Stages of clubbing
Reading File
Finding Sources
Finding Sources
Searching Images
stages of finger clubbing grades
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Searching the Web
stages grades of finger clubbing Schamroth sign classification
Finding Sources
Finding Sources
Loading Image
Here is a comprehensive overview of the stages (grades) of digital clubbing, synthesized from multiple authoritative sources.
Digital Clubbing — Stages & Classification
Clubbing is graded using the Curth classification (most widely used), progressing through 4 grades based on the degree of nail-bed changes, Lovibond angle alteration, and soft-tissue changes.
Key Anatomical Reference Points
Before discussing stages, two landmarks matter:
- Lovibond angle (hyponychial angle): The angle between the nail plate and the proximal nail fold when viewed in profile. Normal ≈ 160°. Obliteration (≥180°) is the hallmark of clubbing.
- Schamroth sign: When dorsal surfaces of the opposing terminal phalanges of corresponding fingers are placed together, a normal diamond-shaped ("window") gap appears at the base of the nail beds. In clubbing, this window is lost.
Grades of Clubbing (Curth/Wynder Classification)
| Grade | Features |
|---|---|
| Grade 1 (Softening) | Fluctuation and softening of the nail bed; periungual erythema. The nail can be "rocked" on its bed. No change in Lovibond angle yet. |
| Grade 2 (Obliteration of angle) | Lovibond angle obliterated — becomes ≥180°. Schamroth sign positive (loss of diamond window). Nail appears flat or slightly elevated at its base. |
| Grade 3 (Rounding) | Nail curves downward in both longitudinal and transverse planes ("watch-glass" or "parrot-beak" appearance). Distal phalanx begins to enlarge. Periungual skin looks shiny. |
| Grade 4 (Drumstick) | Marked bulbous enlargement of the entire distal phalanx — classic "drumstick" or "Hippocratic finger" appearance. The distal segment is warm and may be erythematous. In severe cases: hypertrophic osteoarthropathy (HOA) with periosteal new bone on long bones. |
Some texts use a 5-grade scale that splits Grade 3 into finger-tip enlargement and nail-bed thickening as separate steps, but the 4-grade schema above is standard in most internal medicine and respiratory medicine textbooks.
Full-Blown Clubbing — Four Cardinal Signs
All major textbooks (Murray & Nadel, Fishman's, Harrison's) agree on these features when clubbing is established:
- Lovibond angle obliterated (most sensitive sign — normally 165°, becomes ≥180°)
- Nail bed softening and sponginess — the nail "floats" on a spongy bed; periungual erythema
- Nail curvature — increased convexity in both longitudinal and transverse planes
- Bulbous enlargement of the distal phalanx — warm, erythematous terminal digit
Clinical Notes
- Onset: Can develop rapidly (~2 weeks) in empyema, and similarly reverse after corrective cardiac surgery. — Murray & Nadel's Textbook of Respiratory Medicine
- COPD does NOT cause clubbing — its presence in a COPD patient should prompt a search for lung cancer. — Fishman's Pulmonary Diseases and Disorders
- HOA (hypertrophic osteoarthropathy) can accompany advanced clubbing, especially with bronchogenic carcinoma — periosteal new bone on radius, ulna, tibia, fibula with pain and swelling.
- Unilateral clubbing may suggest Takayasu arteritis, ipsilateral sulcus tumor, or median nerve injury.
- Pathogenesis: Vasodilation of fingertip vessels → increased hydrostatic pressure → interstitial edema of soft tissue. VEGF, PDGF, HIF-1α, and HIF-2α are all elevated in clubbed digits, with increased microvessel density. — Murray & Nadel's
Clinical Photo — Advanced Clubbing

Advanced clubbing (Grade 4): Bulbous "drumstick" enlargement of distal phalanges bilaterally with loss of Lovibond angle.
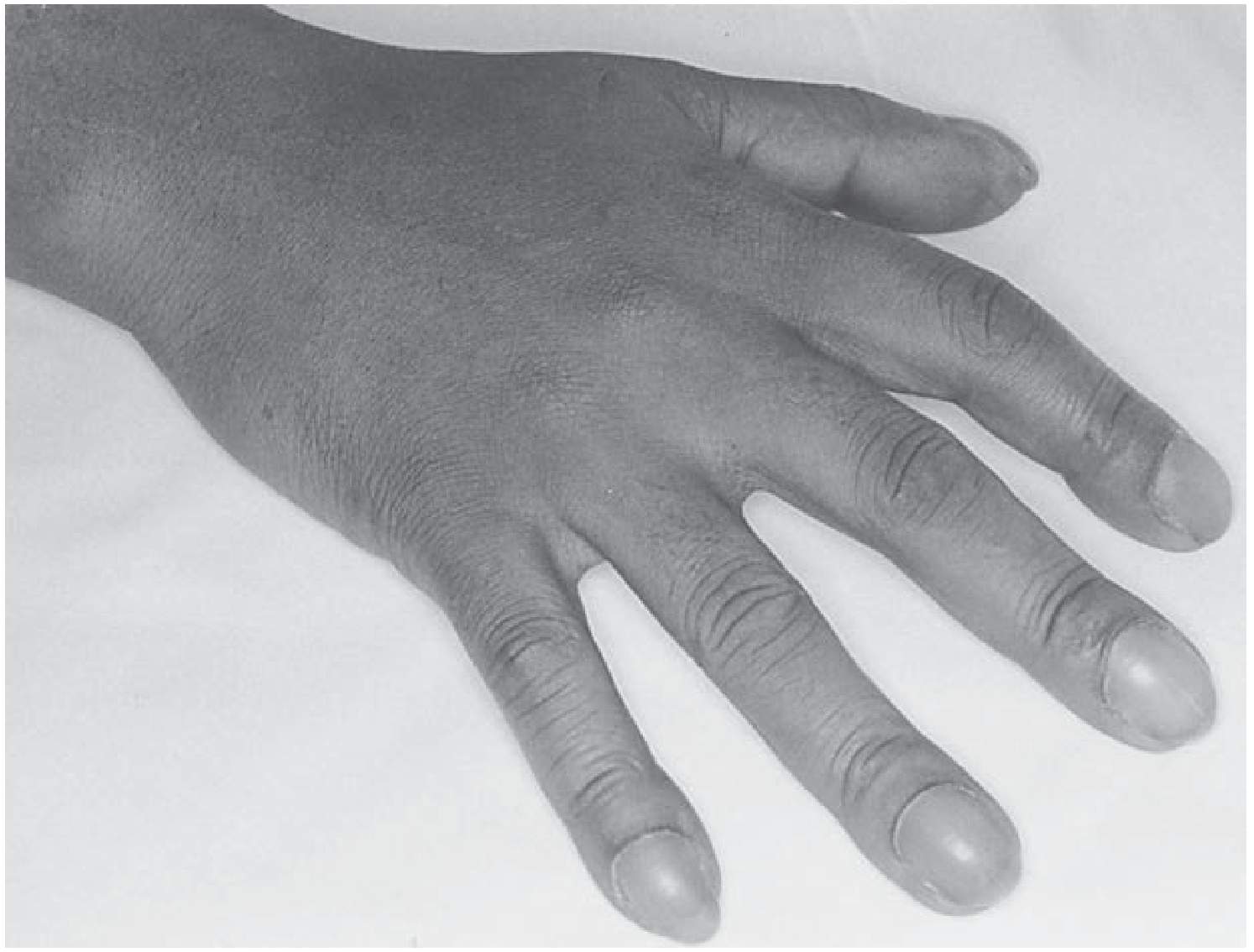
Clubbing of all fingers in a case of primary lung adenocarcinoma (from Fishman's Pulmonary Diseases and Disorders).
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Andrews' Diseases of the Skin; Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.