Toxic shock syndrome toxin 1
Reading File
Finding Sources
Finding Sources
Searching PubMed
"toxic shock syndrome toxin-1" TSST-1 superantigen
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Here is a detailed synthesis:
Toxic Shock Syndrome Toxin-1 (TSST-1)
Identity and Structure
TSST-1 is a 22 kDa protein exotoxin produced by Staphylococcus aureus. It is identical to what was previously termed enterotoxin F. The gene encoding TSST-1 is located on a chromosomal pathogenicity island that interacts with bacteriophages to regulate toxin production; it is found in approximately 20% of all S. aureus isolates, including MRSA strains.
TSST-1 as the Prototypical Superantigen
TSST-1 is the prototypical superantigen - the canonical example of this class of bacterial toxins.
Mechanism of Superantigen Action
Normal antigen presentation involves a peptide antigen processed and presented within the MHC class II groove, recognized by a complementarity-determining region of a specific T-cell receptor (TCR), activating ~0.001-0.01% of T cells.
TSST-1 bypasses this entirely:
- It binds directly to the outer face of MHC class II molecules (not in the peptide-binding groove) on antigen-presenting cells
- Simultaneously binds to the Vβ domain of the TCR, outside the complementarity-determining regions
- This cross-linking is non-specific, activating 5-25% of all T cells at once
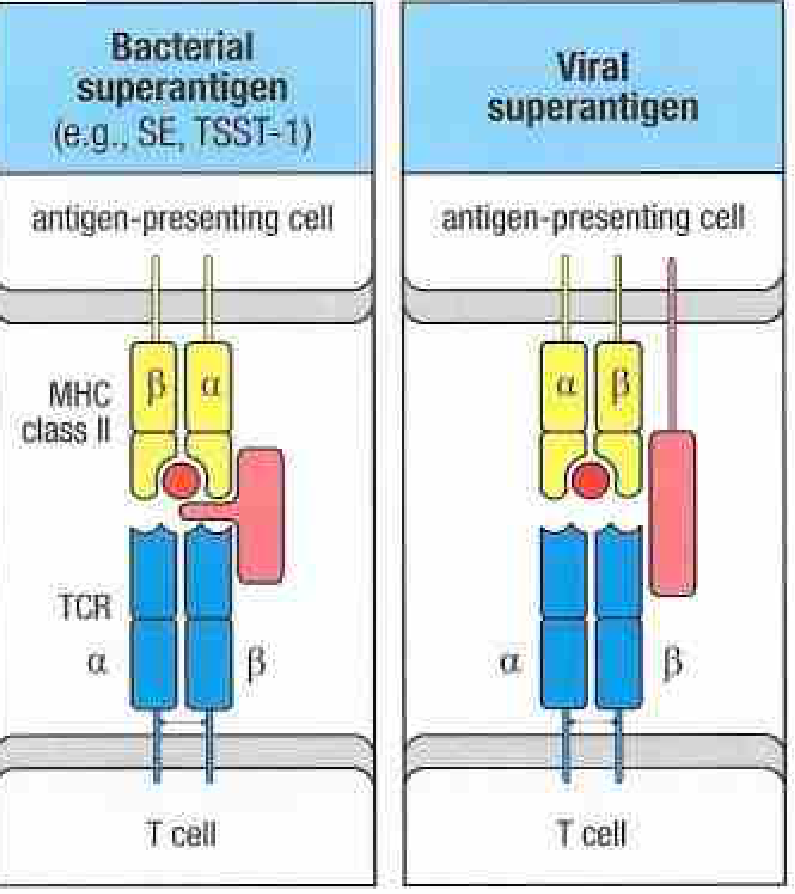
Left: Bacterial superantigens (e.g., SE, TSST-1) bridge MHC class II on the antigen-presenting cell to the TCR Vβ chain on the T cell. Right: Viral superantigens use a similar but distinct bridging mechanism.
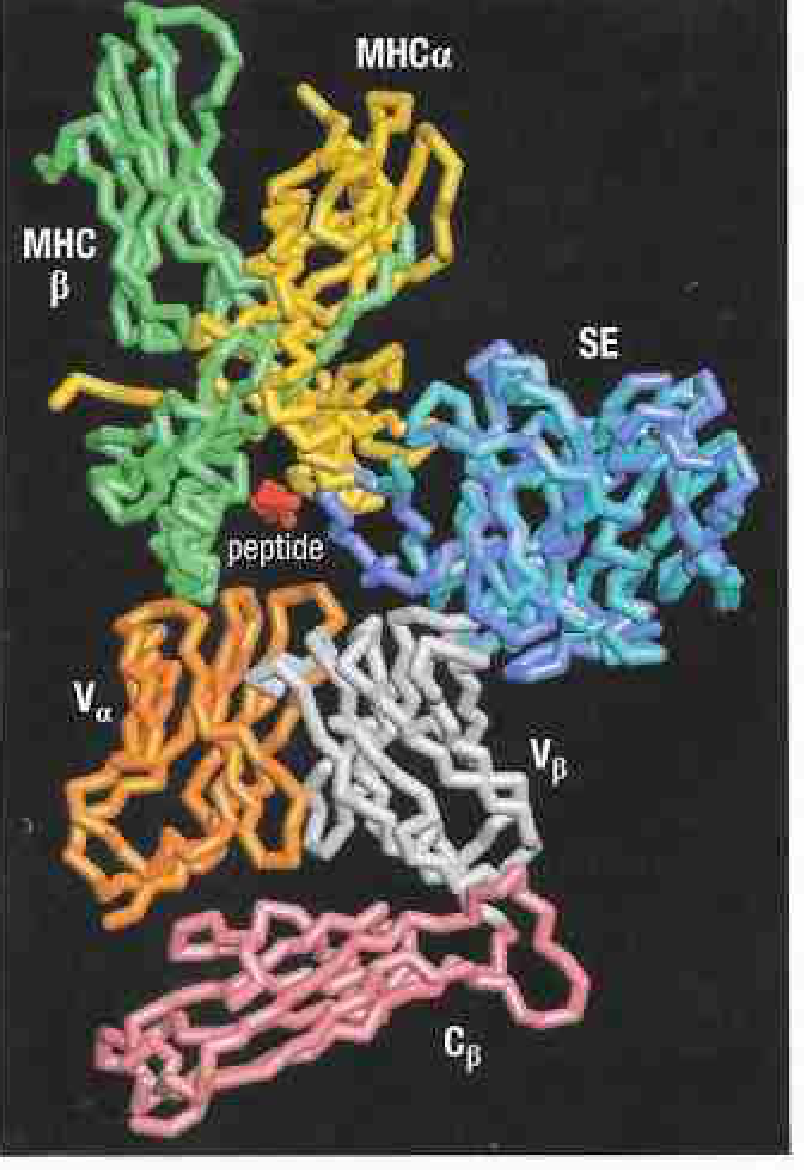
The 3D structure below shows the staphylococcal enterotoxin (SE) binding the MHC class II α chain (yellow) and the TCR Vβ domain (grey/white), with the peptide (red) left undisturbed in the groove:
Consequence - Cytokine Storm
Massive polyclonal T-cell activation results in an enormous release of:
- IL-1, IL-2, TNF-α (from T cells and macrophages)
- IFN-γ
This cytokine storm drives fever, vasodilation, hypotension, and multi-organ dysfunction.
Unique Properties of TSST-1
A feature that distinguishes TSST-1 from other staphylococcal superantigens is its ability to cross mucosal surfaces - this explains why it is uniquely responsible for 100% of menstrual-associated TSS cases (where the vaginal mucosa is the portal of entry), while other enterotoxins (SEA, SEB, SEC) are implicated in nonmenstrual TSS.
Clinical Syndrome: Toxic Shock Syndrome (TSS)
Epidemiology
- TSS was first described in 1978 in children with S. aureus infection
- Gained notoriety with tampon-associated outbreaks in the early 1980s (highly absorbent tampons created a protein-rich, pH-neutralized nidus for toxin production)
- Today, nonmenstrual TSS exceeds menstrual TSS in incidence, following removal of high-absorbency tampons and public education
- Nonmenstrual TSS is associated with: postsurgical wounds, sinusitis, osteomyelitis, influenza, burn wounds, IV drug use, postpartum gynecologic infections, fasciitis, septic abortion
Diagnostic Criteria (all four required)
- Fever ≥38.9°C
- Hypotension (systolic BP ≤90 mmHg)
- Diffuse macular erythroderma (rash)
- Involvement of ≥3 organ systems (renal, hepatic, hematologic, GI, muscular, CNS)
Clinical Features
| Feature | Details |
|---|---|
| Onset | Acute - fever, sore throat, myalgias |
| Rash | Diffuse blanching macular erythroderma, begins on trunk, spreads to extremities, involves palms/soles |
| Desquamation | Full-thickness, appears 1-2 weeks after onset, especially hands and feet |
| Mucous membranes | Strawberry tongue, conjunctivitis, vaginitis (non-exudative) |
| GI symptoms | Diarrhea, vomiting common |
| Outcome | Multiorgan failure if untreated |
Host Susceptibility
Patients lacking neutralizing antibodies against TSST-1 are at significantly increased risk. This explains why most adults have some level of protection (acquired through subclinical colonization), while menstruating women who fail to mount an antibody response are disproportionately affected.
TSST-1 vs. Other Superantigen Toxins
| Feature | TSST-1 | SEB / SEC |
|---|---|---|
| TSS type | Menstrual (100%) + nonmenstrual | Nonmenstrual (~50%) |
| Mucosal crossing | Yes (unique) | No |
| Heat stability | Relatively stable | SEB heat stable |
| Encoded on | Chromosomal pathogenicity island | Pathogenicity island |
Other staphylococcal superantigens include 15 enterotoxins (A-E, G-P) and the exfoliative toxins A and B (which cause staphylococcal scalded skin syndrome by a different mechanism involving desmoglein cleavage rather than cytokine storm).
Treatment
- Aggressive IV fluid resuscitation (mainstay - corrects the vasodilatory shock)
- Remove the source (remove tampon, drain abscess, debride wound)
- Antibiotics targeting S. aureus and S. pyogenes, including MRSA coverage:
- Vancomycin or linezolid (MRSA)
- Clindamycin is particularly useful as it suppresses toxin synthesis (protein synthesis inhibitor)
- Alternatives: imipenem, meropenem, piperacillin-tazobactam
- Ventilatory support and pressors as needed for organ failure
- IVIG has been used to provide neutralizing antibodies in refractory cases
Sources: Jawetz Melnick & Adelberg's Medical Microbiology 28e | Goldman-Cecil Medicine | Janeway's Immunobiology 10e | Fitzpatrick's Dermatology | Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.