Hepato renal syndrome in details
Reading File
Finding Sources
Searching PubMed
"hepatorenal syndrome"[MeSH Terms] AND diagnosis AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information to write a thorough, well-structured answer. Let me compile everything.
Hepatorenal Syndrome (HRS) - Detailed Review
Definition
Hepatorenal syndrome (HRS) is a form of functional renal failure - occurring in patients with advanced cirrhosis or acute liver failure - in which there is no identifiable intrinsic renal pathology. The kidneys are histologically normal; function can be restored by liver transplantation, correction of portal hypertension, or in some cases medical therapy. Notably, kidneys from HRS patients transplanted into non-cirrhotic recipients have been shown to regain function.
- Sleisenger and Fordtran's GI and Liver Disease, p. 1818
Epidemiology
- Acute renal dysfunction occurs in 15-25% of hospitalized patients with cirrhosis
- HRS accounts for 10-30% of those cases
- Annual frequency of HRS in cirrhotic patients with ascites: roughly 8%, and up to 40% in some reports
- HRS develops in approximately 30% of cirrhotic patients admitted with spontaneous bacterial peritonitis (SBP) or other infection
- 25% of those hospitalized with severe alcoholic hepatitis
- 10% who require serial large-volume paracenteses
Classification (Updated Nomenclature - ICA 2015)
The International Club of Ascites (ICA) renamed the two traditional types in 2015:
| Old Term | New Term | Characteristics |
|---|---|---|
| Type 1 HRS | HRS-AKI (Acute Kidney Injury) | Rapid, progressive renal failure over 1-2 weeks; previously required Cr >2.5 mg/dL - now defined by ICA-AKI criteria (Stage 2-3 AKI) |
| Type 2 HRS | HRS-CKD (Chronic Kidney Disease) | Slower, more gradual course; associated with refractory ascites; better prognosis than HRS-AKI |
HRS-AKI is defined as:
- Meets all 6 HRS diagnostic criteria (see below)
- Rise in serum creatinine of ≥0.3 mg/dL within 48 hours, OR a 1.5x rise from baseline within 7 days
The older Type 1 requirement for an absolute creatinine >2.5 mg/dL has been removed because patients with cirrhosis often have profound muscle wasting and reduced urea synthesis, which lowers serum creatinine and can delay recognition.
HRS-NAKI (non-AKI, formerly Type 2) is now also recognized - characterized by gradual deterioration and diuretic-resistant ascites.
Pathophysiology
The pathophysiology involves three key, interrelated components:
1. Splanchnic and Systemic Arterial Vasodilation
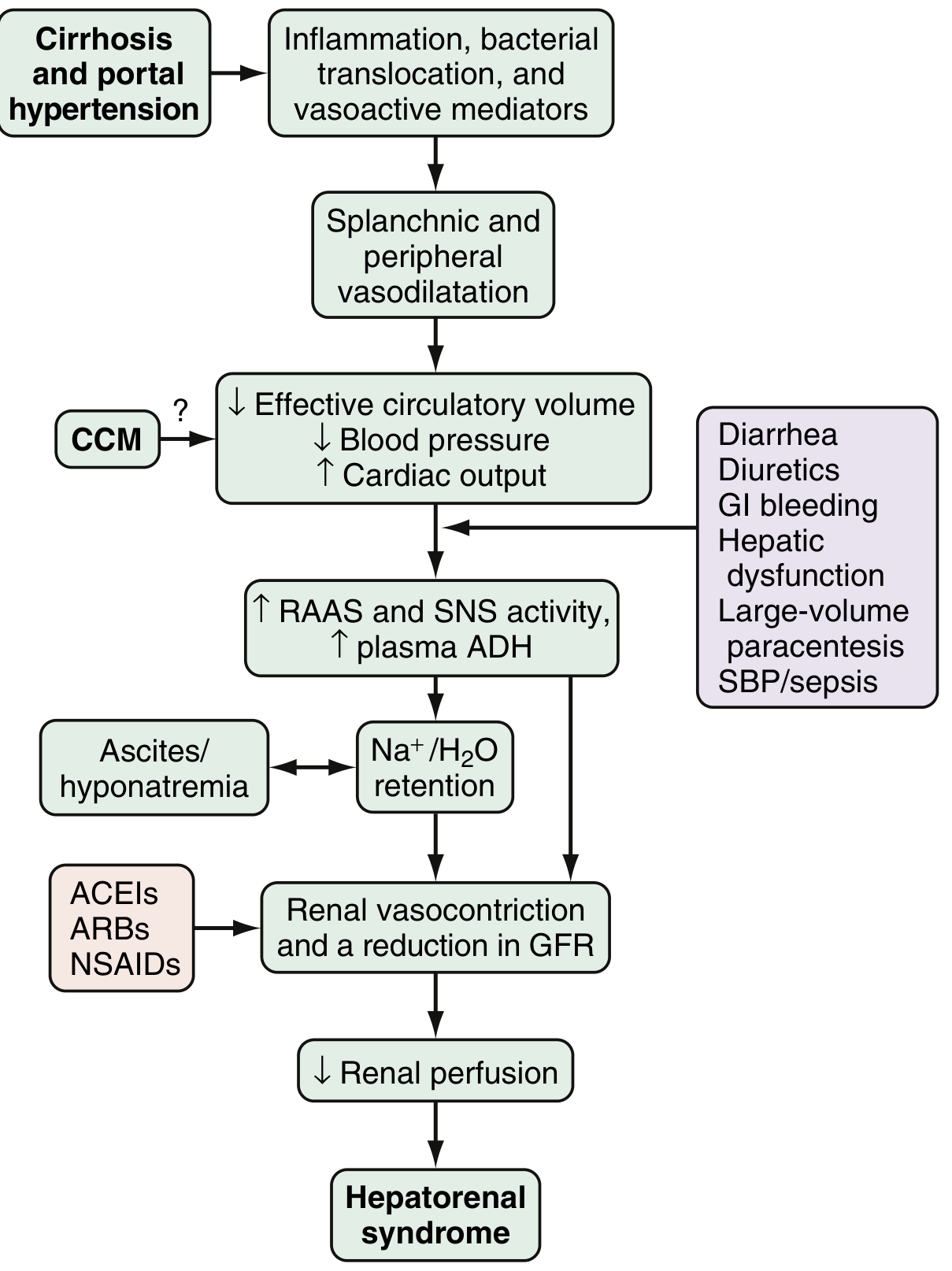
Fig. 94.2 - Proposed pathophysiology and triggers of HRS (from Sleisenger & Fordtran)
- Portal hypertension triggers release of vasoactive mediators: nitric oxide (NO), carbon monoxide (CO), glucagon, prostacyclin, adrenomedullin, and endogenous opiates
- These cause splanchnic and peripheral vasodilation
- In early portal hypertension: increased heart rate and cardiac output compensate (hyperdynamic circulation)
- As liver disease progresses, this compensation fails
2. Compensatory Renal Vasoconstriction
When effective circulatory volume falls, compensatory systems activate:
- Sympathetic nervous system (SNS) activation
- Renin-angiotensin-aldosterone system (RAAS) activation
- Non-osmotic ADH release (arginine vasopressin) - increased secretion + decreased clearance
- Intrarenal mediators: altered endothelins, prostaglandins, kallikreins, F2-isoprostanes
The balance between vasoconstrictive responses in the kidney and systemic/splanchnic vasodilation is ultimately lost - leading to marked increase in renal vascular resistance, decreased renal perfusion, and reduced GFR.
If intense renal vasoconstriction is sustained, tubular damage can occur, converting HRS from a purely functional syndrome to organic renal disease.
3. Cirrhotic Cardiomyopathy (CCM)
Cardiac dysfunction in cirrhosis reduces effective cardiac output further, compounding renal hypoperfusion.
Precipitating Events
Common triggers (see the pathophysiology diagram):
- SBP / sepsis (most common)
- GI bleeding
- Large-volume paracentesis without albumin
- Diuretics
- Nephrotoxic drugs (NSAIDs, ACE inhibitors, ARBs)
- Hepatic dysfunction / acute-on-chronic liver failure
Diagnostic Criteria (ICA 2015 Revised Criteria)
HRS is a diagnosis of exclusion. The following 6 criteria must all be met:
- Cirrhosis with ascites
- AKI by ICA criteria - rise in Cr ≥0.3 mg/dL in <48 h OR ≥50% rise from baseline in 7 days
- No response after ≥2 days of diuretic withdrawal AND volume expansion with albumin (1 g/kg/day up to 100 g/day)
- Absence of shock
- No current or recent nephrotoxic agents (NSAIDs, ACE inhibitors, ARBs, contrast agents)
- No parenchymal kidney disease - proteinuria <500 mg/day, no microhematuria (>50 RBC/HPF), normal renal ultrasound
AKI Staging in Cirrhosis (ICA-AKI)
| Stage | Definition |
|---|---|
| Stage 1 | Cr rise ≥0.3 mg/dL OR ≥1.5- to 2-fold above baseline |
| Stage 2 | Cr rise >2-fold to 3-fold above baseline |
| Stage 3 | Cr rise >3-fold above baseline OR Cr ≥4 mg/dL with acute rise ≥0.3 mg/dL OR initiation of renal replacement therapy |
HRS-AKI = Stage 2 or 3 AKI meeting all criteria above.
Clinical Features
- Most patients are asymptomatic except for decreased urine output
- Oliguria is common but not a diagnostic criterion (patients with cirrhosis are frequently oliguric at baseline due to sodium retention, even with preserved GFR)
- May present with hepatic encephalopathy (HE) as the first sign of HRS
- Rising serum creatinine and BUN
- Urine findings (preserved tubular function): urine Na <10 mmol/L, urine osmolality > plasma osmolality
Differential Diagnosis
| Cause | Key Feature |
|---|---|
| Pre-renal azotemia | Responds to volume expansion |
| Acute tubular necrosis (ATN) | Urine Na >20, granular casts, elevated urinary biomarkers (IL-18, NGAL) |
| Contrast nephropathy | Recent contrast exposure |
| Drug-induced (NSAIDs, ACE-i) | Recent drug history |
| Glomerulonephritis | Proteinuria, hematuria |
| Obstructive uropathy | Abnormal renal US |
Urinary biomarkers (IL-18, NGAL, EGF, fatty acid-binding protein 2) can help distinguish ATN from HRS, though not yet in routine clinical use.
Management (Box 94.3 - Sleisenger & Fordtran)
Prevention
- Prevent variceal bleeding with beta-blockers or band ligation
- Albumin (1.5 g/kg at diagnosis, then 1 g/kg on day 3) in all patients with SBP - reduces incidence of HRS by ~60%
- Albumin infusion with large-volume paracentesis (6-8 g per liter drained for >5 L)
- Norfloxacin prophylaxis in cirrhotic patients at high risk (prevents bacterial translocation)
- Avoid nephrotoxins: NSAIDs, ACE inhibitors, ARBs, aminoglycosides
Initial Steps (All Patients with AKI)
- Stop diuretics
- Volume expansion with IV albumin 1 g/kg/day for 48 h
- Treat any precipitating event (e.g., antibiotics for SBP/infection)
- Evaluate for and treat GI bleeding
- Discontinue nephrotoxic drugs
Pharmacologic Treatment of HRS-AKI
| Agent | Role | Notes |
|---|---|---|
| Terlipressin (vasopressin analog) | First-line vasoconstrictor | Reduces splanchnic vasodilation; FDA approved (2022); IV bolus or continuous infusion; risk of respiratory failure and ischemic complications |
| Norepinephrine | Alternative (1st line where terlipressin unavailable) | Requires ICU monitoring; alpha-agonist; similar efficacy to terlipressin in some studies |
| Midodrine + Octreotide + Albumin | Third-line option (used in the US when above not available) | Less effective; midodrine is an alpha-agonist, octreotide inhibits glucagon release |
| IV Albumin | Used with all vasoconstrictors | Enhances volume expansion; 20-40 g/day |
A 2024 meta-analysis (PMID 38285703) found terlipressin and norepinephrine have comparable efficacy for HRS-AKI reversal, though terlipressin showed greater reversal of HRS with some increase in respiratory adverse events.
Non-Pharmacologic / Procedural
- Transjugular intrahepatic portosystemic shunt (TIPS): reduces portal pressure and can improve renal function, especially in HRS-CKD (Type 2). Contraindicated in severe hepatic insufficiency.
- Renal replacement therapy (RRT/hemodialysis): For patients with AKI stage 3 or refractory HRS - used as a bridge to transplant, not a definitive therapy
- Molecular Adsorbent Recirculating System (MARS): albumin dialysis; limited evidence, used in acute-on-chronic liver failure
Definitive Therapy
Liver transplantation is the only definitive cure. Recovery of renal function typically occurs after transplantation. Combined liver-kidney transplant (SLKT) is considered when renal recovery after liver transplantation is unlikely (e.g., prolonged HRS, Cr >4 mg/dL, RRT >6 weeks).
Prognosis
- Without treatment, median survival in HRS-AKI is <2 weeks (historically, 2 weeks for type 1 HRS)
- HRS-CKD has a longer course but still poor prognosis without transplantation
- Response to vasoconstrictors improves short-term survival
- In patients transplanted for HRS, renal function typically recovers and outcomes are comparable to non-HRS transplant patients
Recent Evidence
- Terlipressin vs. norepinephrine meta-analysis (2024) - PMID 38285703 - comparable efficacy with terlipressin showing higher HRS reversal rates
- AGA Clinical Practice Update 2024 on vasoactive drugs and albumin - PMID 37978969 - emphasizes terlipressin as primary treatment, confirms role of albumin
- Continuous vs. bolus terlipressin meta-analysis (2026) - PMID 41853888 - continuous infusion may have better safety profile
Summary
| Feature | HRS-AKI (Type 1) | HRS-CKD (Type 2) |
|---|---|---|
| Onset | Rapid (days-weeks) | Gradual (months) |
| Creatinine | Rises rapidly | Stable elevation |
| Precipitant | Often SBP, sepsis, bleeding | Refractory ascites |
| Prognosis | Poor (weeks without treatment) | Better than AKI, still poor long-term |
| Treatment | Terlipressin/NE + albumin | TIPS; transplantation |
Key teaching points:
- HRS kidneys are histologically normal - it is a functional, potentially reversible disorder
- Removal of nephrotoxins and albumin challenge are mandatory before diagnosis
- Terlipressin is now FDA-approved and preferred first-line vasoconstrictor
- Liver transplantation remains the definitive treatment
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine; Rosen's Emergency Medicine; Current Surgical Therapy 14e
This is a shared conversation. Sign in to Orris to start your own chat.