what are the options for patients with type ii submucous myomas who have failed medical therapy and desire to retain fertility?
Reading File
Finding Sources
Finding Sources
Searching PubMed
submucous myoma hysteroscopic myomectomy fertility
Finding Sources
Finding Sources
Searching PubMed
submucosal fibroid myomectomy fertility preservation
Finding Sources
Finding Sources
Searching PubMed
hysteroscopic myomectomy type 2 submucosal fibroid two-step
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Searching the Web
type II submucosal myoma failed medical therapy fertility options hysteroscopic two-step staged resection
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information needed for a complete, authoritative answer. Here it is:
Type II Submucous Myoma: Options After Failed Medical Therapy in Fertility-Preserving Patients
Background: What Makes Type II Difficult
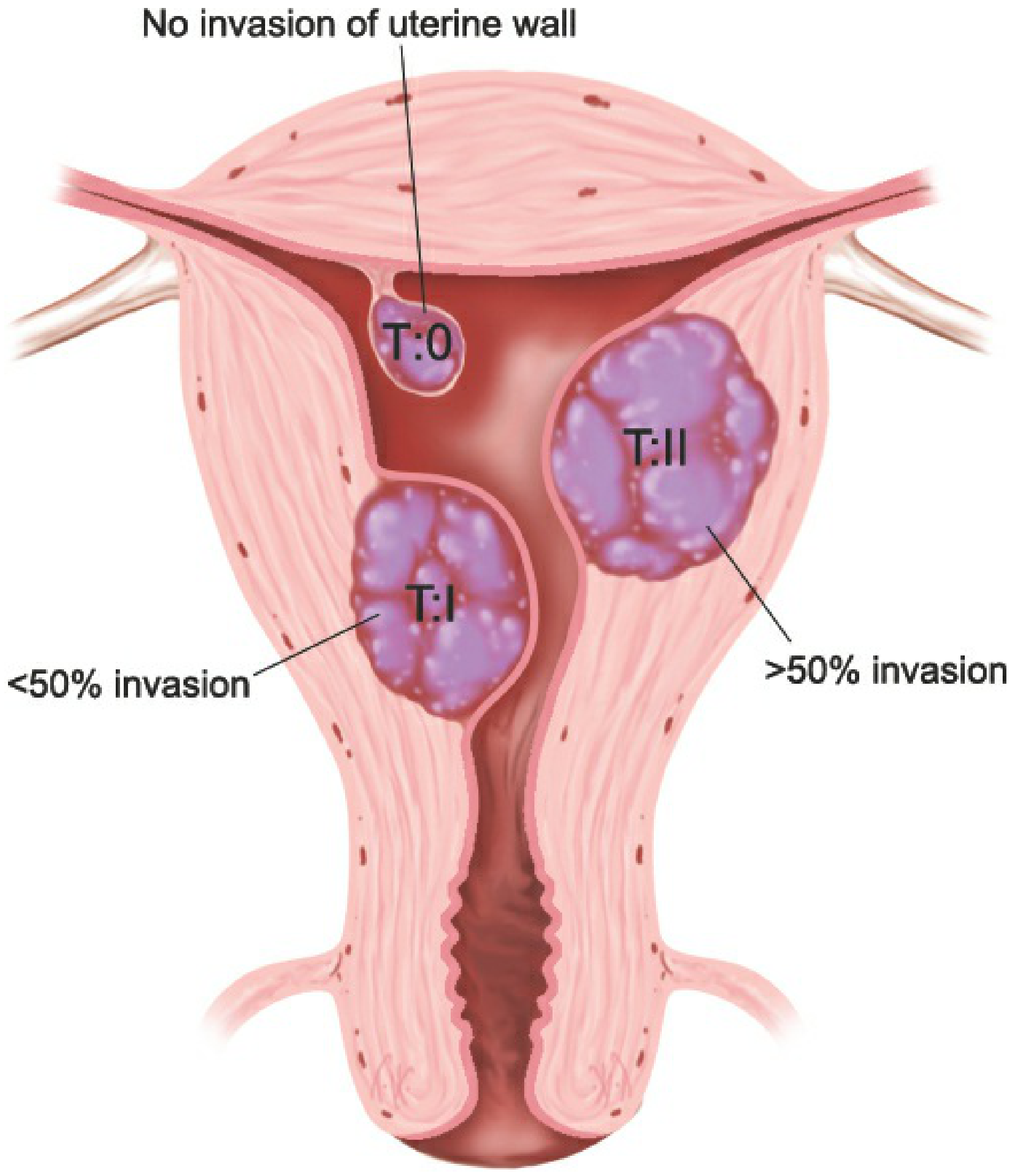
By the FIGO classification, a Type II (G2) submucosal myoma has ≥50% of its volume embedded within the myometrium, with less than half projecting into the uterine cavity. This is the most technically challenging submucosal subtype to manage.
A meta-analysis found that submucosal fibroids with uterine cavity distortion decrease ongoing pregnancy/live birth rates by 70% (RR 0.32), and resection improves those rates - making intervention appropriate for fertility-seeking patients who have failed medical therapy. - Berek & Novak's Gynecology
Surgical Options (Primary Approach)
1. Hysteroscopic Myomectomy - Two-Stage (Staged) Procedure
This is the preferred first approach for Type II myomas, though it is more complex than for Types 0 and 1. Because less than half the fibroid protrudes into the cavity, complete single-session resection carries elevated risks:
- Fluid absorption and hyponatremia (from prolonged distension time)
- Uterine perforation (risk increases directly with depth of myometrial involvement)
- Insufficient myometrial margin (especially if <5 mm between fibroid and serosa)
Staged approach:
- First session: Resect the intracavitary portion down to the level of the surrounding myometrium
- Interval: A GnRH analogue is typically given between procedures (approximately 6-8 weeks apart); uterine contractions often expel the remaining intramural portion into the cavity
- Second session: Complete the resection of the now-intracavitary residual fibroid
Complete resection is achievable but requires more repeat procedures than Types 0 and 1. Preoperative SIS or MRI is mandatory to gauge the thickness of normal myometrium between the fibroid and the serosa. - Berek & Novak's Gynecology, p. 532-533
Note: One RCT found that hysteroscopic myomectomy improved fertility rates for Type 0 and Type 1 myomas but did not show a statistically significant benefit for Type II - though the evidence is limited by small numbers. (IntechOpen review)
2. Hysteroscopic Tissue Removal (HTR) / Intrauterine Morcellation Systems
An alternative to the classic electrosurgical resectoscope. HTR systems (e.g., MyoSure, TRUCLEAR) use mechanical morcellation in physiologic saline (bipolar-compatible). A systematic review of 8 studies with 283 women showed:
- Complete resection rates comparable to resectoscopic surgery
- No significant intra- or postoperative complications at a fluid deficit of up to 2,500 mL of isotonic solution
- Type 0 and Type 1 fibroids are easier; Type 2 remains more challenging with HTR systems as well
- Berek & Novak's Gynecology, p. 533
Advantages include use with normal saline (reduces hyponatremia risk) and potentially faster resection of softer tissue components.
3. Preoperative Medical Pretreatment Before Hysteroscopy
While the question specifies failure of medical therapy for symptom control, short-course medical pretreatment specifically before surgery is a different use-case and can still be employed:
- GnRH analogues (e.g., leuprolide): 2-3 months preoperatively - reduce fibroid vascularity and uterine size, correct anemia, and may shift the type II fibroid toward a more favorable position (some intramural component may become intracavitary)
- Mifepristone / SPRMs: Used in some protocols (particularly in Asia) as preoperative conditioning to reduce myoma size and facilitate safer hysteroscopic removal - a recent 2025 case report described HIFU combined with mifepristone as pretreatment for a 42x41 mm Type II myoma in a fertility-seeking patient to enable single-session hysteroscopy
- HIFU (High-Intensity Focused Ultrasound) as pretreatment: Not the same as standalone therapy - used to pre-ablate and reduce the intramural component, making hysteroscopic removal safer and more complete
4. Laparoscopic (or Abdominal) Myomectomy
For Type II myomas - especially large ones (>4-5 cm), those with very thin overlying myometrium, or where hysteroscopy is predicted to fail or be unsafe - laparoscopic myomectomy is an appropriate fertility-preserving surgical option. An experienced laparoscopic surgeon can remove the fibroid with a multilayered myometrial closure, which is preferable for preserving uterine integrity for future pregnancy. - Berek & Novak's Gynecology, pp. 347-355
Abdominal (open) myomectomy remains an option for very large or multiple fibroids where laparoscopic access is limited.
5. Combined Hysteroscopic + Laparoscopic Approach
For very large Type II fibroids or those approaching the serosa (<5 mm myometrial margin), a simultaneous laparoscopic-hysteroscopic approach can be employed:
- Laparoscopy provides real-time visualization of the uterine serosa to prevent perforation
- Allows immediate repair if perforation occurs
- Particularly useful when the remaining myometrial wall is thin
Pre-Procedural Evaluation (Mandatory for Type II)
Before any intervention, obtain:
- Saline infusion sonography (SIS) or MRI to map fibroid depth, estimate intramural extension, and measure the myometrium-to-serosa distance (must be >5 mm for safe hysteroscopy)
- Hemoglobin - correct anemia preoperatively if present (use GnRH analogue or iron supplementation)
- Counsel patient that a two-stage procedure is likely and repeat surgery may be needed
Options NOT Recommended for Fertility-Seeking Patients
| Option | Reason to Avoid |
|---|---|
| Endometrial ablation | Destroys endometrium; precludes pregnancy |
| UAE (uterine artery embolization) | Associated with reduced ovarian reserve, increased miscarriage, preterm birth |
| MRgHIFU as definitive treatment | Specifically not recommended for women wishing future fertility |
| Hysterectomy | Not applicable - patient desires fertility |
Summary
For a fertility-seeking patient with a Type II submucosal myoma who has failed medical therapy, the options in order of preference are:
- Two-stage hysteroscopic myomectomy (with GnRH analogue between stages) - preferred when fibroid is ≤5 cm and myometrial margin is adequate
- HTR/intrauterine morcellator as an alternative to resectoscope
- Medical pretreatment (GnRH analogue, mifepristone, or HIFU) followed by hysteroscopic resection - to reduce size and improve access
- Laparoscopic myomectomy - for large fibroids, inadequate myometrial margin, or anticipated hysteroscopic failure
- Combined laparoscopic + hysteroscopic - for cases with high perforation risk
Preoperative MRI or SIS is mandatory to determine which surgical route is safest. Patient counseling should include realistic expectations: Type II fibroids have lower complete single-session resection rates and less certain fertility benefit than Types 0 and 1.
Sources: Berek & Novak's Gynecology (Berek & Novak's Gynecology, pp. 531-533); IntechOpen hysteroscopic surgery for submucosal fibroids; SLS Hysteroscopic Myomectomy chapter
This is a shared conversation. Sign in to Orris to start your own chat.