Inverted papilloma
Reading File
Finding Sources
Searching PubMed
"inverted papilloma" sinonasal
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information to provide a detailed answer on inverted papilloma. Let me compile everything.
Inverted Papilloma (Sinonasal)
Overview
Inverted papilloma (IP) is the second most common benign tumor of the sinonasal tract after osteoma, and the most common form of sinonasal papilloma. It accounts for 0.4%-4.7% of all surgically removed nasal tumors, with an incidence of 0.74-2.3 new cases per 100,000 per year. Men are affected 2-3 times more than women, with peak incidence in the 5th and 6th decades of life.
- Cummings Otolaryngology Head and Neck Surgery, p. 986
Histopathology
The defining feature is epithelium inverting into the stroma rather than growing outward. Key histologic features:
- Hyperplastic ribbons of basement membrane-enclosed epithelium growing downward into the underlying stroma
- Multilayered epithelium composed of squamous or ciliated columnar cells
- Mixed with mucocytes and transmigrating neutrophils
- Distinct and intact basement membrane throughout
- Occasional association with sinonasal hamartomas
This inward (inverted) growth pattern distinguishes IP from exophytic and oncocytic papillomas.
Site of Origin
| Site | Frequency |
|---|---|
| Ethmoid region | 48% |
| Lateral nasal wall / maxillary sinus | 28% |
| Frontal sinus | 2.5% |
| Bilateral frontal involvement | ~16% |
The maxillary medial wall (especially near the fontanelles) is the single most common origin site. Frontal and sphenoid sinuses are rarely the primary site. Bilateral papillomas are exceptional.
Etiology
Established risk factors:
- Organic solvent exposure - significantly associated with IP with a dose-response relationship
- Smoking - not linked to IP development but is a strong risk factor for recurrence and malignant transformation (12-fold higher risk of malignant transformation in smokers vs. non-smokers, P <0.001)
HPV role (controversial):
- HPV DNA detected in ~13-22% of cases (low-risk types 6 & 11 most common; high-risk types 16, 18, 45 less common)
- Transcriptionally active HPV was NOT detected in a study of 52 IPs including those with malignant transformation, suggesting most carcinomatous transformation is driven by non-HPV mechanisms
- A 2025 meta-analysis (PMID 39739414) further examined HPV infection and recurrence - the role remains controversial
Molecular basis:
- IP harbors activating EGFR mutations, preserved even in malignant transformation
- Oncocytic papillomas carry KRAS mutations (never found in IP) - this distinction helps confirm they are separate entities
Clinical Features
Symptoms:
- Unilateral nasal obstruction (most common)
- Watery rhinorrhea
- Unilateral rhinosinusitis (headache, facial pain from obstruction)
- Epiphora, proptosis, diplopia - seen with orbital involvement (should raise suspicion of malignant transformation)
Endoscopic appearance:

Imaging
CT: Primary mode of imaging; identifies extent of disease, bony erosion, and focal hyperostosis (a useful marker for site of origin).
MRI (preferred for complete assessment):
- Better differentiation between tumor and inflammatory mucosa
- Demonstrates the pathognomonic cerebriform-columnar pattern - alternating parallel folds of highly cellular metaplastic epithelium and less cellular stroma - highly predictive of IP

MRI is especially useful in frontal sinus disease to distinguish mucus from tumor. Bony spur/focal hyperostosis on imaging helps pinpoint the site of origin.
Biopsy under endoscopic guidance is always indicated to establish definitive histology.
Malignant Transformation
- Occurs in 5-15% of cases
- Synchronous occurrence (coexisting carcinoma at time of diagnosis) is more frequent than metachronous
- Vast majority are squamous cell carcinomas (SCC)
- Rare associated tumors: sinonasal undifferentiated carcinoma, mucoepidermoid carcinoma, verrucous carcinoma

Risk factors for malignant transformation:
- Smoking (12x higher risk)
- High-risk HPV (debated)
- Dysplasia on histology
Management
Surgical Principles
Surgery is the definitive treatment. The key principles are:
- Identify the precise site of origin
- Dissect involved mucosa in the subperiosteal plane
- Drill the underlying bone at the attachment site
- Achieve complete excision - residual disease is the primary cause of recurrence
Approach
Endoscopic (preferred) - recommended whenever feasible, with lower morbidity than open approaches.
Contraindications to exclusive endoscopic approach:
- Concomitant malignancy involving critical structures
- Site of origin on the anterior wall or lateral recess of the frontal sinus, or massive frontal sinus mucosal involvement
- Orbital involvement
Contemporary trend - pedicle-oriented resection:
Rather than complete demucosalization of the entire sinus, this approach focuses resection on the specific site of tumor attachment, offering equivalent recurrence rates with shorter operative times and fewer complications.
Frontal Sinus IP - Surgical Strategy
| Site of origin | Recommended approach |
|---|---|
| Medial wall or lower anterior/posterior wall | Draf IIa/b or MELP |
| Superior anterior/posterior wall or lateral wall | OPF, or MELP with external trephine |
| Lateral to midpoint of orbit | OPF, MELP with external trephine |
Frontal sinus IP has higher recurrence rates (22%) than IP at other sinonasal sites managed endoscopically (~3%), reflecting the anatomical challenges of the frontal recess.
(MELP = modified endoscopic Lothrop procedure; OPF = osteoplastic flap)
Recurrence
- Recurrence is the defining clinical challenge - most often due to residual disease rather than true biological recurrence
- Rates vary by site and surgical technique
- Regular postoperative endoscopic surveillance is mandatory
Key Summary Points
| Feature | Detail |
|---|---|
| Incidence | 0.4-4.7% of nasal tumors |
| Sex/age | M:F = 2-3:1; 5th-6th decade |
| Most common site | Lateral nasal wall / maxillary sinus |
| Histology | Endophytic epithelial growth, intact BM |
| Key mutation | EGFR activating mutation |
| Imaging hallmark | Cerebriform-columnar pattern on MRI |
| Malignant transformation | 5-15% (mainly SCC) |
| Treatment | Complete surgical excision + bone drilling |
| Recurrence risk | Mainly from residual disease |
Recent literature note: A 2025 meta-analysis (PMID 39739414) specifically examined HPV infection and IP recurrence, supporting the ongoing debate about HPV's role. Machine learning for IP identification was reviewed in a 2025 systematic review (PMID 40933895), reflecting interest in AI-assisted diagnosis of this lesion.
Sources: Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1
Make a short note on middle ear mucosal fold
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a comprehensive short note. Here it is:
Middle Ear Mucosal Folds
Introduction
The mucous membrane lining the tympanic cavity extends beyond the bony walls to cover the ossicles, their supporting ligaments, tendons of the two middle ear muscles, and associated neurovascular structures - much like the peritoneum drapes over the abdominal viscera. In doing so, it forms a series of mucosal folds (which may thicken to become ligaments) that divide the middle ear into distinct compartments with important physiological and surgical implications.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2
Compartments Created by Mucosal Folds
The folds divide the tympanic cavity into three broad levels:
| Compartment | Location |
|---|---|
| Epitympanum (attic) | Above the level of the malleolar folds |
| Mesotympanum | Middle region; visible through EAC with microscope |
| Hypotympanum | Below the inferior tympanic sulcus; continuous with mesotympanum |
The epitympanum is further divided into anterior and posterior components by the bony cog.
Named Mucosal Folds (Proctor's Classification)
The folds are classically described by Proctor and arise mainly from the ossicular chain:
| Fold | Origin / Location |
|---|---|
| Lateral malleolar fold | Lateral to malleus neck; bounds Prussak's space superiorly |
| Anterior malleolar fold | Part of the epitympanic diaphragm; contributes to separation of attic from mesotympanum |
| Superior malleolar fold | Over the head of malleus |
| Tensor fold | Formed by the tensor tympani tendon/mucosal covering; anterior component of epitympanic diaphragm |
| Lateral malleoincudal fold | Posterior component of epitympanic diaphragm |
| Interosseous fold (17) | Between malleus and incus |
| Medial incudal fold (9) | Medial to incus |
| Superior incudal fold (11) | Over body of incus |
| Plica stapedi (8) | Around the stapes |
| Obturatoria stapedi (5) | At the stapes footplate |
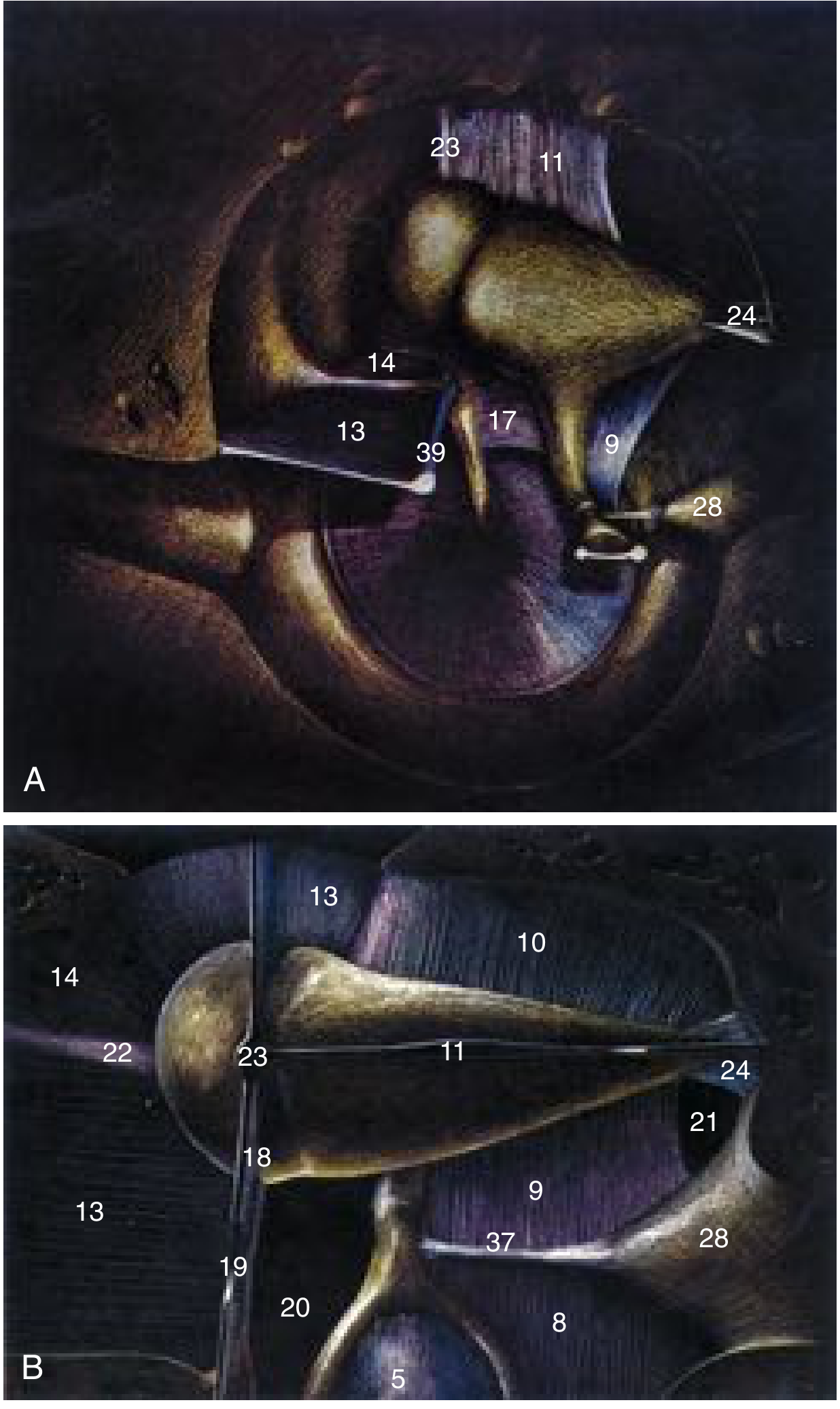
Proctor's illustration of middle ear mucosal folds (Cummings): Tensor fold (13), interosseous fold (17), medial incudal fold (9) separate epitympanum from mesotympanum. The isthmus tympani anticus (20) and posticus (21) are the only remaining ventilation openings.
The Epitympanic Diaphragm
The epitympanic diaphragm is formed by two key structures:
- Lateral malleoincudal fold - posteriorly
- Tensor fold - anteriorly
Together they separate the epitympanum from the mesotympanum, leaving only two small openings as the conduits for air ventilation into the attic:
Tympanic Isthmus
- Isthmus tympani anticus (anterior isthmus) - anterior opening
- Isthmus tympani posticus (posterior isthmus) - posterior opening
These are the only routes for ventilation of the epitympanic space from the Eustachian tube via the mesotympanum.
Prussak's Space
- Located between the pars flaccida and the neck of the malleus
- Bounded superiorly by the lateral malleolar fold
- Important because it is a site of keratin retention and the primary origin of pars flaccida cholesteatoma
Clinical Significance
1. Middle Ear Aeration
The mesotympanum is ventilated freely by the Eustachian tube at all times. The epitympanum, however, depends entirely on airflow through the narrow isthmus tympani. This makes it selectively vulnerable to ventilation failure.
2. Cholesteatoma Pathogenesis
- Blockage of the isthmus by:
- Congenital fold defects
- Mucosal disease (chronic otitis media)
- Cholesteatoma itself
- Inflammatory processes
- Results in negative pressure in the epitympanum → retraction of pars flaccida → Prussak's space involvement → acquired cholesteatoma
3. Surgical Relevance
- Mucosal folds create multiple recesses and pockets (sinus tympani, facial recess, supratubal recess) that can harbor occult cholesteatoma
- Knowledge of fold anatomy is essential for complete cholesteatoma clearance and safe ossicular surgery
- The chorda tympani nerve courses between the malleus and incus through the fold system
Summary
The middle ear mucosal folds are thin mucosal reflections that cover the ossicles, tendons, and neurovascular structures within the tympanic cavity. Their primary roles are:
- Compartmentalize the middle ear (epitympanum vs. mesotympanum)
- Create the epitympanic diaphragm, restricting attic ventilation to the isthmus tympani
- Form Prussak's space, the key site of pars flaccida cholesteatoma development
Any disruption to fold integrity - whether inflammatory, congenital, or iatrogenic - can compromise epitympanic ventilation and predispose to cholesteatoma formation.
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2; Cummings Otolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.