Lung
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of lung anatomy and physiology, drawn from Murray & Nadel's Textbook of Respiratory Medicine.
Lung - Anatomy & Physiology
1. Essential Functions
The lung has two core, interdependent functions:
- Ventilation-perfusion matching - delivering O2 to tissues and removing CO2
- Host defense - protecting against airborne pathogens, chemicals, and particulates
Secondary functions include surfactant synthesis and recycling, mucociliary clearance, neuroendocrine signaling, and secretion of diverse molecules by epithelial and endothelial cells. - Murray & Nadel's, p. 32
2. Gross Organization
- The lungs weigh 900-1000 g in life, of which nearly 40-50% is blood.
- At end-expiration (FRC), gas volume is about 2.5 L; at maximal inspiration (TLC) it reaches 6 L.
- Lung density ranges from 0.30 g/mL at FRC to 0.14 g/mL at TLC, and is not uniform - ~1 g/mL near the hilum, ~0.1 g/mL peripherally.
- Over 50% of all alveoli sit in the outer 30% of lung radius (hilum to chest wall).
- Blood vessels are more distended in the lower lung fields due to increasing vascular distending pressure (~1 cm H2O per cm height descending the lung). - Murray & Nadel's, p. 33
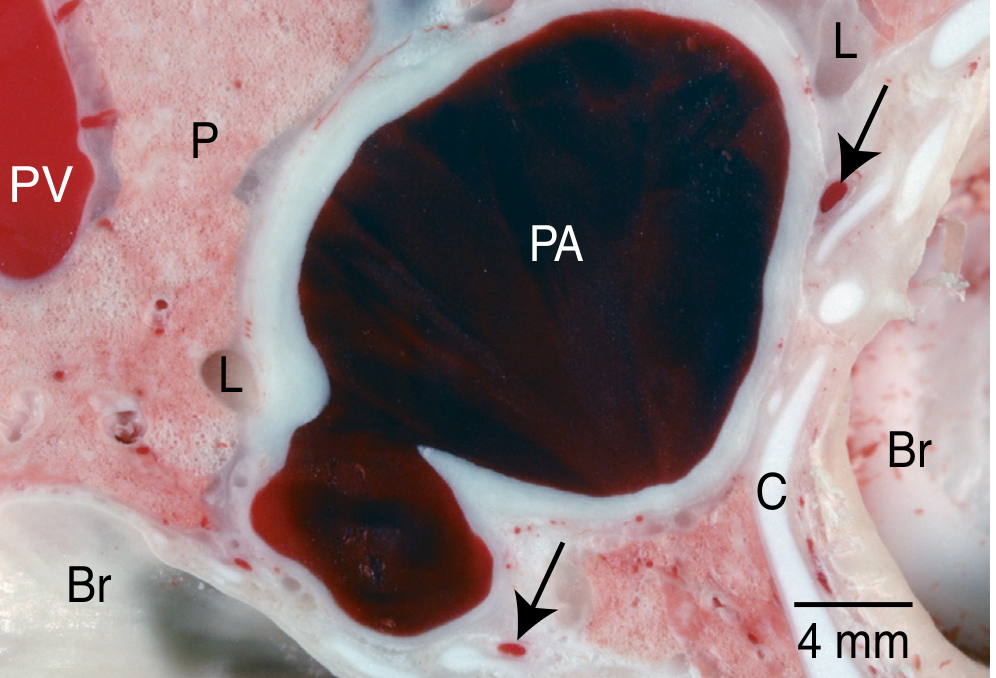
Figure: Frozen sheep lung showing oxygenation levels - PA blood is dark purple (deoxygenated), PV blood is crimson (oxygenated). Gas exchange occurs across lung parenchyma (P).
3. Airways
The airway tree conducts gas from the trachea down to the terminal respiratory units (TRUs). Key structural levels:
| Level | Structure | Feature |
|---|---|---|
| Conducting zone | Trachea → bronchi → bronchioles | Cartilage present down to bronchi; mucociliary clearance |
| Transitional | Respiratory bronchioles | Both conduct and participate in gas exchange |
| Gas exchange zone | Alveolar ducts + alveoli | Ultra-thin walls for diffusion |
The bronchial circulation supplies the conducting airways; the pulmonary circulation handles gas exchange. - Murray & Nadel's, Ch. 1
4. Terminal Respiratory Unit (TRU) / Acinus
The TRU is the fundamental gas-exchange unit, consisting of a respiratory bronchiole plus all accompanying alveolar ducts and alveoli.
- Each TRU contains ~100 alveolar ducts and ~2000 alveoli
- At FRC: ~5 mm diameter, volume ~0.02 mL per unit
- There are approximately 150,000 TRUs in the adult human lung
Gas-phase diffusion is so fast within the TRU that O2 and CO2 partial pressures are uniform throughout the unit. The TRU size is defined by the fact that gas molecules equilibrate within the unit faster than they cross the air-blood barrier into blood. - Murray & Nadel's, p. 265
Air-blood barrier structure (thin side, inside-out):
Type I epithelium → fused basal laminae (interstitium) → capillary endothelium → plasma → red blood cell cytoplasm
The thin side is kept extremely thin because O2 diffusion through water is the rate-limiting step in gas exchange. - Murray & Nadel's, p. 262
Key diffusion fact: CO2 is 20x more soluble in water than O2. Even though its driving pressure is only 1/10th that of O2, CO2 still diffuses rapidly into the gas phase.
5. Pleural Space
- The pleural space is a real space, not a potential space.
- Normal pleural liquid volume: 0.1-0.2 mL/kg body weight.
- Surface area: ~1000 cm2/lung; pleural space width: 10-20 µm.
- Mesothelial microvilli are only 3-5 µm long, so there is normally little direct contact between parietal and visceral pleura.
- Lymphatic stomata (1-12 µm diameter) in the parietal pleura drain the pleural space; they are located over intercostal spaces in the distal thorax and along the sternum. - Murray & Nadel's, p. 43
6. Lung Volumes & Respiratory Mechanics
| Volume/Capacity | Definition | How Measured |
|---|---|---|
| Tidal Volume (VT) | Volume of one normal breath | Spirometry |
| Vital Capacity (VC) | Max volume exhaled after max inhalation | Spirometry |
| Total Lung Capacity (TLC) | Volume at end of maximal inspiration | Plethysmography or helium dilution |
| Residual Volume (RV) | Volume after maximal expiration | Plethysmography or helium dilution |
| FRC | Volume at end of normal tidal exhalation (respiratory muscles relaxed) | Plethysmography or helium dilution |
FRC is the equilibrium point where elastic inward recoil of the lungs exactly balances elastic outward recoil of the chest wall.
Key mechanics concepts:
- Compliance - volume change per unit pressure; reflects lung and chest wall stiffness
- Resistance - pressure required per unit flow; dominated by airway caliber
- Work of breathing - energy cost of moving gas; increased in obstructive (high resistance) and restrictive (low compliance) disease
- At a constant flow, gas velocity is greater in narrower tubes (why turbulence develops at bifurcations). - Murray & Nadel's, p. 253
7. Ventilation-Perfusion (V/Q) Matching
Most clinical hypoxemia is due to V/Q inequality, not diffusion limitation. In normal lungs:
- Perfusion increases apex-to-base (gravity effect)
- Ventilation also increases apex-to-base, but less steeply
- The apex has a higher V/Q ratio; the base has a lower V/Q ratio
- Diffusion limitation only occurs in healthy people during heavy exercise at altitude (where RBC transit time is shortened). - Murray & Nadel's, p. 275
Summary Table
| Feature | Value |
|---|---|
| Lung weight | 900-1000 g |
| Gas volume at FRC | ~2.5 L |
| Gas volume at TLC | ~6 L |
| Number of alveoli | ~500 million |
| Number of TRUs | ~150,000 |
| Alveoli per TRU | ~2000 |
| Normal pleural fluid | 0.1-0.2 mL/kg |
| Air-blood barrier (thin side) | <0.5 µm |
Source: Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume (ISBN 9780323655873), Chapter 1 - Anatomy, and Chapter 11 - Respiratory System Mechanics and Energetics.
Lung Anatomy hilum openings
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Excellent - both hilum diagrams retrieved. Here is the full answer:
Lung Hilum - Anatomy & Structures
What is the Hilum?
The hilum (plural: hila) is the wedge-shaped depression on the mediastinal (inner) surface of each lung, where structures enter and leave the organ. It is enclosed in a sleeve of mediastinal pleura that reflects onto the lung surface as visceral pleura - the region outlined by this pleural reflection is the hilum.
The collective bundle of structures at the hilum is called the root of the lung - a short tubular assembly that attaches the lung to the mediastinum. - Gray's Anatomy for Students, p. 204
Structures Passing Through the Hilum
Six categories of structures enter/exit at each hilum:
| Structure | Notes |
|---|---|
| Pulmonary artery (×1) | Carries deoxygenated blood from the right ventricle |
| Pulmonary veins (×2) | Carry oxygenated blood back to the left atrium; located inferior and anterior |
| Main bronchus (×1) | Carries air; lies posteriorly in the hilum |
| Bronchial vessels | Systemic vessels that nourish the bronchial wall and lung parenchyma |
| Lymphatics | Drain via hilar lymph nodes into mediastinal nodes |
| Autonomic nerves | Sympathetic and parasympathetic fibers forming the pulmonary plexus |
Abundant lymph nodes and loose connective tissue surround all these tubular structures. - Fischer's Mastery of Surgery, p. 2213
General Positional Arrangement (Anterior → Posterior)
From front to back at each hilum:
- Anterior pulmonary plexus (nerves)
- Pulmonary vessels - artery superior, two veins inferior
- Bronchi and bronchial vessels (most posterior)
- Posterior pulmonary plexus (nerves)
Generally: pulmonary artery is superior, pulmonary veins are inferior and anterior, bronchus is posterior. - Scott-Brown's Otorhinolaryngology, p. 939
Right vs. Left Hilum - Key Differences
Right Hilum
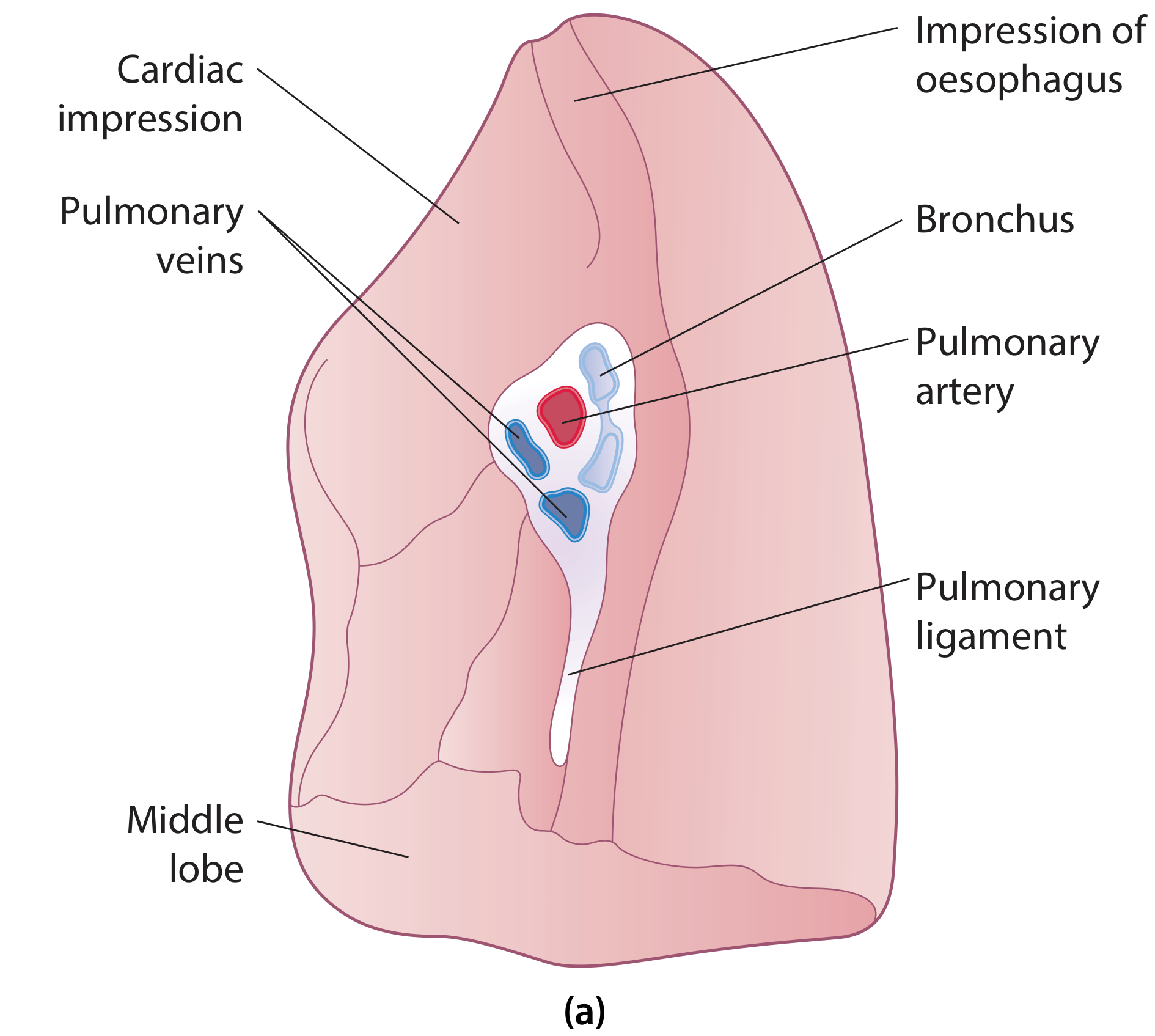
- Pulmonary veins are the most anterior structures; their course is predominantly inferomedial
- Pulmonary artery is intermediately placed; course is predominantly transverse
- Bronchus is the most posterior; course is superolateral
- The right upper lobe bronchus branches from the main bronchus within the root itself (above the pulmonary artery) - this is unique to the right side
- The azygos vein crosses cephalad to the hilum (superior relation)
- Phrenic nerve and pericardiophrenic artery pass anterior to the root in a different tissue plane (important surgically)
- Vagus nerve passes posterior to the hilum; the esophagus is posterior/inferior
Left Hilum
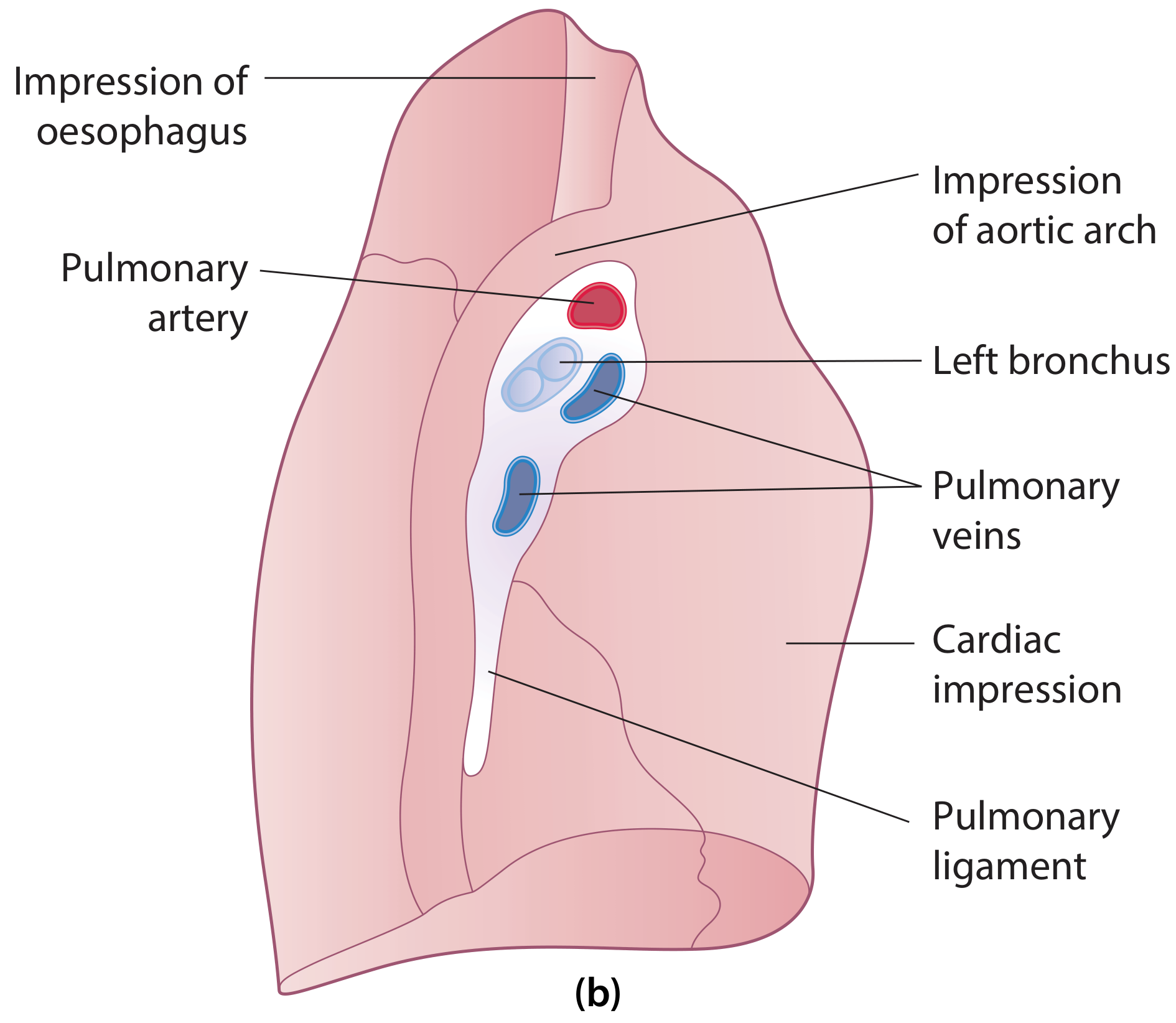
- Pulmonary artery is superior to the bronchus and pulmonary vein; it initially runs anteriorly then curves over the bronchus before dividing
- Pulmonary veins are anterior and inferior (same as right)
- Bronchus is posterior (same pattern)
- The left upper lobe bronchus branches within the lung itself, not in the root (unlike the right)
- Aortic arch is the superior relation (vs. azygos on the right)
- Descending aorta and left vagus nerve cross posteriorly to the left hilum
- Phrenic nerve passes anterior to the left hilum
Summary: Right vs. Left Hilum at a Glance
| Feature | Right Hilum | Left Hilum |
|---|---|---|
| Superior relation | Azygos vein | Aortic arch |
| Posterior relation | Right vagus + esophagus | Descending aorta + left vagus |
| Anterior relation | Superior vena cava | Phrenic nerve |
| Upper lobe bronchus | Branches in the root (above PA) | Branches within the lung |
| Pulmonary artery position | Intermediate (transverse) | Superior (curves over bronchus) |
Pulmonary Ligament
Inferior to the hilum, a blade-like fold of pleura hangs down as the pulmonary ligament. It extends from the hilum to the mediastinum, stabilizes the position of the inferior lobe, and accommodates the movement of hilar structures during breathing. - Gray's Anatomy for Students, p. 204; Scott-Brown's Otorhinolaryngology, p. 939
Sources: Gray's Anatomy for Students (9780323934237), Scott-Brown's Otorhinolaryngology (9781138094642), Fischer's Mastery of Surgery (9781975176433)
This is a shared conversation. Sign in to Orris to start your own chat.