pain on elbow fexion shouder abduction past from 6 minths shoulfder pain wha tis pt ,angemnt
Reading File
search_medical_text
shoulder pain elbow flexion abduction 6 months diagnosis differential
search_medical_text
chronic shoulder pain abduction management physiotherapy treatment
GradeResponse
GradeResponse
Based on the retrieved content and clinical knowledge, here is a comprehensive answer:
Likely Diagnosis
Pain on elbow flexion + shoulder abduction for 6 months is the classic presentation of bicipital tendinopathy (biceps tendinitis/tendinosis), often coexisting with rotator cuff impingement or subacromial bursitis.
The combination of:
- Pain on shoulder abduction → subacromial impingement / rotator cuff pathology
- Pain on elbow flexion → biceps tendon (long head) involvement
- 6 months duration → chronic / subacute presentation
...strongly suggests bicipital tendinitis ± rotator cuff impingement syndrome, with possible adhesive capsulitis developing if range of motion is significantly restricted.
Differential Diagnosis
| Condition | Key Feature |
|---|---|
| Bicipital tendinitis | Anterior shoulder pain, worse with elbow flexion & forearm supination |
| Rotator cuff impingement | Pain on abduction (60–120° arc), positive Neer/Hawkins test |
| Subacromial bursitis | Diffuse shoulder pain, worse at night |
| Adhesive capsulitis (Frozen shoulder) | Global ROM restriction, progressive stiffness |
| Rotator cuff tear (partial/full) | Weakness, positive drop arm test |
| Acromioclavicular joint arthritis | Pain at AC joint, cross-arm adduction test |
| Cervical radiculopathy (C5–C6) | Neck pain, neurological signs (sensory/reflex changes) |
Per Harrison's Principles of Internal Medicine (p. 631): Mechanical shoulder pain is often worse at night, aggravated by passive abduction, internal rotation, or extension of the arm. If neurological signs are absent, the differential includes bicipital tendinitis, frozen shoulder, bursitis, rotator cuff tear, and impingement.
Clinical Tests to Perform
- Speed's test — resisted forward flexion with elbow extended; positive = anterior shoulder pain → bicipital tendinitis
- Yergason's test — resisted supination with elbow at 90°; positive = bicipital groove pain
- Neer's sign — passive forward flexion with internal rotation; positive = impingement
- Hawkins-Kennedy test — internal rotation at 90° abduction; positive = impingement
- Empty can test — weakness/pain = supraspinatus tear
- Painful arc — pain between 60–120° = subacromial pathology
Investigations
| Investigation | Purpose |
|---|---|
| X-ray shoulder (AP + outlet view) | Bony pathology, acromion morphology, calcific deposits |
| Ultrasound shoulder | First-line for tendon pathology, bursitis, rotator cuff tears — dynamic assessment |
| MRI shoulder | Gold standard for rotator cuff, labrum, capsule, tendon detail |
| Cervical spine X-ray / MRI | If radiculopathy suspected (C5/C6) |
Patient Management
1. Conservative (First-line, 6–12 weeks)
- Activity modification — avoid provocative movements (overhead work, heavy lifting)
- NSAIDs — oral (e.g., ibuprofen 400–600 mg TID, naproxen 500 mg BD) for 2–4 weeks
- Physiotherapy — cornerstone of management:
- Rotator cuff strengthening
- Scapular stabilization exercises
- Posterior capsule stretching
- Pendulum exercises if ROM limited
- Ice/Heat — ice in acute flares, heat for chronic stiffness
2. Injection Therapy (if inadequate response at 4–6 weeks)
- Subacromial corticosteroid injection — for bursitis/impingement (ultrasound-guided preferred)
- Bicipital groove injection — for isolated bicipital tendinitis (peritendinous, NOT intratendinous)
- Limit to 2–3 injections; avoid repeated injections (tendon rupture risk)
3. Surgical Referral (if conservative fails at 3–6 months)
- Arthroscopic subacromial decompression (acromioplasty) for refractory impingement
- Rotator cuff repair if tear confirmed on imaging
- Biceps tenodesis or tenotomy for recalcitrant bicipital tendinopathy
Red Flags to Rule Out
| Flag | Think of |
|---|---|
| Significant weakness, wasting | Rotator cuff tear, cervical myelopathy |
| Radicular symptoms (numbness, tingling) | C5–C6 radiculopathy |
| Constitutional symptoms (fever, weight loss) | Septic arthritis, malignancy (Pancoast tumor) |
| Night pain unrelated to position | Malignancy |
| History of trauma | Fracture, dislocation |
Bottom line: A 6-month history of shoulder abduction pain + elbow flexion pain most likely represents chronic bicipital tendinitis with rotator cuff impingement. Start with NSAIDs + structured physiotherapy. Obtain shoulder ultrasound or MRI if no improvement in 4–6 weeks. Consider subacromial/bicipital groove injection if conservative measures fail. Refer to orthopaedics if symptoms persist beyond 3–6 months of optimal conservative management.
bicipital tendoitis
search_medical_text
bicipital tendinitis diagnosis clinical features tests treatment
search_medical_image
bicipital tendinitis shoulder anatomy biceps tendon
GradeResponse
GradeResponse
Bicipital Tendinitis (Long Head of Biceps Tendinitis)
Anatomy & Pathophysiology
The long head of the biceps tendon (LHBT) originates from the supraglenoid tubercle, passes through the bicipital groove of the humerus, and is covered by a synovial sheath. It is vulnerable to:
- Repetitive overhead activity (throwing, swimming, weightlifting)
- Impingement from adjacent structures (acromion, rotator cuff)
- Instability — tendon slipping out of the bicipital groove
- Degenerative change (tendinosis in chronic cases)
The result is anterior shoulder pain from inflammation or degeneration of the tendon/sheath.
Clinical Features
| Feature | Detail |
|---|---|
| Pain location | Anterior shoulder, over bicipital groove |
| Character | Deep, throbbing ache |
| Radiation | May radiate down anterior arm to elbow |
| Aggravating factors | Overhead activity, elbow flexion, forearm supination, lifting |
| Tenderness | Over bicipital groove with arm in 10° internal rotation |
| Night pain | Common |
| Associated findings | Often coexists with rotator cuff impingement or SLAP tear |
Clinical Tests
| Test | How to Perform | Positive Finding |
|---|---|---|
| Upper Cut Test (best screening) | Patient resists upward punch from waist; examiner resists | Pain/click in bicipital groove |
| Speed's Test (confirmatory) | Resist forward flexion with elbow extended, palm up | Anterior shoulder pain |
| Yergason's Test (confirmatory) | Resist supination with elbow flexed at 90° | Bicipital groove pain |
| Ludington's Test | Clasp hands behind head, contract biceps | Pain or weakness at groove |
Per Chronic Shoulder Pain Guidelines (p. 6): The upper cut test should be used as the screening test, and Speed's + Yergason's as confirmatory tests for biceps tendon disorders.
MRI Findings
The MRI below shows classic bicipital tendinitis — increased signal intensity and thickening of the LHBT in the bicipital groove (axial view), with an intact rotator cuff (coronal view):
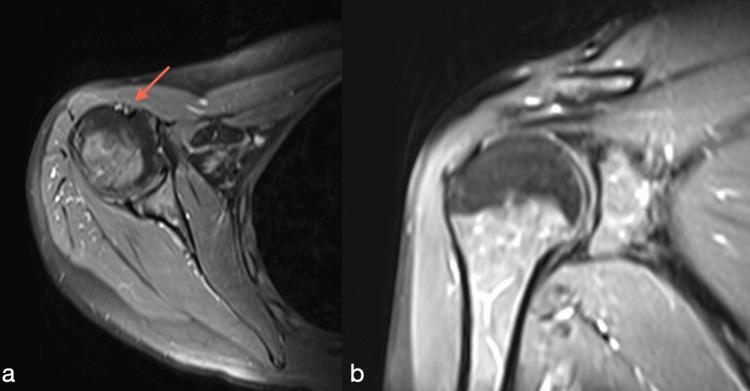
Investigations
| Investigation | Purpose |
|---|---|
| Ultrasound | First-line — fluid in tendon sheath, tendon thickening, dynamic instability |
| MRI shoulder | Gold standard — differentiates tendinitis vs. partial/complete tear vs. SLAP lesion |
| X-ray | Excludes bony pathology, calcification |
Management
Step 1 — Conservative (4–6 weeks, first-line)
- Rest + activity modification — avoid overhead and repetitive arm use
- NSAIDs — ibuprofen 400–600 mg TID or naproxen 500 mg BD for 2–4 weeks
- Ice (acute) / Heat (chronic stiffness)
- Physiotherapy:
- Pendulum exercises (early)
- Rotator cuff strengthening (supraspinatus, infraspinatus)
- Biceps eccentric exercises
- Scapular stabilization
- Posterior capsule stretching
Step 2 — Injection Therapy (if no improvement at 4–6 weeks)
- Peritendinous corticosteroid injection into the bicipital groove sheath (ultrasound-guided preferred)
- Avoid intratendinous injection — risk of tendon rupture
- Limit to 1–2 injections
Step 3 — Surgical (if refractory > 3–6 months)
| Procedure | Indication |
|---|---|
| Biceps tenodesis | Young, active patients — reattach tendon to proximal humerus |
| Biceps tenotomy | Older/less active patients — release tendon (risk: "Popeye" deformity) |
| SLAP repair | If associated SLAP tear confirmed on MRI |
Complications of Untreated Disease
- Progression to tendinosis (degenerative, non-inflammatory)
- Partial or complete tendon rupture — sudden "pop," ecchymosis, Popeye sign (distal biceps bunching)
- Development of adhesive capsulitis (frozen shoulder)
Key Takeaway
Bicipital tendinitis = anterior shoulder pain + elbow flexion/supination pain + bicipital groove tenderness. Diagnose clinically with Speed's/Yergason's/Upper Cut tests, confirm with ultrasound or MRI. Manage conservatively first with NSAIDs + physiotherapy; escalate to injection or surgery if refractory.
postrior capsular stretvh
search_medical_image
posterior capsular stretch shoulder exercise sleeper stretch
GradeResponse
Posterior Capsular Stretch (Sleeper Stretch)
Purpose
Stretches the posterior glenohumeral capsule and the posterior rotator cuff (infraspinatus + teres minor). Tightness in the posterior capsule causes anterior-superior humeral head migration, contributing to:
- Subacromial impingement
- Rotator cuff pathology
- Bicipital tendinitis
- GIRD (Glenohumeral Internal Rotation Deficit) — especially in overhead athletes
Technique — Sleeper Stretch
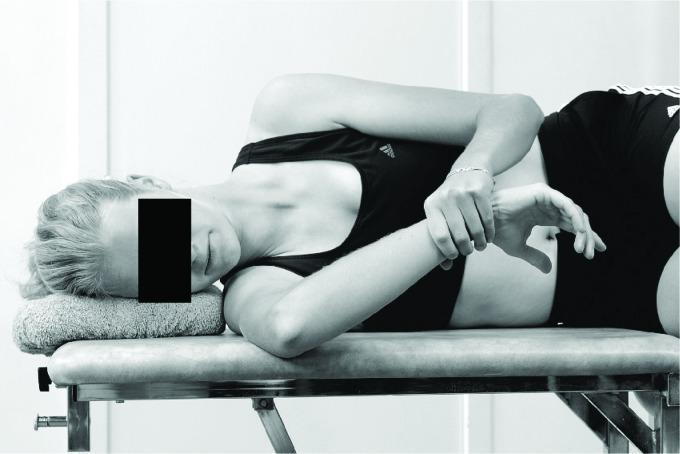
Step-by-step:
- Position — Lie on the affected side (lateral decubitus) with a rolled towel under the head
- Arm position — Affected shoulder abducted to 90°, elbow flexed to 90° (forearm pointing upward)
- Apply stretch — Use the opposite hand to gently press the forearm downward toward the table, promoting passive internal rotation of the glenohumeral joint
- Hold — 30 seconds per repetition
- Repeat — 3–5 reps, 1–2 times daily
Key Points
| Parameter | Detail |
|---|---|
| Target structure | Posterior glenohumeral capsule, infraspinatus, teres minor |
| Position | Side-lying on affected arm |
| Shoulder | 90° abduction |
| Elbow | 90° flexion |
| Force direction | Downward on forearm → internal rotation |
| Hold time | 30 seconds |
| Frequency | 3–5 reps, 1–2× daily |
Important Cautions
- Do not force — stretch should be gentle, a pulling sensation only — no sharp pain
- Avoid if there is an acute rotator cuff tear or shoulder instability (anterior laxity)
- Stabilize the scapula against the table — do not allow it to roll forward (this substitutes scapular movement for true glenohumeral stretch)
- Stop if pain radiates down the arm (may indicate nerve irritation)
Other Posterior Capsule Stretches
| Stretch | Technique |
|---|---|
| Cross-body stretch | Standing, bring affected arm across chest; opposite hand holds elbow and pulls toward opposite shoulder |
| Corner/doorway stretch | Not specific to posterior capsule — more for anterior structures |
The sleeper stretch is preferred over the cross-body stretch for targeting the posterior capsule specifically, as it better isolates glenohumeral internal rotation without scapular compensation.
This is a shared conversation. Sign in to Orris to start your own chat.