony part: vomer
- Anterior cartilaginous: quadrilateral (septal) cartilage
- Common site for septal deviation (most common anatomical variation)
| Turbinate | Meatus Beneath | Drainage |
|---|---|---|
| Inferior turbinate | Inferior meatus | Nasolacrimal duct |
| Middle turbinate | Middle meatus | Frontal sinus, maxillary sinus, anterior ethmoid |
| Superior turbinate | Superior meatus | Posterior ethmoid, sphenoid sinus |
The ostiomeatal complex (OMC) — the area under the middle turbinate — is the key functional drainage site; obstruction here causes sinusitis.
- Anterior entry zone just inside nostril; contains vibrissae (nasal hairs) filtering large particles
- Narrowest part of the airway (~90° angle between septum and upper lateral cartilage)
- Most common site of nasal airflow resistance
B. Paranasal Sinuses
| Sinus | Location | Drainage | Development |
|---|---|---|---|
| Maxillary | Maxilla (cheekbone) | Middle meatus (via ostium ~4 mm) | Present at birth |
| Ethmoid | Between orbit and nasal septum | Anterior cells → middle meatus; posterior cells → superior meatus | Present at birth |
| Frontal | Frontal bone above orbit | Middle meatus (via frontal recess) | Visible ~age 4–5 |
| Sphenoid | Body of sphenoid bone | Superior meatus / sphenoethmoidal recess | Develops in teens |
Frontal sinus absent in up to 10% of normal individuals (Murray & Nadel, p. 1613)
- Force dissipation in facial trauma
- Vocal resonance
- Mucus production and immune surveillance
- Contribution to facial aesthetics
C. Blood Supply — Key for Epistaxis
| Vessel | Origin | Area Supplied |
|---|---|---|
| Sphenopalatine artery (SPA) | External carotid → internal maxillary | Majority of nasal cavity; posterior nasal cavity |
| Anterior ethmoid artery | Internal carotid → ophthalmic | Superior/anterior nasal cavity, ethmoid roof |
| Posterior ethmoid artery | Internal carotid → ophthalmic | Posterior superior nasal cavity |
| Greater palatine artery | External carotid | Floor of nasal cavity |
| Superior labial artery | External carotid → facial | Anterior septum (Little's area) |
- Anteroinferior septum where all 5 vessels anastomose
- Site of 90% of anterior nosebleeds
D. Nerve Supply
| Nerve | Origin | Area |
|---|---|---|
| Olfactory nerve (CN I) | Cribriform plate | Olfactory epithelium (superior nasal cavity) |
| Ophthalmic (V1) | Trigeminal | Anterior nasal cavity (anterior ethmoidal nerve) |
| Maxillary (V2) | Trigeminal | Posterior nasal cavity (nasopalatine, posterior nasal nerves) |
| Autonomic (parasympathetic) | CN VII → pterygopalatine ganglion | Glandular secretion, vascular tone |
| Sympathetic | T1 superior cervical ganglion | Vasoconstriction → nasal decongestion |
3. Gross Anatomy
Nasal Skeleton
BONY FRAMEWORK CARTILAGINOUS FRAMEWORK
___________________ ________________________
| Nasal bones (2) | | Upper lateral |
| Frontal process | | cartilages (2) |
| of maxilla | | Lower lateral (alar) |
|___________________| | cartilages (2) |
| Septal cartilage |
| Sesamoid cartilages |
|________________________|
- Nasion to rhinion: bony dorsum (nasal bones)
- Rhinion to tip: cartilaginous dorsum (upper lateral cartilages)
- Tip: defined by lower lateral (greater alar) cartilages — medial + lateral crura
Turbinate Gross Appearance
- Scroll-shaped bony projections covered by thick, vascular mucosa
- Erectile tissue (venous sinusoids) → nasal cycle: alternating congestion/decongestion every 2–6 hours
- Inferior turbinate: largest; most significant in nasal obstruction
Choanae
- Posterior opening of each nasal cavity into the nasopharynx
- Width ~1 cm in adults
- Choanal atresia: congenital bony/membranous obstruction → neonatal respiratory distress
4. Histology
A. Nasal Mucosa — Two Zones
| Layer | Detail |
|---|---|
| Epithelium | Pseudostratified ciliated columnar epithelium (PCCE) + goblet cells |
| Lamina propria | Rich in seromucinous glands, venous sinusoids, mast cells, eosinophils |
| Submucosa | Erectile venous tissue (cavernous sinusoids), especially inferior turbinate |
- Ciliated columnar cells (most abundant): ~200 cilia/cell; beat 1000×/min; mucociliary clearance
- Goblet cells: mucin-secreting; form upper gel layer of mucus blanket
- Basal cells: stem cells; regenerate epithelium
- Brush cells: chemosensory
- Club cells (formerly Clara): detoxification
| Cell Type | Function |
|---|---|
| Olfactory receptor neurons (ORNs) | Bipolar neurons; dendrites end in olfactory knob with cilia; axons → CN I |
| Sustentacular (supporting) cells | Columnar; metabolic support, detoxification |
| Basal cells | Stem cells; ORNs regenerate every ~60 days |
| Bowman's glands | Serous glands in lamina propria; wash odorants across olfactory epithelium |
B. Nasal Glands (Seromucinous)
- Seromucous glands: serous + mucous components; produce the sol layer (periciliary fluid) and gel layer (mucus blanket)
- Innervated by parasympathetic fibers (CN VII → pterygopalatine ganglion → VIP/ACh)
- Stimulation → watery secretion (rhinorrhea)
C. Paranasal Sinus Histology
- Lined by ciliated pseudostratified columnar epithelium (thinner than nasal mucosa)
- Fewer goblet cells and glands than nasal cavity
- Cilia beat toward ostium → mucociliary drainage into nasal cavity (Murray & Nadel, p. 1613)
5. Physiology
A. Nasal Airflow & Conditioning
- Nose handles ~90% of inspired air at rest
- Functions: Filter, Warm, Humidify
| Function | Mechanism |
|---|---|
| Filtration | Vibrissae (>10 µm); turbulent airflow + mucociliary blanket (2–10 µm); mucosal IgA (<2 µm) |
| Warming | Countercurrent heat exchange via turbinate vasculature → air reaches ~34°C by posterior nasal cavity |
| Humidification | Mucosal evaporation → ~75–80% relative humidity achieved |
B. Mucociliary Clearance (MCC)
- Two-layer mucus blanket:
- Sol layer (periciliary, low viscosity): cilia beat freely within this
- Gel layer (upper, viscous): traps particles and pathogens
- Ciliary beat: effective stroke (forward, moves gel layer) + recovery stroke (backward, within sol layer)
- Clearance rate: ~6 mm/min; mucus blanket replaced every 10–15 minutes
- Entire nasal mucus cleared in ~30 minutes to nasopharynx → swallowed
C. Nasal Cycle
- Alternating unilateral nasal congestion/decongestion (~2–7 hours cycle)
- Mediated by sympathetic tone controlling erectile venous sinusoids
- Total nasal resistance remains relatively constant (one side opens as other closes)
D. Olfaction (Smell)
Odorant molecule (volatile, hydrophobic)
↓
Dissolves in Bowman's gland secretion
↓
Binds olfactory receptor proteins (G-protein coupled)
↓
Adenylyl cyclase → ↑cAMP
↓
cAMP-gated Na⁺/Ca²⁺ channels open → depolarization
↓
Action potential → olfactory nerve (CN I) → cribriform plate
↓
Olfactory bulb → olfactory tract → piriform cortex, amygdala, hypothalamus
(No thalamic relay — direct limbic access → explains emotion-smell link)
E. Sneezing Reflex
- Trigger: irritation of nasal mucosa → CN V afferents → brainstem sneeze center
- Response: deep inspiration → glottis closes → explosive expiration (up to 160 km/h)
- Clears nasal cavity of irritants
6. Biochemistry
A. Nasal Mucus Composition
| Component | Function |
|---|---|
| Water (~95%) | Maintains sol/gel layer viscosity |
| Mucins (MUC5B, MUC5AC) | Gel-forming glycoproteins; trap pathogens/particles |
| Lysozyme | Cleaves bacterial cell wall (peptidoglycan) |
| Lactoferrin | Binds free iron → bacteriostatic |
| Secretory IgA (sIgA) | Prevents microbial adherence to mucosa |
| Defensins | Antimicrobial peptides; disrupt microbial membranes |
| Peroxidases | Generate reactive oxygen species → antimicrobial |
B. Olfactory Receptor Biochemistry
- ~400 functional olfactory receptor (OR) genes in humans (largest gene family; ~3% of genome)
- Each ORN expresses one type of OR (one-receptor-one-neuron rule)
- OR activation → Golf protein → adenylyl cyclase III → ↑cAMP → CNGA2 channels open → Na⁺/Ca²⁺ influx
- Ca²⁺ also activates Cl⁻ channels → amplification
C. Nitric Oxide (NO) in the Nose
- Paranasal sinuses (especially maxillary) produce high concentrations of NO
- Nasal NO: ~250 ppb (highest in body)
- Functions: vasodilation, ciliary beat stimulation, antimicrobial, bronchodilation in lower airways
- Reduced nasal NO = marker of primary ciliary dyskinesia (PCD)
D. Inflammatory Mediators in Allergic Rhinitis
| Mediator | Source | Effect |
|---|---|---|
| Histamine | Mast cells | Sneezing, itching, rhinorrhea, vasodilatation |
| Leukotrienes (LTC4/D4) | Mast cells, eosinophils | Mucosal edema, hypersecretion |
| PGD2 | Mast cells | Nasal congestion |
| IL-4, IL-5, IL-13 | Th2 cells | IgE switching, eosinophil recruitment, mucus hypersecretion |
| TSLP, IL-33, IL-25 | Epithelial cells | Alarmin cascade → innate type 2 inflammation |
7. Pathology
A. Inflammatory Conditions
| Condition | Key Pathology |
|---|---|
| Allergic Rhinitis | IgE-mediated; mast cell degranulation; eosinophilic infiltrate in lamina propria |
| Chronic Rhinosinusitis (CRS) | Persistent mucosal inflammation >12 weeks; eosinophilic (with polyps) or neutrophilic (without) |
| Nasal Polyps | Benign pedunculated masses from middle meatus; oedematous stroma + eosinophils; associated with asthma, aspirin sensitivity (Samter's triad) |
| Acute Rhinosinusitis | Mucosal edema, neutrophilic infiltrate, sinus ostia obstruction |
B. Structural Pathology
| Condition | Description |
|---|---|
| Deviated Nasal Septum (DNS) | Most common; causes unilateral obstruction; may be congenital or post-traumatic |
| Turbinate Hypertrophy | Inferior turbinate enlargement; commonest cause of nasal obstruction |
| Concha Bullosa | Pneumatization of middle turbinate; may obstruct OMC |
| Choanal Atresia | Congenital bony/membranous obstruction of choana; bilateral = neonatal emergency |
| Epistaxis | Anterior (Little's area, 90%) vs posterior (SPA territory); dangerous in posterior |
C. Destructive & Neoplastic
| Condition | Key Features |
|---|---|
| Inverted Papilloma | Benign but locally aggressive; endophytic growth; associated with HPV 6/11; risk of malignant transformation; arises from lateral wall |
| Nasopharyngeal Carcinoma (NPC) | Associated with EBV; undifferentiated type; arises in fossa of Rosenmüller |
| Squamous Cell Carcinoma | Most common malignant nasal tumor |
| Esthesioneuroblastoma | Rare; arises from olfactory neuroepithelium; Kadish staging |
| Wegener's (GPA) | Granulomatous vasculitis; saddle-nose deformity; c-ANCA positive |
| Midline Granuloma (NK/T-cell lymphoma) | Destructive; EBV-associated |
D. Rhinosinusitis — Diagnostic Criteria (Murray & Nadel, p. 1613)
| Type | Duration | Key Features |
|---|---|---|
| Acute rhinosinusitis | <4 weeks | Clinical diagnosis; purulent discharge + facial pain/pressure + nasal obstruction |
| Subacute | 4–12 weeks | Persistent without resolution |
| Chronic rhinosinusitis | >12 weeks | Requires objective evidence (endoscopy or CT) |
| Recurrent acute | ≥4 episodes/year | Each <4 weeks with symptom-free intervals |
8. Microbiology
Acute Rhinosinusitis (Bacterial)
| Organism | Notes |
|---|---|
| Streptococcus pneumoniae | Most common (~30–40%); most virulent |
| Haemophilus influenzae (non-typeable) | ~20–30%; β-lactamase producing strains common |
| Moraxella catarrhalis | ~10–20%; almost always β-lactamase positive |
| Anaerobes | Dental sinusitis (maxillary sinus) — Bacteroides, Fusobacterium |
| Viral | Rhinovirus, coronavirus, influenza — precede 90% of bacterial ARS |
Chronic Rhinosinusitis
- Polymicrobial: Staphylococcus aureus (dominant, including MRSA), coagulase-negative staph, Pseudomonas, anaerobes
- S. aureus superantigen hypothesis: drives eosinophilic inflammation in CRS with polyps
Fungal Sinusitis
| Type | Organism | Notes |
|---|---|---|
| Allergic fungal sinusitis | Aspergillus, Bipolaris, Curvularia | Non-invasive; allergic mucin; eosinophilia; IgE elevated |
| Invasive fungal sinusitis | Aspergillus, Mucor/Rhizopus | Immunocompromised/diabetic; angioinvasive; black eschar; emergency |
| Mycetoma (fungal ball) | Aspergillus | Maxillary sinus; non-immunocompromised |
Rhinoscleroma
- Caused by Klebsiella rhinoscleromatis
- Chronic granulomatous infection; causes nasal sclerosis
- Mikulicz cells (foamy macrophages with Russell bodies) on histology
9. Clinical Presentation
Symptom Framework — "PODS"
Purulent discharge · Obstruction · Dysosmia · Sinus pain/pressure/fullness
Key Presentations
| Condition | Cardinal Symptoms |
|---|---|
| Allergic Rhinitis | Sneezing (paroxysmal), watery rhinorrhea, nasal itch, nasal obstruction, conjunctivitis; seasonal or perennial |
| Acute Sinusitis | Facial pain/pressure (worsens on bending), purulent discharge, nasal obstruction, fever |
| Chronic Sinusitis | Persistent obstruction, chronic purulent discharge, hyposmia, postnasal drip, halitosis |
| Nasal Polyps | Bilateral nasal obstruction, hyposmia/anosmia, CRS symptoms |
| DNS | Unilateral obstruction, snoring, mouth breathing |
| Epistaxis | Anterior: bleeding from anterior septum (Little's area); Posterior: severe, bilateral, may need hospitalization |
| NPC | Painless neck mass (lymph node), epistaxis, unilateral serous otitis media, CN palsy |
Anterior Rhinoscopy (Clinical Exam)
- Inspect: septum deviation, turbinate hypertrophy, mucosa color/edema, polyps, discharge
- Allergic salute: horizontal nasal crease from repeated upward wiping
- Allergic shiners: infraorbital darkening from venous congestion
Nasal Endoscopy (Key Findings)
| Finding | Significance |
|---|---|
| Purulent discharge from middle meatus | Anterior group sinusitis |
| Polyps from middle meatus | CRS with polyps, Samter's triad |
| Pearly white mass from pars flaccida | Cholesteatoma (ear, not nose — wrong location) |
| Friable mass lateral wall | Inverted papilloma / malignancy |
| Black eschar in nasal cavity | Mucormycosis — emergency! |
10. Medicine (Clinical)
Investigations
| Investigation | Use |
|---|---|
| Nasal endoscopy | Direct visualization; essential for CRS diagnosis |
| CT sinuses (coronal) | Gold standard for sinusitis; shows mucosal thickening, air-fluid levels, OMC obstruction |
| MRI | Soft tissue detail; orbital/intracranial extension; distinguish polyp from tumor |
| Skin prick test / RAST (serum IgE) | Allergic rhinitis diagnosis |
| Nasal cytology | Eosinophilia (NARES, allergic); neutrophilia (infective) |
| Nasal NO | Low in primary ciliary dyskinesia |
| Ciliary beat frequency / electron microscopy | Primary ciliary dyskinesia workup |
| Sweat chloride / CFTR gene | Cystic fibrosis (bilateral polyps in child) |
Complications of Sinusitis
- Preseptal cellulitis → orbital cellulitis → subperiosteal abscess → orbital abscess → cavernous sinus thrombosis
- Chandler classification (I–V)
- Meningitis, epidural/subdural abscess, brain abscess, Pott's puffy tumour (frontal osteomyelitis with forehead swelling)
- Mucus-filled expansion of sinus (usually frontal); erodes bone; pushes orbit laterally
11. Pharmacology
A. Intranasal Corticosteroids (INCS) — First-Line for AR & CRS
| Drug | Example | Key Points |
|---|---|---|
| Fluticasone propionate/furoate | Flonase | High lipophilicity; minimal systemic absorption |
| Mometasone furoate | Nasonex | Very low bioavailability (<1%); safe long-term |
| Budesonide | Rhinocort | Good evidence in polyps |
| Beclomethasone | Beconase | Older; more systemic absorption |
Mechanism: reduce Th2 cytokines (IL-4, IL-5, IL-13), inhibit mast cells, reduce eosinophils, decrease goblet cell hyperplasia
B. Antihistamines
| Drug | Class | Use |
|---|---|---|
| Cetirizine, Loratadine, Fexofenadine | 2nd generation (non-sedating) H1 blocker | Allergic rhinitis; sneezing, rhinorrhea, itch; less effective for congestion |
| Diphenhydramine, Chlorphenamine | 1st generation | Sedating; avoid in elderly; effective but CNS side effects |
| Azelastine | Intranasal antihistamine | Rapid onset (<15 min); also anti-inflammatory |
C. Decongestants
| Drug | Type | Mechanism | Notes |
|---|---|---|---|
| Oxymetazoline | Topical (nasal) | α2-agonist; vasoconstriction | Max 3–5 days → rhinitis medicamentosa (rebound congestion) |
| Xylometazoline | Topical | α1/α2-agonist | Same risk as oxymetazoline |
| Pseudoephedrine | Oral | α/β-adrenergic | Effective for congestion; raises BP; precursor for methamphetamine |
| Phenylephrine | Oral | α1-agonist | Less effective than pseudoephedrine |
D. Leukotriene Modifiers
| Drug | Class | Use |
|---|---|---|
| Montelukast | LTD4 receptor antagonist | Allergic rhinitis + asthma (Samter's triad); nasal polyps |
| Zafirlukast | LTD4 receptor antagonist | Less commonly used for rhinitis |
E. Biologics (Severe CRS with Polyps)
| Drug | Target | Indication |
|---|---|---|
| Dupilumab | IL-4Rα (blocks IL-4 + IL-13) | CRS with nasal polyps (FDA approved 2019); also asthma |
| Omalizumab | Anti-IgE | Allergic rhinitis + asthma; reduces IgE-mediated mast cell activation |
| Mepolizumab | Anti-IL-5 | CRS with polyps + eosinophilic asthma |
F. Antibiotics for Rhinosinusitis
| Drug | Indication |
|---|---|
| Amoxicillin-clavulanate | First-line bacterial ARS (covers S. pneumo + β-lactamase producing H. inf and M. cat) |
| Doxycycline | Penicillin allergy |
| Levofloxacin / Moxifloxacin | Severe or failed first-line |
| Clindamycin + cefixime | MRSA concern in CRS |
G. Antifungals
| Drug | Use |
|---|---|
| Amphotericin B (liposomal) | Invasive (mucormycosis/aspergillus); IV; nephrotoxic |
| Voriconazole | Invasive aspergillosis; first-line alternative |
| Itraconazole | Allergic fungal sinusitis |
H. Immunotherapy
- Allergen immunotherapy (AIT): subcutaneous (SCIT) or sublingual (SLIT)
- Mechanism: shifts Th2 → Th1/Treg; increases blocking IgG4; induces tolerance
- Indication: allergic rhinitis not controlled by medications
- Only treatment that modifies disease course rather than just controlling symptoms
Summary Table
| Domain | Key Highlights |
|---|---|
| Surface Anatomy | Root, dorsum, apex, ala, columella, nasion, rhinion |
| Regional Anatomy | Septum, 3 turbinates, OMC, 4 paired sinuses; SPA supplies most of nasal cavity |
| Gross Anatomy | Bony + cartilaginous skeleton; nasal cycle via venous sinusoids; Kiesselbach's plexus |
| Histology | PCCE + goblet cells (respiratory); bipolar ORNs + Bowman's glands (olfactory); mucus sol/gel layers |
| Physiology | Filter/warm/humidify; mucociliary clearance 6 mm/min; olfactory G-protein cAMP cascade; nasal NO |
| Biochemistry | Mucins MUC5B/MUC5AC; sIgA; lysozyme; Th2 mediators (histamine, LTs, IL-4/5/13); olfactory cAMP pathway |
| Pathology | Allergic rhinitis (eosinophilic); CRS ± polyps; DNS; mucormycosis (black eschar = emergency); NPC (EBV) |
| Microbiology | ARS: S. pneumoniae; Mucormycosis in diabetics; fungal ball = Aspergillus in maxillary sinus |
| Clinical | "PODS" symptoms; Chandler classification for orbital complications; Pott's puffy tumour |
| Medicine | Coronal CT = gold standard; nasal NO for PCD; skin prick test for allergy |
| Pharmacology | INCS (mometasone) 1st line; dupilumab for CRS+polyps; avoid topical decongestants >5 days; AmBisome for mucor |
Throat please
throat anatomy pharynx larynx tonsils epiglottis labeled diagram
larynx vocal cords epiglottis endoscopy histology squamous epithelium
The Throat — Complete Multi-Disciplinary Overview
1. Surface Anatomy
External Landmarks (Anterior Neck)
| Landmark | Level | Structure |
|---|---|---|
| Hyoid bone | C3 | U-shaped bone; base of tongue; only bone without articulation |
| Thyroid notch | C4–C5 | Superior indentation of thyroid cartilage (Adam's apple) |
| Thyroid cartilage | C4–C5 | Largest laryngeal cartilage; "V"-shape; more prominent in males |
| Cricothyroid membrane | C5–C6 | Between thyroid and cricoid cartilages; site of emergency cricothyrotomy |
| Cricoid cartilage | C6 | Complete ring; narrowest part of airway in children |
| Tracheal rings | C6–C7 downward | Felt as corrugated surface below cricoid |
| Carotid pulse | Lateral neck | At level of thyroid cartilage |
Simple Drawing Guide — Surface Anatomy
Mandible
|
Hyoid bone ← C3 (palpable, moves with swallowing)
|
Thyroid notch
[THYROID CART.] ← C4-5 (Adam's apple)
|
Cricothyroid membrane ← Emergency airway here
[CRICOID CART.] ← C6
|
Tracheal rings
2. Regional Anatomy
A. The Pharynx
i. Nasopharynx (Epipharynx)
- Boundaries: Skull base (sphenoid/occipital) → soft palate
- Key structures:
- Eustachian tube orifice (lateral wall, at level of inferior turbinate) → middle ear communication
- Fossa of Rosenmüller (pharyngeal recess) — commonest site for nasopharyngeal carcinoma (NPC)
- Adenoids (pharyngeal tonsil) — posterior wall; prominent in children; regresses by puberty
- Pharyngobasilar fascia — strong fibrous roof
ii. Oropharynx
- Boundaries: Soft palate → tip of epiglottis/hyoid bone
- Key structures:
| Structure | Detail |
|---|---|
| Palatine tonsils | Between anterior (palatoglossal) and posterior (palatopharyngeal) pillars; most commonly infected |
| Tonsillar fossa | Bounded by superior constrictor muscle (medially) |
| Soft palate + uvula | Roof; separates naso- from oropharynx |
| Posterior pharyngeal wall | Vertebral bodies behind |
| Base of tongue (BOT) | Anterior floor; contains lingual tonsil |
| Vallecula | Depression between base of tongue and epiglottis |
Lymphatics from palatine tonsils drain to jugulodigastric nodes (Level II); spread also to Levels III, IV, V and retropharyngeal nodes (nodes of Rouvière) (Cummings, p. 1809)
iii. Hypopharynx (Laryngopharynx)
- Boundaries: Tip of epiglottis → lower border of cricoid (C6)
- Key structures:
| Structure | Detail |
|---|---|
| Pyriform sinuses | Lateral recesses either side of larynx; common site for foreign body lodgement and hypopharyngeal carcinoma |
| Posterior pharyngeal wall | C3–C6 vertebral levels |
| Post-cricoid region | Connects to oesophagus; site of Plummer-Vinson webs |
B. The Larynx
| Zone | Boundaries | Key Structures |
|---|---|---|
| Supraglottis | Epiglottis → false vocal cords | Epiglottis, aryepiglottic folds, false cords (vestibular folds), arytenoids |
| Glottis | True vocal cords + 1 cm below | True vocal cords, anterior commissure, posterior commissure |
| Subglottis | 1 cm below glottis → cricoid lower border | Transition to trachea; narrowest in children |
| Cartilage | Type | Function |
|---|---|---|
| Thyroid | Hyaline | Largest; forms anterior/lateral shield |
| Cricoid | Hyaline | Only complete ring; base of larynx |
| Epiglottis | Elastic | Leaf-shaped; folds back during swallowing to protect airway |
| Arytenoids (×2) | Hyaline | Pyramid-shaped; vocal cord attachment; abduction/adduction of cords |
| Corniculate (×2) | Elastic | Tips of arytenoids |
| Cuneiform (×2) | Elastic | Within aryepiglottic folds |
- Cricothyroid joint: thyroid tilts forward → lengthens/tenses vocal cords → higher pitch
- Cricoarytenoid joint: rotates arytenoids → abducts/adducts vocal cords
C. Nerve Supply
| Nerve | Origin | Supplies |
|---|---|---|
| Superior laryngeal nerve (SLN) | CN X (vagus) | External branch → cricothyroid muscle (tension/pitch); Internal branch → sensory above vocal cords |
| Recurrent laryngeal nerve (RLN) | CN X | All intrinsic laryngeal muscles EXCEPT cricothyroid; sensory below vocal cords |
| Glossopharyngeal (CN IX) | — | Sensory to oropharynx, posterior 1/3 tongue, tonsils |
| Trigeminal V2 | Maxillary | Soft palate, nasopharynx |
RLN vulnerability: Left RLN loops under aortic arch (longer course) → more at risk in thoracic/mediastinal pathology. Right RLN loops under subclavian artery.
D. Blood Supply
| Vessel | Origin | Area |
|---|---|---|
| Superior laryngeal artery | Superior thyroid → external carotid | Supraglottis |
| Inferior laryngeal artery | Inferior thyroid → subclavian | Subglottis + posterior larynx |
| Ascending pharyngeal artery | External carotid | Pharyngeal walls |
| Facial + lingual arteries | External carotid | Tonsils, tongue base, soft palate |
3. Gross Anatomy
Tonsillar Ring (Waldeyer's Ring)
Adenoids (pharyngeal tonsil) ← posterior nasopharynx
/ \
Tubal tonsils Tubal tonsils ← around Eustachian tube openings
| |
Palatine tonsils ← bilateral; between pillars
\ /
Lingual tonsil ← base of tongue
Palatine Tonsil — Gross Features
- Oval mass in tonsillar fossa
- Crypts: branching recesses in surface epithelium (~10–20); trap food debris → tonsilloliths
- Capsule: fibrous; separates tonsil from superior constrictor muscle
- No lymphatics in germinal centres (unlike other lymph nodes); subepithelial lymphatics drain to jugulodigastric nodes (Cummings, p. 1809)
Epiglottis — Gross
- Leaf-shaped elastic cartilage; attached to hyoid by hyoepiglottic ligament and to thyroid cartilage by thyroepiglottic ligament
- Vallecula: space between lingual surface of epiglottis and base of tongue — site of foreign body impaction
- Petiole: inferior narrow stalk; attaches at thyroid cartilage
Vocal Cords — Gross
- True vocal cords (vocal folds): pearly white; vibratory edge = free margin
- False vocal cords (vestibular folds): pink; no vibratory function; protective
- Glottis: opening between true cords — anterior commissure (anterior) + posterior commissure (arytenoids, posterior)
- Rima glottidis: ~60% membranous, ~40% cartilaginous (between arytenoids)
4. Histology
A. Pharyngeal Epithelium — Varies by Region
| Region | Epithelium | Rationale |
|---|---|---|
| Nasopharynx | Pseudostratified ciliated columnar (respiratory) + patches of stratified squamous | Transition zone |
| Oropharynx | Non-keratinizing stratified squamous epithelium | Exposed to friction/food |
| Hypopharynx | Non-keratinizing stratified squamous | Continuous with oesophagus |
B. Tonsil Histology
| Feature | Detail |
|---|---|
| Epithelium | Non-keratinizing stratified squamous; forms crypts — reticulated ("moth-eaten") where lymphocytes invade epithelium |
| Lymphoid follicles | Secondary follicles with germinal centres — B-cell zone |
| Interfollicular areas | T-cell zone |
| High endothelial venules (HEV) | Lymphocyte homing into tonsil tissue |
| Capsule | Fibrous; incomplete on medial surface |
C. Laryngeal Epithelium — Varies by Zone
| Region | Epithelium |
|---|---|
| Supraglottis (most) | Pseudostratified ciliated columnar (respiratory type) |
| True vocal cords (vibrating edge) | Non-keratinizing stratified squamous — resistant to vibratory stress |
| Subglottis | Pseudostratified ciliated columnar → transitions to tracheal epithelium |
D. Vocal Cord — Microanatomy (Reinke's Space)
____________________________________
| Stratified squamous epithelium | ← Surface
|____________________________________|
| Superficial lamina propria | ← Reinke's space (loose connective tissue)
| (loose fibrous tissue) | Oedema here = Reinke's oedema
|____________________________________|
| Intermediate + deep lamina propria| ← Vocal ligament (collagen + elastin)
|____________________________________|
| Vocalis muscle (thyroarytenoid) | ← Body of vocal fold
|____________________________________|
- Mucosa-cover model: superficial layer (mucosa/cover) vibrates over deeper body (vocalis muscle)
- Reinke's space: potential space in superficial LP; fluid accumulates here in Reinke's oedema (smoker's polypoid corditis)
E. Epiglottis Histology
- Elastic cartilage core (not hyaline — does NOT calcify)
- Laryngeal surface (posterior, airway-facing): stratified squamous epithelium
- Lingual surface (anterior, tongue-facing): respiratory (ciliated columnar) epithelium
- Mucous glands in lamina propria
5. Physiology
A. Swallowing (Deglutition) — 3 Phases
- Tongue shapes food into bolus, pushes it posteriorly against palate
- Soft palate elevates → seals nasopharynx (levator veli palatini, CN X)
Bolus touches fauces/posterior pharyngeal wall
↓
Swallowing centre (medulla — nucleus tractus solitarius)
↓
Sequence of coordinated events:
1. Soft palate rises → closes nasopharynx
2. Hyoid + larynx elevate anterosuperiorly
3. Epiglottis folds back → covers laryngeal inlet
4. True + false vocal cords adduct → close glottis
5. Pharyngeal constrictors contract (superior → inferior)
6. Upper oesophageal sphincter (cricopharyngeus) relaxes
↓
Bolus passes into oesophagus
- Entire pharyngeal phase in <1 second
- Respiration inhibited during swallowing (apnoea)
- Peristaltic waves carry bolus to stomach
- Lower oesophageal sphincter relaxes
B. Voice Production (Phonation)
Subglottic air pressure builds up
↓
Overcomes adducted vocal cord tension
↓
Cords blown apart (Bernoulli effect sucks them back)
↓
Rapid opening/closing cycles = mucosal wave
↓
Air pulsed into supraglottic resonating chambers
↓
Sound modified by: pharynx, palate, tongue, lips, teeth
| Parameter | Control |
|---|---|
| Pitch (frequency) | Cricothyroid muscle (lengthens/tenses cords → higher pitch) |
| Loudness | Subglottic air pressure |
| Quality/timbre | Resonance chambers (pharynx, oral cavity, nasal cavity) |
C. Laryngeal Protective Functions
| Function | Mechanism |
|---|---|
| Airway protection during swallowing | Epiglottis + aryepiglottic fold closure + true cord adduction |
| Cough reflex | Irritation → RLN afferents → forced expiration against momentarily closed glottis |
| Valsalva manoeuvre | Closed glottis → increases intrathoracic/intraabdominal pressure |
| Straining (defecation, childbirth) | Glottis closure fixes thorax |
D. Adenotonsillar Physiology
- Waldeyer's ring = first line immunological barrier to inhaled/ingested antigens
- Tonsils process antigens → generate secretory IgA + systemic antibody response
- Peak immunological activity: ages 4–10 years
- Function diminishes after puberty (atrophy)
6. Biochemistry
A. Saliva & Pharyngeal Mucus
| Component | Function |
|---|---|
| Mucins (MUC5B) | Lubrication for swallowing; protective gel layer |
| Amylase | Initiates starch digestion in oropharynx |
| Lysozyme + lactoferrin | Antimicrobial |
| sIgA | Mucosal immune defence; prevents microbial adhesion |
| Defensins (α + β) | Antimicrobial peptides from tonsillar crypts |
B. Vocal Cord Biochemistry
- Hyaluronic acid: abundant in Reinke's space → maintains viscoelasticity and pliability of vocal fold cover
- Fibronectin, collagen I/III: vocal ligament; provide tensile strength
- Elastin: allows recoil after vibration
- Loss of hyaluronic acid (scarring, ageing) → voice dysphonia, reduced mucosal wave
C. Inflammatory Mediators — Tonsillitis
| Mediator | Role |
|---|---|
| IL-1β, IL-6, TNF-α | Fever, acute phase response |
| IL-8 | Neutrophil recruitment to crypts |
| IFN-γ | Antiviral response (EBV, adenovirus) |
| M proteins (GAS) | Streptococcal virulence; molecular mimicry → rheumatic fever |
7. Pathology
A. Pharyngeal Pathology
| Condition | Key Pathology |
|---|---|
| Acute tonsillitis | Neutrophilic infiltrate; tonsillar swelling; crypt exudate |
| Peritonsillar abscess (Quinsy) | Pus collection between tonsil capsule and superior constrictor; deviation of uvula away from side of abscess |
| Retropharyngeal abscess | Pus in retropharyngeal space; pre-vertebral bulge; rare in adults |
| Infectious mononucleosis | EBV; lymphocytic infiltrate; atypical lymphocytes; tonsillar hypertrophy + exudate; risk of splenic rupture |
| Adenoid hypertrophy | Chronic hypertrophy → nasal obstruction, OME, mouth breathing, "adenoid facies" |
| Nasopharyngeal carcinoma | EBV-associated; undifferentiated type; fossa of Rosenmüller; early nodal metastasis |
| Oropharyngeal SCC | Increasingly HPV-16 driven (p16 positive); tonsil and BOT commonest sites; better prognosis than HPV-negative |
B. Laryngeal Pathology
| Condition | Key Pathology |
|---|---|
| Acute epiglottitis | Severe supraglottic oedema; H. influenzae type b; "thumb sign" on X-ray; airway emergency |
| Laryngotracheobronchitis (Croup) | Parainfluenza virus; subglottic oedema; "steeple sign" on X-ray; barking cough |
| Reinke's Oedema | Oedema in superficial lamina propria (Reinke's space); bilateral; chronic smokers; low-pitched voice |
| Vocal cord nodules | Bilateral; anterior 1/3 - mid-cord junction; fibrous thickening; voice misuse |
| Vocal cord polyp | Unilateral; haemorrhagic or hyaline stroma; acute vocal trauma |
| Laryngomalacia | Most common cause of stridor in infants; floppy epiglottis/arytenoids collapse during inspiration |
| Laryngeal papillomatosis | HPV 6/11; squamous papillomas; recurrent; airway risk in children |
| Condition | Key Pathology |
|---|---|
| Laryngeal SCC | Squamous cell; glottic most common; early hoarseness (good prognosis); supraglottic presents late |
| Vocal cord palsy (RLN palsy) | Left side more common; causes: thyroid surgery, lung/mediastinal malignancy, aortic arch pathology |
C. Hypopharyngeal Pathology
| Condition | Key Pathology |
|---|---|
| Hypopharyngeal SCC | Pyriform sinus (70%); late presentation; poor prognosis |
| Plummer-Vinson syndrome | Iron deficiency anaemia + post-cricoid web + dysphagia; risk of post-cricoid carcinoma |
| Zenker's diverticulum | Pulsion diverticulum at Killian's dehiscence (weak triangle between thyropharyngeus and cricopharyngeus) |
8. Microbiology
Pharyngitis / Tonsillitis
| Organism | Notes |
|---|---|
| Group A Streptococcus (GAS) = S. pyogenes | Most important bacterial cause; exudative tonsillitis; Centor/McIsaac criteria; complications: rheumatic fever, GN, peritonsillar abscess |
| Epstein-Barr virus (EBV) | Infectious mononucleosis; most common viral cause of severe exudative tonsillitis; heterophile antibody (Monospot) |
| Adenovirus | Common viral pharyngitis; pharyngoconjunctival fever |
| Rhinovirus / Coronavirus | Most common overall cause of pharyngitis (viral URTI) |
| Fusobacterium necrophorum | Lemierre's syndrome: peritonsillar abscess → IJV thrombophlebitis → septic emboli |
| Corynebacterium diphtheriae | Diphtheria; grey pseudomembrane; bull-neck; myocarditis/neuropathy; prevented by vaccine |
| Neisseria gonorrhoeae | STI-related pharyngitis |
| Treponema pallidum | Secondary syphilis: mucous patches |
Acute Epiglottitis
| Organism | Notes |
|---|---|
| Haemophilus influenzae type b (Hib) | Classic cause (pre-vaccine era); still occurs in unvaccinated |
| GAS, S. pneumoniae, S. aureus | Post-vaccine era pathogens |
Deep Space Neck Infections
- Peritonsillar abscess: GAS + oral anaerobes (Prevotella, Fusobacterium, Peptostreptococcus)
- Retropharyngeal abscess: Staphylococcus, GAS, anaerobes, H. influenzae (children)
- Ludwig's angina: submandibular space infection; mixed oral flora; floor of mouth
9. Clinical Presentation
Symptom Framework — Throat
| Symptom | Common Causes |
|---|---|
| Sore throat (odynophagia) | Viral/bacterial pharyngitis, tonsillitis, peritonsillar abscess |
| Dysphagia | Peritonsillar abscess, epiglottitis, hypopharyngeal SCC, Zenker's, PVS |
| Hoarseness (dysphonia) | Vocal cord nodules, polyp, SCC, RLN palsy, laryngitis |
| Stridor | Epiglottitis (inspiratory), croup (inspiratory), laryngomalacia (inspiratory) |
| Muffled/hot potato voice | Peritonsillar abscess |
| Referred otalgia | Tonsillitis, oropharyngeal/hypopharyngeal carcinoma (via CN IX/X–Arnold's nerve) |
| Neck mass | Lymphoma, metastatic SCC (tonsil, BOT, NPC), peritonsillar/retropharyngeal abscess |
Centor/McIsaac Score (Bacterial Tonsillitis)
| Criterion | Score |
|---|---|
| Tonsillar exudate | +1 |
| Tender anterior cervical lymphadenopathy | +1 |
| Fever >38°C | +1 |
| Absence of cough | +1 |
| Age 3–14 | +1 |
| Age ≥45 | -1 |
Score ≥4: treat with antibiotics / rapid strep test positive → treat
Epiglottitis — Classic Presentation (Emergency!)
- "4 Ds": Drooling · Dysphagia · Dysphonia · Distress
- Child sits leaning forward ("tripod position")
- Lateral neck X-ray: "Thumb sign" (enlarged epiglottis)
- Do NOT examine throat with tongue depressor → may precipitate airway obstruction
10. Medicine (Clinical)
Investigations
| Investigation | Use |
|---|---|
| Throat swab + culture | GAS confirmation; sensitivity ~90% |
| Rapid antigen detection test (RADT) | Point-of-care GAS test; specificity ~99% |
| Monospot (Paul-Bunnell) | Heterophile antibodies for EBV; false-negative in <3 years |
| EBV-specific antibodies | VCA IgM (acute), EA (early antigen), EBNA (late/past infection) |
| Flexible nasopharyngoscopy | Laryngeal, hypopharyngeal, nasopharyngeal visualisation |
| Direct laryngoscopy + biopsy | Laryngeal lesion characterisation |
| CT neck with contrast | Deep space infections, abscess, tumour staging |
| MRI | Soft tissue detail; perineural spread, BOT tumours |
| PET-CT | Staging oropharyngeal/laryngeal carcinoma; unknown primary |
| Video fluoroscopy (VFSS) | Swallowing study; aspiration risk assessment |
| Stroboscopy | Vocal cord mucosal wave assessment; voice clinic |
Complications of Tonsillitis/Pharyngitis
- Peritonsillar abscess (quinsy) — most common
- Parapharyngeal/retropharyngeal abscess
- Otitis media (Eustachian tube dysfunction)
- Rheumatic fever (2–4 weeks after GAS pharyngitis): carditis, arthritis, chorea, subcutaneous nodules, erythema marginatum (Jones criteria)
- Post-streptococcal glomerulonephritis (1–3 weeks): haematuria, oedema, hypertension
- PANDAS: paediatric autoimmune neuropsychiatric disorder
- F. necrophorum → peritonsillar abscess → IJV thrombophlebitis → septic pulmonary emboli → sepsis
- Young adults; often mistaken for "glandular fever"
11. Pharmacology
A. Antibiotics for Throat Infections
| Drug | Indication | Notes |
|---|---|---|
| Phenoxymethylpenicillin (Pen V) | First-line GAS tonsillitis | 10-day course to prevent rheumatic fever |
| Amoxicillin | GAS tonsillitis | AVOID in undiagnosed mononucleosis → ampicillin rash (maculopapular) |
| Cephalexin / Cefuroxime | Penicillin-allergic (non-severe) | |
| Clindamycin | Penicillin allergy (severe) or MRSA concern; peritonsillar abscess | |
| Co-amoxiclav | Deep space infections; peritonsillar abscess | Covers anaerobes |
| Metronidazole | Add to cover anaerobes in Lemierre's, deep neck infections | |
| Benzylpenicillin (IV) | Severe GAS infection; acute rheumatic fever treatment |
B. Steroids
| Drug | Use |
|---|---|
| Dexamethasone (single dose) | Acute tonsillitis/pharyngitis: reduces pain, swelling, time to symptom relief |
| Dexamethasone (nebulised/IM) | Croup: reduces subglottic oedema; single dose highly effective |
| Prednisolone | Severe EBV tonsillitis with airway compromise; laryngeal oedema |
C. Inhaled / Nebulised Agents
| Drug | Use |
|---|---|
| Adrenaline (nebulised) | Acute croup with severe stridor; reduces subglottic oedema (α-vasoconstriction); temporary — rebound after 2 hrs |
| Heliox (helium-oxygen) | Upper airway obstruction; reduces turbulent flow, work of breathing |
| Budesonide (nebulised) | Croup; equivalent to oral/IM dexamethasone |
D. Voice & Laryngeal Pharmacology
| Drug | Indication |
|---|---|
| Proton pump inhibitors (omeprazole, lansoprazole) | Laryngopharyngeal reflux (LPR) — key cause of chronic laryngitis, granulomas, subglottic stenosis |
| Botulinum toxin A (Botox) | Spasmodic dysphonia (laryngeal dystonia): injected into thyroarytenoid muscle; reduces spasm; lasts 3–4 months |
| Intralesional cidofovir / bevacizumab | Adjuvant therapy in recurrent laryngeal papillomatosis |
| Intralesional corticosteroid | Vocal cord granuloma (post-intubation) |
E. Biologics / Targeted Therapy
| Drug | Target | Use |
|---|---|---|
| Cetuximab (anti-EGFR) | EGFR | Oropharyngeal/laryngeal SCC + platinum/radiotherapy |
| Pembrolizumab / Nivolumab (anti-PD-1) | PD-1/PD-L1 | Recurrent/metastatic head and neck SCC (HPV+ and HPV−); first-line in PD-L1 high |
| Nivolumab | PD-1 | Second-line H&N SCC |
F. Rheumatic Fever Prophylaxis
| Drug | Dose | Duration |
|---|---|---|
| Benzathine penicillin G (IM monthly) | 1.2 MU IM every 4 weeks | Until age 21 (no carditis) or lifelong (with carditis) |
| Phenoxymethylpenicillin (oral) | 250 mg BD | Alternative secondary prophylaxis |
| Sulfadiazine | 1 g/day | Penicillin allergy |
Summary Table
| Domain | Key Highlights |
|---|---|
| Surface Anatomy | Hyoid (C3), thyroid cartilage (C4–5), cricothyroid membrane = emergency airway, cricoid (C6) |
| Regional Anatomy | Pharynx = nasopharynx / oropharynx / hypopharynx; larynx = supraglottis / glottis / subglottis; Waldeyer's ring |
| Gross Anatomy | Tonsillar crypts + jugulodigastric drainage; Reinke's space; Killian's dehiscence (Zenker's) |
| Histology | Oropharynx/hypopharynx = non-keratinizing stratified squamous; vocal cords = stratified squamous over Reinke's space; tonsil = reticulated crypt epithelium |
| Physiology | 3-phase swallowing; myoelastic phonation; pitch by cricothyroid; cough/Valsalva via glottis closure |
| Biochemistry | Hyaluronic acid = vocal cord viscoelasticity; M protein = rheumatic fever mechanism; EBV → lymphocytic infiltrate |
| Pathology | Quinsy (GAS), epiglottitis (Hib), croup (parainfluenza), HPV-16 oropharyngeal SCC, RLN palsy |
| Microbiology | GAS = most important bacterial; EBV = viral; Fusobacterium → Lemierre's; C. diphtheriae = pseudomembrane |
| Clinical | Centor score; 4Ds of epiglottitis; ampicillin rash in mono; referred otalgia = pharyngeal/laryngeal Ca |
| Medicine | RADT for GAS; stroboscopy for mucosal wave; VFSS for aspiration; PET-CT for staging |
| Pharmacology | Pen V for GAS; dexamethasone for croup; Botox for spasmodic dysphonia; pembrolizumab for H&N SCC; benzathine pen for RF prophylaxis |
Eyes please
eye anatomy labeled diagram cornea retina lens optic nerve cross section
retinal layers histology OCT rods cones ganglion cells fundus
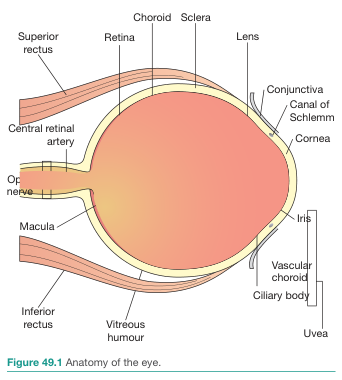
The Eye — Complete Multi-Disciplinary Overview
1. Surface Anatomy
External Eye Landmarks
| Landmark | Description |
|---|---|
| Eyelids (palpebrae) | Upper + lower; meet at medial canthus (inner corner) and lateral canthus (outer corner) |
| Palpebral fissure | Opening between lids; ~30 mm wide × 10 mm tall |
| Tarsal plates | Dense fibrous plates within each lid; give structural rigidity |
| Meibomian glands | Sebaceous glands in tarsal plate; ~25 in upper lid, ~20 in lower; open at lid margin |
| Lashes (cilia) | 2–3 rows; associated with Glands of Zeis (sebaceous) and Glands of Moll (apocrine) |
| Conjunctiva | Thin mucous membrane; palpebral (lines lids) + bulbar (covers sclera); meet at fornix |
| Limbus | Junction of cornea and sclera; site of corneal stem cells |
| Caruncle | Fleshy pink mound at medial canthus; modified skin with sebaceous glands |
| Plica semilunaris | Vestigial third eyelid at medial canthus |
| Lacrimal puncta | Tiny openings at medial lid margins → drain tears into lacrimal sac |
Simple Drawing Guide
Superior lid
_____
/ | | \
/ Upper fornix \ ← Conjunctival sac
| Bulbar conjunctiva |
| [white sclera] |
| [coloured iris] |
| [black pupil] |
\ /
\ Limbus (ring) /
¯¯¯¯¯¯¯¯¯¯¯
Inferior lid
Lacrimal punctum (medial)
2. Regional Anatomy
A. Eyeball (Globe) — Three Concentric Coats
OUTER COAT MIDDLE COAT (UVEA) INNER COAT
___________________ ___________________ _______________
| Cornea (anterior) | | Iris | | Retina |
| | | Ciliary body | | (sensory) |
| Sclera (posterior)| | Choroid | | |
|___________________| |___________________| |_______________|
B. Anterior Segment
| Structure | Detail |
|---|---|
| Cornea | Transparent; avascular; ~11–12 mm diameter; 5-layered; responsible for ~70% of total refracting power (~43 D) |
| Anterior chamber | Between cornea and iris; filled with aqueous humour; depth ~3 mm |
| Iris | Pigmented diaphragm; controls pupil size; sphincter pupillae (CN III, miosis) + dilator pupillae (sympathetic, mydriasis) |
| Pupil | Central aperture of iris; normally 2–5 mm; reacts to light (direct + consensual) |
| Posterior chamber | Between iris and lens; contains aqueous humour |
| Lens | Biconvex; avascular; ~10 mm diameter; contributes ~20 D (variable); held by zonule fibres (of Zinn) from ciliary body |
| Ciliary body | Ring of smooth muscle + secretory epithelium; ciliary muscle (CN III) → accommodation; ciliary epithelium → produces aqueous humour |
| Canal of Schlemm | Circular venous channel at limbus; drains aqueous humour → trabecular meshwork → episcleral veins |
C. Posterior Segment
| Structure | Detail |
|---|---|
| Vitreous humour | Gel (99% water + collagen fibrils + hyaluronic acid); fills posterior cavity (~4 mL); attached at vitreous base, optic disc, macula, retinal vessels |
| Retina | ~10-layered neural tissue; extends from optic disc to ora serrata |
| Macula | Central retina, ~5 mm; contains highest cone density; fovea centralis at centre = point of maximum visual acuity (cones only, no vessels) |
| Optic disc | ~1.5 mm; where ganglion cell axons exit as optic nerve; no photoreceptors = blind spot |
| Choroid | Vascular layer between retina and sclera; nourishes outer retina; rich in melanin |
| Sclera | Tough white outer coat; continuous with cornea at limbus; site of extraocular muscle insertion |
D. Extraocular Muscles & Nerve Supply
| Muscle | Action | Nerve |
|---|---|---|
| Medial rectus | Adduction | CN III |
| Lateral rectus | Abduction | CN VI (abducens) |
| Superior rectus | Elevation + intorsion + adduction | CN III |
| Inferior rectus | Depression + extorsion + adduction | CN III |
| Superior oblique | Intorsion + depression + abduction | CN IV (trochlear) |
| Inferior oblique | Extorsion + elevation + abduction | CN III |
| Levator palpebrae | Elevates upper lid | CN III (+ sympathetic for Müller's muscle) |
Mnemonic: "LR6SO4" — Lateral Rectus = CN VI, Superior Oblique = CN IV, all others = CN III
E. Lacrimal System
Lacrimal gland (superolateral orbit)
↓ (tears)
Tear film over cornea/conjunctiva
↓
Upper + lower lacrimal puncta (medial lids)
↓
Canaliculi → common canaliculus
↓
Lacrimal sac (medial orbital wall)
↓
Nasolacrimal duct → inferior meatus of nose
- Lacrimal gland: serous + mucous secretion; innervated by CN VII (parasympathetic via pterygopalatine ganglion)
- Tear film: 3 layers: lipid (Meibomian) + aqueous (lacrimal) + mucin (goblet cells)
F. Orbital Anatomy
- Bony orbit: 7 bones — frontal, zygomatic, maxilla, palatine, lacrimal, ethmoid, sphenoid
- Optic canal (sphenoid): transmits CN II (optic nerve) + ophthalmic artery
- Superior orbital fissure: CN III, IV, V1 (ophthalmic), VI + superior ophthalmic vein
- Inferior orbital fissure: CN V2 (maxillary), inferior ophthalmic vein
3. Gross Anatomy
Cornea — 5 Layers (Gross to Micro)
1. Epithelium (stratified squamous, 5–6 cell layers)
2. Bowman's layer (acellular condensed stroma)
3. Stroma (90% of corneal thickness; collagen lamellae)
4. Descemet's membrane (basement membrane of endothelium)
5. Endothelium (single layer; maintains corneal dehydration/clarity)
- Total thickness: ~0.5 mm centrally, ~0.7 mm peripherally
- Avascular — nourished by aqueous humour (anterior) and tear film (anterior surface)
- Innervation: densely innervated by CN V1 (ophthalmic) — most sensitive tissue in the body
Lens — Gross Features
- Three components: capsule (elastic basement membrane) + epithelium (anterior only) + lens fibres (crystallins)
- No nucleus in mature fibres; no blood supply; nourished by aqueous/vitreous
- Zonules of Zinn: suspensory ligaments from ciliary body
Optic Nerve
- ~50 mm long; 4 segments: intraocular (1 mm) → intraorbital (25–30 mm) → intracanalicular (6–9 mm) → intracranial (10 mm)
- Surrounded by meningeal sheaths (dura, arachnoid, pia) → subarachnoid space continues → raised ICP → papilloedema
- Contains ~1.2 million nerve fibres (retinal ganglion cell axons)
4. Histology
A. Retinal Layers (10 layers, outer → inner)
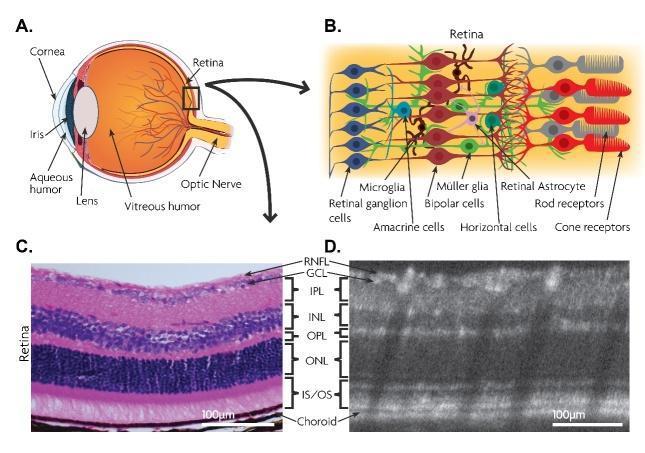
| Layer | Cells/Content |
|---|---|
| 1. Retinal Pigment Epithelium (RPE) | Single layer of hexagonal pigmented cells; phagocytoses shed photoreceptor outer segments; vitamin A recycling; blood-retinal barrier (outer) |
| 2. Photoreceptor layer | Outer segments of rods + cones (contain visual pigments) |
| 3. Outer limiting membrane (OLM) | Zonula adherens between photoreceptors and Müller cells |
| 4. Outer nuclear layer (ONL) | Cell bodies (nuclei) of rods and cones |
| 5. Outer plexiform layer (OPL) | Synapses: photoreceptors → bipolar + horizontal cells |
| 6. Inner nuclear layer (INL) | Bipolar cells, horizontal cells, amacrine cells, Müller cell nuclei |
| 7. Inner plexiform layer (IPL) | Synapses: bipolar + amacrine cells → ganglion cells |
| 8. Ganglion cell layer (GCL) | Retinal ganglion cells (RGC); axons form optic nerve |
| 9. Nerve fibre layer (RNFL) | Axons of ganglion cells converging to optic disc |
| 10. Internal limiting membrane (ILM) | Basement membrane of Müller cells; vitreous boundary |
B. Rods vs Cones
| Feature | Rods | Cones |
|---|---|---|
| Number | ~120 million | ~6–7 million |
| Distribution | Peripheral retina; absent from fovea | Concentrated at fovea/macula |
| Function | Scotopic vision (low light) | Photopic vision (colour, detail) |
| Pigment | Rhodopsin (opsin + 11-cis retinal) | Photopsin (S, M, L — blue, green, red) |
| Convergence | High (many rods → 1 ganglion cell) | Low (1:1 at fovea) |
| Sensitivity | High | Low |
C. Corneal Histology
- Epithelium: 5–6 layers non-keratinizing stratified squamous; rapid turnover (7–10 days); stem cells at limbus
- Bowman's layer: acellular collagen mesh; does NOT regenerate if damaged
- Stroma: 200+ regularly arranged collagen lamellae (type I) + keratocytes; regular arrangement = transparency
- Descemet's membrane: thick (~10 µm in adults); produced by endothelium
- Endothelium: single layer of hexagonal cells (~2,500 cells/mm²); pump fluid out of stroma (Na⁺/K⁺-ATPase); does NOT regenerate — cell density decreases with age
D. Iris Histology
- Anterior: loose collagen stroma with melanocytes (iris colour)
- Posterior: double layer of pigmented epithelium (continuation of ciliary epithelium)
- Sphincter pupillae: smooth muscle ring at pupillary margin (parasympathetic — CN III)
- Dilator pupillae: radial myoepithelial cells (sympathetic)
5. Physiology
A. Aqueous Humour Dynamics
Ciliary epithelium (non-pigmented layer)
↓ secretion (~2–3 µL/min; active transport + ultrafiltration)
Posterior chamber
↓ (through pupil)
Anterior chamber
↓
Trabecular meshwork (conventional, 90%)
↓
Canal of Schlemm → episcleral veins
(Uveoscleral pathway: 10%)
- Normal intraocular pressure (IOP): 10–21 mmHg
- IOP = Rate of aqueous production / Facility of outflow (resistance of trabecular meshwork)
- Aqueous provides nutrients (glucose, O₂, amino acids) to avascular cornea and lens
B. Accommodation (Near Focus)
Near object → ciliary muscle CONTRACTS (CN III parasympathetic)
↓
Zonule fibres RELAX (become slack)
↓
Lens becomes MORE CONVEX (elastic recoil)
↓
Increased refracting power → near focus
- Presbyopia: age-related loss of accommodation; lens hardening reduces elasticity (typically >40 years)
- Accommodation reflex triad: convergence + accommodation + miosis
C. Pupillary Light Reflex
Light → Retinal ganglion cells (intrinsically photosensitive: melanopsin/ipRGCs)
↓ CN II (afferent)
Pretectal nucleus (midbrain)
↓ (bilateral projection)
Edinger-Westphal nucleus (CN III parasympathetic)
↓ CN III (efferent)
Ciliary ganglion → short ciliary nerve → sphincter pupillae → miosis
- Direct reflex: light in same eye → constriction in same eye
- Consensual reflex: light in one eye → constriction in both eyes (bilateral pretectal projection)
- RAPD (Relative Afferent Pupillary Defect): swinging flashlight test; affected eye shows paradoxical dilation when light swings to it → optic nerve lesion
D. Phototransduction (Visual Transduction)
Light → rhodopsin (11-cis retinal → all-trans retinal)
↓
Opsin activates transducin (Gα protein)
↓
Phosphodiesterase (PDE) activated → cGMP hydrolysed
↓
cGMP-gated Na⁺/Ca²⁺ channels CLOSE → hyperpolarization
↓
Less glutamate released at photoreceptor synapse → bipolar cell activation
↓
Retinal ganglion cell fires → optic nerve → visual cortex
Note: photoreceptors are depolarized in the dark (Na⁺ influx via cGMP channels = "dark current") and hyperpolarize in light — opposite to most sensory systems.
E. Visual Pathway
Retina → Optic nerve (CN II)
↓
Optic chiasm (nasal fibres decussate; temporal fibres stay ipsilateral)
↓
Optic tract → Lateral Geniculate Nucleus (LGN) of thalamus
↓
Optic radiation (Meyer's loop inferiorly through temporal lobe)
↓
Primary visual cortex (V1) — calcarine fissure, occipital lobe
| Lesion | Visual Field Defect |
|---|---|
| Optic nerve | Monocular blindness (ipsilateral) |
| Optic chiasm (pituitary) | Bitemporal hemianopia |
| Optic tract | Contralateral homonymous hemianopia |
| Meyer's loop (temporal lobe) | "Pie in the sky" — superior quadrantanopia |
| Parietal lobe | Inferior quadrantanopia |
| Occipital cortex (V1) | Homonymous hemianopia with macular sparing |
6. Biochemistry
A. Visual Cycle (Retinoid Cycle)
All-trans retinal (after light activation)
↓ (reduced to all-trans retinol)
Transported to RPE
↓ (RPE isomerase)
11-cis retinal regenerated
↓
Transported back to photoreceptor outer segment
↓ + opsin → rhodopsin (dark-adapted)
- Vitamin A (retinol) is essential — deficiency → night blindness (nyctalopia)
- RPE is central to visual cycle — RPE dysfunction → photoreceptor death
B. Lens Biochemistry
| Protein | Function |
|---|---|
| α-crystallin | Heat shock protein; prevents protein aggregation; most abundant |
| β/γ-crystallins | Structural proteins; maintain transparency by short-range order |
| Glutathione | Antioxidant; maintains lens protein in reduced state |
- Cataract formation: oxidative damage to crystallins → protein aggregation → opacification
- Lens relies on anaerobic glycolysis (no mitochondria in mature fibres) → high sorbitol in diabetes (polyol pathway) → osmotic cataract
C. Aqueous Humour Biochemistry
- High ascorbic acid (antioxidant; ~20× plasma concentration)
- High hyaluronic acid in vitreous
- Low protein (unlike blood) → maintains optical clarity
- Tryptophan metabolites → absorb UV radiation (protecting lens/retina)
D. Intraocular Pressure — Molecular Regulation
- Prostaglandins (PGF2α): increase uveoscleral outflow → lower IOP
- Beta-blockers: decrease aqueous secretion (inhibit β-adrenergic receptors on ciliary epithelium)
- Carbonic anhydrase: produces HCO₃⁻ essential for active secretion of aqueous → inhibition lowers IOP
7. Pathology
A. Corneal Pathology
| Condition | Key Pathology |
|---|---|
| Keratoconus | Progressive thinning + ectasia of cornea; cone-shaped deformity; irregular astigmatism; Munson's sign |
| Corneal ulcer | Epithelial defect ± stromal infiltrate; bacterial, viral (HSV — dendrite), fungal, Acanthamoeba |
| Fuchs' endothelial dystrophy | Endothelial cell loss → corneal oedema; guttata on Descemet's; bilateral; worse in AM |
| Band keratopathy | Calcium phosphate deposition in Bowman's layer; associated with hypercalcaemia, chronic inflammation |
B. Lens Pathology
| Condition | Key Pathology |
|---|---|
| Cataract | Lens opacity; nuclear (age, UV), cortical, posterior subcapsular (steroids, diabetes); leading cause of reversible blindness worldwide |
| Ectopia lentis | Lens subluxation; Marfan's (upward — FBN1 mutation), homocystinuria (downward) |
C. Glaucoma
| Type | Mechanism | Key Features |
|---|---|---|
| Primary open-angle (POAG) | Trabecular meshwork dysfunction → ↑IOP → optic nerve damage | Most common; painless; insidious visual field loss; cup:disc ratio >0.6 |
| Acute angle-closure | Pupil block → iris bows forward → blocks trabecular meshwork | Painful red eye; rock-hard globe; mid-dilated non-reactive pupil; halos; vomiting; emergency! |
| Normal tension | Optic nerve damage at normal IOP; vascular insufficiency | Diagnosed by optic nerve appearance + VF loss despite normal IOP |
| Secondary | Caused by: neovascularisation (diabetes), trauma, uveitis, steroid-induced | Variable mechanism |
D. Retinal Pathology
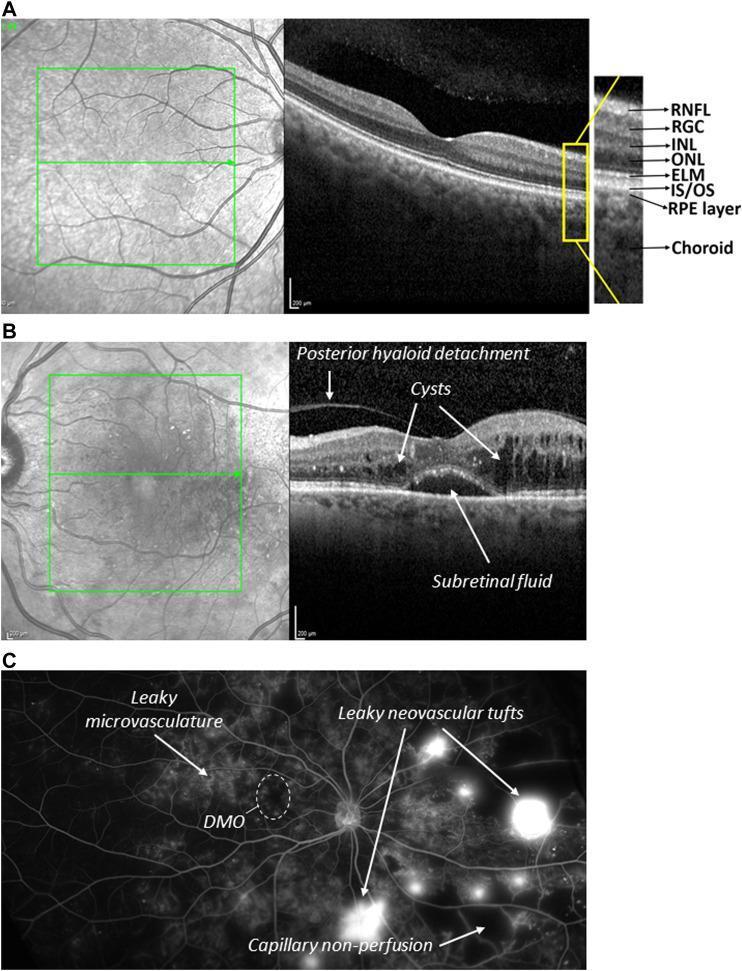
| Condition | Key Pathology |
|---|---|
| Retinal detachment | Separation of neurosensory retina from RPE; rhegmatogenous (tear), tractional (PDR), exudative (tumour, inflammation) |
| Age-related macular degeneration (AMD) | Dry: drusen + RPE atrophy; Wet: choroidal neovascularisation (CNV) → subretinal haemorrhage; VEGF-driven |
| Diabetic retinopathy | Background: microaneurysms, dot-blot haemorrhages, hard exudates; Proliferative (PDR): neovascularisation on disc/retina |
| Retinitis pigmentosa (RP) | Hereditary rod-cone dystrophy; bone-spicule pigmentation; tunnel vision; ERG extinguished |
| Central retinal artery occlusion (CRAO) | Sudden painless visual loss; pale oedematous retina + cherry-red spot at fovea |
| Central retinal vein occlusion (CRVO) | Flame haemorrhages in all 4 quadrants; disc swelling; "stormy sunset" fundus |
E. Optic Nerve Pathology
| Condition | Key Features |
|---|---|
| Papilloedema | Bilateral disc swelling from raised ICP; enlarged blind spot; late: visual field loss |
| Optic neuritis | Demyelination (MS); unilateral painful visual loss; RAPD; central scotoma; Marcus Gunn pupil |
| Optic atrophy | End-stage optic nerve damage; pale disc; causes: glaucoma, ischaemia, compression |
8. Microbiology
Conjunctivitis
| Organism | Type | Features |
|---|---|---|
| Adenovirus (types 3, 7, 8, 19) | Viral | Most common; watery discharge; follicular; pharyngoconjunctival fever (types 3,7) or epidemic keratoconjunctivitis (types 8,19) |
| Chlamydia trachomatis (D–K) | Bacterial | Adult inclusion conjunctivitis; STI-related; follicular |
| Chlamydia trachomatis (A–C) | Bacterial | Trachoma — leading cause of preventable blindness worldwide; pannus formation; trichiasis → corneal scarring |
| N. gonorrhoeae | Bacterial | Hyperacute (profuse purulent discharge within 24h); corneal perforation risk; neonatal ophthalmia neonatorum |
| S. aureus, S. pneumoniae, H. influenzae | Bacterial | Acute bacterial conjunctivitis; mucopurulent discharge; lid crusting |
| Herpes simplex virus (HSV-1) | Viral | Dendritic corneal ulcer; recurrent; staining with fluorescein |
| Herpes zoster ophthalmicus (VZV) | Viral | V1 distribution rash; Hutchinson's sign (tip of nose) → nasociliary nerve involvement → high risk of eye disease |
Endophthalmitis
- Post-surgical: S. epidermidis, S. aureus, Gram-negative rods
- Post-traumatic: Bacillus cereus (soil/vegetable matter injury — very virulent)
- Endogenous (haematogenous): Candida, Aspergillus, Klebsiella (diabetics in Asia)
Toxoplasmosis (Posterior Uveitis)
- Toxoplasma gondii; most common cause of posterior uveitis worldwide
- "Headlight in fog": white fluffy retinal lesion adjacent to old pigmented scar
- Reactivation of congenital or acquired infection
9. Clinical Presentation
Red Eye — Differential Diagnosis
| Condition | Pain | Vision | Discharge | Pupil | IOP |
|---|---|---|---|---|---|
| Conjunctivitis | Gritty | Normal | Watery/purulent | Normal | Normal |
| Corneal ulcer | Severe | Reduced | Watery | Normal/small | Normal |
| Acute angle-closure | Severe | Reduced | None | Mid-dilated, fixed | Very high |
| Anterior uveitis (iritis) | Ache | Reduced | None | Small, irregular | Low/normal |
| Scleritis | Severe, boring | Normal/reduced | None | Normal | Normal |
| Episcleritis | Mild | Normal | None | Normal | Normal |
| Subconjunctival haemorrhage | None | Normal | None | Normal | Normal |
Sudden Visual Loss — Framework
| Cause | Features |
|---|---|
| CRAO | Painless, sudden, complete; pale retina + cherry red spot |
| Retinal detachment | Flashes + floaters → curtain/shadow visual field loss |
| Vitreous haemorrhage | Sudden floaters/red vision; no fundal view; PDR, CRVO, trauma |
| Ischaemic optic neuropathy (AION) | Painless; altitudinal field defect; disc swelling; associated with giant cell arteritis |
| Optic neuritis | Painful; central scotoma; RAPD; young female; MS |
Marcus Gunn (RAPD) Test
- Swinging flashlight: light in normal eye → both pupils constrict
- Light swings to affected eye → both pupils dilate (paradoxical response)
- Indicates ipsilateral optic nerve or extensive retinal disease
10. Medicine (Clinical)
Ophthalmic Investigations
| Test | Use |
|---|---|
| Slit-lamp biomicroscopy | Anterior segment examination (cornea, lens, anterior chamber) |
| Fundoscopy (ophthalmoscopy) | Posterior segment: disc, macula, vessels, retina |
| OCT (Optical Coherence Tomography) | Retinal layer cross-section; macula thickness; RNFL for glaucoma |
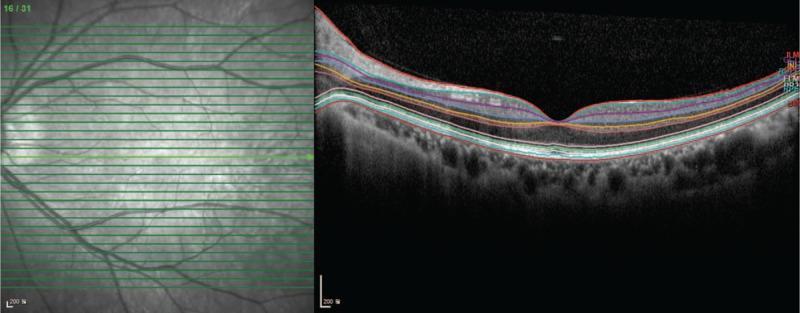
| Test | Use |
|---|---|
| Fluorescein angiography (FFA) | Retinal vascular disease; AMD; diabetic retinopathy |
| Visual field testing (perimetry) | Glaucoma monitoring; optic nerve/chiasm lesions |
| Electroretinogram (ERG) | Photoreceptor function; RP, toxicity monitoring |
| Tonometry (Goldmann) | Gold-standard IOP measurement |
| Corneal topography | Keratoconus; pre-refractive surgery |
| B-scan ultrasound | Posterior segment when media opacity blocks view; retinal detachment |
Diabetic Eye Disease Grading (ETDRS / UK NSC)
| Grade | Features |
|---|---|
| R0 | No diabetic retinopathy |
| R1 (Background) | Microaneurysms, dot-blot haemorrhages, hard exudates |
| R2 (Pre-proliferative) | Cotton wool spots, venous beading, IRMA (intraretinal microvascular abnormalities) |
| R3 (Proliferative) | New vessels on disc (NVD) or elsewhere (NVE) |
| M1 (Maculopathy) | Exudates or oedema within 1 disc diameter of fovea |
11. Pharmacology
A. Glaucoma Treatments (Lowering IOP)
| Drug Class | Example | Mechanism | Notes |
|---|---|---|---|
| Prostaglandin analogues | Latanoprost, bimatoprost, travoprost | ↑ Uveoscleral outflow (FP receptor agonist) | First-line; once daily nocturnal; SE: iris pigmentation, lash growth, periorbital fat atrophy |
| Beta-blockers | Timolol, betaxolol | ↓ Aqueous secretion (β2 blockade on ciliary epithelium) | Avoid in asthma, COPD, heart block; betaxolol = selective β1 |
| Alpha-2 agonists | Brimonidine, apraclonidine | ↓ Aqueous secretion + ↑ uveoscleral outflow | SE: allergy, fatigue, dry mouth; avoid in children (<2 yrs — CNS depression) |
| Carbonic anhydrase inhibitors | Dorzolamide (topical), acetazolamide (systemic) | ↓ Aqueous secretion (inhibit CA-II in ciliary epithelium → ↓ HCO₃⁻ → ↓ aqueous) | Acetazolamide IV in acute angle closure; SE: sulphonamide allergy, renal stones, paraesthesia |
| Miotics (cholinergics) | Pilocarpine | ↑ Trabecular outflow (ciliary muscle contraction opens trabecular spaces) | Angle-closure emergency; SE: brow ache, miosis, myopia |
| Rho kinase inhibitors | Netarsudil | ↑ Trabecular outflow + ↓ aqueous secretion | Newer agent; SE: conjunctival hyperaemia |
B. Age-Related Macular Degeneration (Wet AMD) — Anti-VEGF
| Drug | Type | Dose |
|---|---|---|
| Ranibizumab (Lucentis) | Anti-VEGF Fab fragment | Intravitreal monthly → PRN |
| Bevacizumab (Avastin) | Anti-VEGF full antibody (off-label) | Intravitreal; cheaper alternative |
| Aflibercept (Eylea) | VEGF trap (VEGF-A, VEGF-B, PlGF) | Intravitreal; 2-monthly after loading |
| Faricimab (Vabysmo) | Anti-VEGF-A + anti-Ang2 bispecific | Intravitreal; up to 4-monthly |
| Brolucizumab (Beovu) | Anti-VEGF scFv | Intravitreal; up to 3-monthly; retinal vasculitis risk |
C. Diabetic Macular Oedema (DMO) — Same anti-VEGF drugs; also:
- Intravitreal corticosteroids: dexamethasone implant (Ozurdex), fluocinolone acetonide (Iluvien) — for pseudophakic or unresponsive cases; SE: cataract + raised IOP
D. Infection / Inflammation
| Drug | Indication |
|---|---|
| Chloramphenicol (topical) | Bacterial conjunctivitis (broad-spectrum; first-line UK) |
| Ciprofloxacin / ofloxacin (topical) | Bacterial keratitis (corneal ulcer) |
| Aciclovir (topical + oral) | HSV keratitis; herpes zoster ophthalmicus |
| Ganciclovir (intravitreal) | CMV retinitis (immunocompromised) |
| Topical steroids (prednisolone, dexamethasone) | Anterior uveitis, scleritis, post-surgical inflammation |
| Topical cyclosporin (Restasis) | Dry eye disease (immunomodulatory) |
| Pyrimethamine + sulfadiazine + folinic acid | Ocular toxoplasmosis |
⚠️ Steroids in the eye: can cause steroid-induced glaucoma (IOP rise) and posterior subcapsular cataract with prolonged use
E. Mydriatics / Cycloplegics
| Drug | Type | Duration | Use |
|---|---|---|---|
| Tropicamide 1% | Anticholinergic (short) | 4–6 hours | Routine fundal examination |
| Cyclopentolate 1% | Anticholinergic | 12–24 hours | Refraction in children; uveitis (prevents posterior synechiae) |
| Atropine 1% | Anticholinergic (long) | 1–2 weeks | Amblyopia treatment; severe uveitis |
| Phenylephrine 2.5–10% | Sympathomimetic | 4–6 hours | Mydriasis without cycloplegia; combined with tropicamide for fundoscopy |
⚠️ Avoid mydriatics in known narrow angles — risk of precipitating acute angle closure
F. Lubricants (Dry Eye Disease)
| Drug | Type | Notes |
|---|---|---|
| Hypromellose, carbomers | Viscosity-based drops | Most common; OTC |
| Sodium hyaluronate | Viscoelastic | Retains moisture; good for moderate dry eye |
| Lipid-containing drops | Liposomal sprays | Evaporative dry eye (Meibomian dysfunction) |
| Ciclosporin A 0.1% (Ikervis) | Immunomodulatory | Severe dry eye; reduces T-cell-mediated inflammation of lacrimal gland |
Summary Table
| Domain | Key Highlights |
|---|---|
| Surface Anatomy | Palpebral fissure, limbus, lacrimal puncta, canthi, Meibomian glands, tear film 3 layers |
| Regional Anatomy | 3 coats: sclera/cornea → uvea → retina; anterior/posterior segments; EOM supply LR6SO4 |
| Gross Anatomy | Cornea 5 layers; optic nerve 4 segments + meningeal sheaths → papilloedema; lens crystallins |
| Histology | Retina 10 layers; Reinke — no, Reinke's is larynx; RPE phagocytoses outer segments; corneal endothelium doesn't regenerate |
| Physiology | Aqueous cycle via Canal of Schlemm; accommodation (CN III); phototransduction via cGMP-gated channels; visual pathway + field defects |
| Biochemistry | Visual cycle needs Vit A; crystallins prevent aggregation; polyol pathway → diabetic cataract; prostaglandins ↑ uveoscleral outflow |
| Pathology | POAG (painless); acute angle closure (painful + vomiting); AMD wet (VEGF-driven); CRAO (cherry-red spot); RP (bone spicules) |
| Microbiology | Adenovirus = most common conjunctivitis; Chlamydia A–C = trachoma; HSV = dendritic ulcer; Bacillus cereus = soil injury endophthalmitis |
| Clinical | Red eye differential (pain/vision/discharge/pupil/IOP); RAPD swinging flashlight; fundal grading for diabetic retinopathy |
| Medicine | OCT for retinal layers; FFA for vasculature; Goldmann tonometry for IOP; ERG for RP |
| Pharmacology | Prostaglandins = 1st-line glaucoma; anti-VEGF intravitreal for wet AMD/DMO; aciclovir for HSV; steroids → steroid glaucoma + PSC cataract |
abdomen, hepatobiliary for surgery