Angiofibroma
Reading File
Finding Sources
Searching PubMed
angiofibroma
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Angiofibroma, covering the two main clinically important types: Juvenile Nasopharyngeal Angiofibroma (JNA) and Cutaneous Angiofibroma.
Angiofibroma
I. Juvenile Nasopharyngeal Angiofibroma (JNA / JA)
Definition & Nature
Juvenile angiofibroma (JA) is a benign but locally aggressive tumor histologically characterized by vascular endothelium-lined spaces embedded in a fibrous stroma. It occurs almost exclusively in adolescent males. Immunohistochemical and electron microscopy studies suggest it is more accurately a vascular malformation (hamartoma) than a true neoplasm. - Cummings Otolaryngology Head and Neck Surgery
Pathogenesis / Origin
- Postulated to arise from incomplete regression of the first branchial arch artery, which transiently connects the ventral and dorsal aortas during embryogenesis (days 22-24).
- The lesion's blood supply from the maxillary and sphenopalatine arteries, with persistent ICA connections, supports this theory.
- Molecular studies show upregulation of VEGFA (angiogenesis) and FGFR pathway involvement.
- CTNNB1 mutations (encoding β-catenin) are present in the majority of sporadic cases.
- In familial adenomatous polyposis (FAP), JA can arise from germline APC gene mutations (both lead to β-catenin activation). - Robbins Pathologic Basis of Disease
Site of Origin
The pathognomonic epicenter is the pterygopalatine fossa - specifically near the sphenopalatine foramen, the base of the pterygoid process, or the superior portion of the choana.
Patterns of Spread
JA grows through foramina and fissures of the skull base:
- Medially - through the sphenopalatine foramen into the nasopharynx and nasal cavity
- Laterally - through the pterygomaxillary fissure into the infratemporal fossa
- Anteriorly - pushes the posterior wall of the maxillary sinus forward
- Superiorly - into the sphenoid sinus through the sphenoid floor
- Intracranially - via the orbit or direct skull base erosion (advanced cases)
Bone involvement occurs by two mechanisms: pressure resorption (subperiosteal growth) or cancellous bone invasion at the root of the pterygoid process.
Clinical Features
| Symptom | Comment |
|---|---|
| Unilateral nasal obstruction | Most common presenting complaint |
| Epistaxis (recurrent, severe) | Most common presenting complaint |
| Cheek swelling | Infratemporal fossa involvement |
| Proptosis / diplopia | Orbital involvement |
| Headache | Cranial fossa involvement |
- Classic presentation: smooth, hypervascularized mass behind the middle turbinate in a teenage boy
- Biopsy is rarely justified due to high hemorrhage risk.
Imaging Diagnosis
Diagnosis is based on CT + MRI:
- Origin invariably at the pterygopalatine fossa with erosion of the medial pterygoid plate base
- Hypervascular enhancement after contrast
- Characteristic pattern of spread
- On MRI: signal voids on T1 and T2 (representing major intralesional vessels) - pathognomonic
Differentiation from lobular capillary hemangioma, hemangiopericytoma, and schwannoma may be needed - these do NOT involve the pterygopalatine fossa and occur in different age groups.
Blood Supply
- Primary supply: External carotid artery (internal maxillary artery and ascending pharyngeal artery)
- Advanced lesions: also receive supply from the internal carotid artery (found in ~35.6%) and bilateral supply (~30.8%)
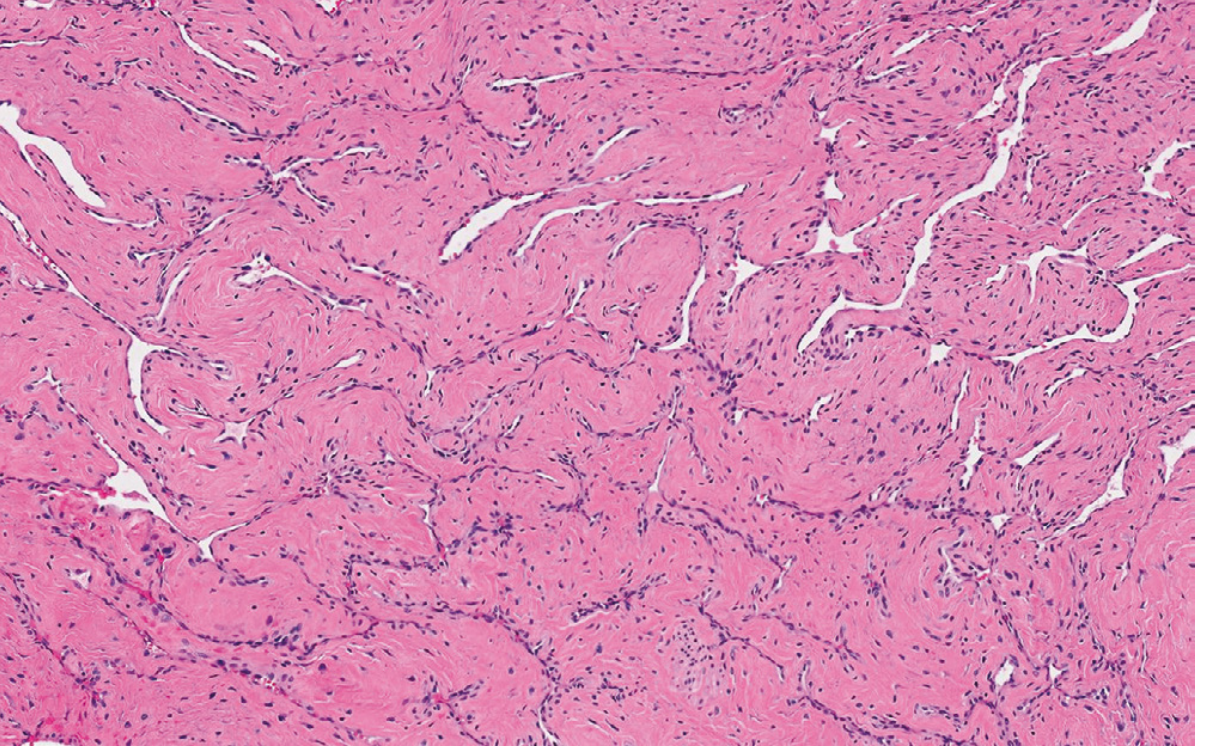
Histopathology
The tumor consists of numerous thin-walled vessels lined by a single layer of endothelial cells, embedded in a dense collagenous stroma containing small, bland fibroblasts. The vessels lack a well-developed smooth muscle layer and cannot contract when cut - explaining the severe, uncontrolled epistaxis.
Management
Preoperative embolization (performed 48 hours before surgery) is now standard practice. It dramatically reduces intraoperative bleeding, allows more accurate dissection of tumor borders, and maps the vascular supply (ICA connections, vertebral artery, contralateral carotid branches). Superselective embolization is performed using polyvinyl alcohol particles via intra-arterial digital subtraction angiography.
Surgery (endoscopic or open depending on extent) is the treatment of choice. - Cummings Otolaryngology; Robbins Pathologic Basis of Disease
- Recurrence rates approach 20%
- 9% of cases can be fatal (in historically reported series)
- Residual disease can involute spontaneously on MRI follow-up (especially in adolescents)
Radiotherapy is reserved for unresectable intracranial extension.
II. Cutaneous Angiofibroma
Cutaneous angiofibroma is a descriptive term for a group of lesions with different clinical presentations but similar histology. - Dermatology 2-Volume Set 5e
Clinical Variants
| Type | Features |
|---|---|
| Fibrous papule | Solitary, dome-shaped, shiny, skin-colored to reddish papule on the nose/face of adults. Can mimic intradermal nevus, BCC, or adnexal tumor. White color on dermoscopy. |
| Pearly penile papules | Pearly white, dome-shaped, closely aggregated papules on the corona of the glans penis. Found in up to 30% of postpubertal men (more common in uncircumcised). Often mistaken for condylomata acuminata. |
| Multiple facial angiofibromas | Associated with tuberous sclerosis (TS), MEN1, Birt-Hogg-Dube syndrome, and rarely NF2. Bilateral, on cheeks, nasolabial folds, nose, chin - sparing perioral skin in TS. |
| Ungual fibroma (Koenen tumor) | Periungual fibromas seen in tuberous sclerosis |
Associations (Multiple Facial Angiofibromas)
- Tuberous sclerosis (TS): Facial angiofibromas (≥3) and ungual angiofibromas (≥2) are major diagnostic criteria for TS
- Multiple Endocrine Neoplasia type 1 (MEN1)
- Birt-Hogg-Dube syndrome
- Rarely neurofibromatosis type 2
Histopathology
All angiofibromas share: dome-shaped lesions with a dermal proliferation of plump or stellate fibroblasts in a collagenous stroma, with an increase in thin-walled, dilated blood vessels. Collagen fibers may arrange concentrically around hair follicles and vessels (perifollicular fibroma variant). Elastic fibers are decreased; some fibroblasts may be multinucleated.
Treatment of Facial Angiofibromas in Tuberous Sclerosis
A 2024 systematic review on laser treatment (PMID 38728593) confirms laser therapy as an effective modality for facial angiofibromas in TS. Topical sirolimus (mTOR inhibitor) is also established as a treatment - a 2024 systematic review (PMID 39018447) confirms its efficacy in dermatologic angiofibromas. This is significant because TS is caused by mutations in TSC1/TSC2 genes, leading to mTOR pathway overactivation - making topical sirolimus a pathogenesis-directed treatment.
Summary Comparison
| Feature | Juvenile Nasopharyngeal Angiofibroma | Cutaneous Angiofibroma |
|---|---|---|
| Who | Adolescent males | Adults (varies by type) |
| Location | Pterygopalatine fossa / nasopharynx | Face, penis, periungual |
| Behavior | Locally aggressive, no metastases | Benign, no aggressive behavior |
| Key symptoms | Epistaxis, nasal obstruction | Cosmetic; diagnose associations |
| Genetics | CTNNB1/APC mutations | TSC1/TSC2 (in TS context) |
| Treatment | Embolization + surgery | Laser, topical sirolimus |
| Key associations | FAP (APC mutations) | Tuberous sclerosis, MEN1, BHD |
Sources: Cummings Otolaryngology Head and Neck Surgery; Robbins, Cotran & Kumar Pathologic Basis of Disease; Dermatology 2-Volume Set 5e; Bailey and Love's Short Practice of Surgery 28th Ed
This is a shared conversation. Sign in to Orris to start your own chat.