Treatment algorithm of hypertension as per jnc
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
JNC 8 hypertension treatment algorithm flowchart
Finding Sources
Reading File
Finding Sources
I now have comprehensive information to provide a thorough answer. Let me compile the JNC hypertension treatment algorithm.
JNC 8 Hypertension Treatment Algorithm
Blood Pressure Classification (JNC 7 framework, still widely used)
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Normal | < 120 | < 80 |
| Prehypertension | 120–139 | 80–89 |
| Stage 1 HTN | 140–159 | 90–99 |
| Stage 2 HTN | ≥ 160 | ≥ 100 |
Step 1 — Lifestyle Modifications (All Patients)
Initiate in all hypertensive patients and those with prehypertension:
- Weight reduction (target BMI < 25 kg/m²) → ↓ SBP ~5–20 mmHg per 10 kg lost
- DASH diet (low saturated fat, low sodium) → ↓ SBP ~8–14 mmHg
- Sodium restriction (< 2.4 g/day) → ↓ SBP ~2–8 mmHg
- Regular aerobic exercise (30 min/day, most days) → ↓ SBP ~4–9 mmHg
- Alcohol limitation (≤ 2 drinks/day men, ≤ 1 drink/day women)
- Smoking cessation
Step 2 — Treatment Thresholds (JNC 8)
| Patient Group | Initiate Drug Therapy At | Target BP |
|---|---|---|
| Age ≥ 60 years (general) | SBP ≥ 150 or DBP ≥ 90 | < 150/90 mmHg |
| Age < 60 years | SBP ≥ 140 or DBP ≥ 90 | < 140/90 mmHg |
| Any age + CKD | SBP ≥ 140 or DBP ≥ 90 | < 140/90 mmHg |
| Any age + Diabetes | SBP ≥ 140 or DBP ≥ 90 | < 140/90 mmHg |
Step 3 — Initial Drug Selection
Non-African American Patients (including those with diabetes)
Choose one of:
- Thiazide-type diuretic (e.g., chlorthalidone, HCTZ)
- Calcium Channel Blocker (CCB)
- ACE Inhibitor (ACEI)
- Angiotensin Receptor Blocker (ARB)
African American Patients (including those with diabetes)
Choose one of:
- Thiazide-type diuretic or CCB
- (ACEI/ARB are less effective as monotherapy in this group)
Patients with CKD (all races)
- ACEI or ARB is mandatory (first-line or add-on), regardless of race or diabetes status
- Improves renal outcomes independent of BP lowering
Step 4 — Titration Algorithm
Start one drug (or two if BP is >20/10 mmHg above target)
↓
Reassess within 1 month
↓
Goal not reached?
├── Increase dose of initial drug
└── OR add a second drug from a different class
↓
Still not at goal?
└── Add third drug from remaining classes
↓
Goal still not reached?
└── Refer to hypertension specialist
Use other classes: aldosterone antagonists, α-blockers,
central agents, direct vasodilators
- If BP is > 20/10 mmHg above target at presentation → start with two drugs simultaneously (combination pill preferred)
- Most patients (~75%) will need ≥ 2 drugs
Compelling Indications — Preferred Drug Classes
| Co-morbidity | Preferred Agent(s) |
|---|---|
| Heart failure (HFrEF) | ACEI/ARB + Beta-blocker + Diuretic + Aldosterone antagonist |
| Post-MI | ACEI/ARB + Beta-blocker |
| Coronary artery disease | ACEI + Beta-blocker |
| Diabetes mellitus | ACEI or ARB (especially if microalbuminuria) |
| CKD / Proteinuria | ACEI or ARB |
| Previous stroke | ACEI + Thiazide diuretic |
| LV hypertrophy | ACEI, ARB, or CCB |
| Pregnancy | Alpha-methyldopa, Hydralazine (avoid ACEI, ARB, diuretics) |
| Peripheral vascular disease | CCB or vasodilators (avoid beta-blockers) |
| Hypercholesterolemia | ACEI, CCB, alpha-blockers |
| Asthma/COPD | Avoid beta-blockers |
Important Combinations to Avoid
- ACEI + ARB (dual RAS blockade) — almost always contraindicated
- ARB + Renin inhibitor (e.g., aliskiren) — contraindicated
- Beta-blocker — not first-line in most patients with uncomplicated HTN (inferior stroke prevention vs. other classes)
- ACEI — avoid in pregnancy (teratogenic)
Resistant Hypertension
Defined as BP remaining above goal despite ≥ 3 drugs (including a diuretic) at optimal doses.
Management:
- Ensure medication adherence and correct technique
- Rule out secondary causes (renal artery stenosis, primary aldosteronism, pheochromocytoma, sleep apnea)
- Add spironolactone (aldosterone antagonist) 12.5–50 mg/day — has strong evidence
- Consider referral to hypertension specialist
Key Clinical Pearls:
- Chlorthalidone is preferred over HCTZ (longer-acting, more potent)
- CCBs are often under-used; peripheral edema can be mitigated by combining with a low-dose ACEI
- ACEI/ARB are safe in CKD with mild-moderate renal insufficiency; an increase in creatinine of up to 30–40% is acceptable if it stabilizes
- Monitor for hyperkalemia when using ACEI/ARB, especially in CKD
— Swanson's Family Medicine Review, p. 136–137; Textbook of Family Medicine 9e, p. 653–654; Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1411–1413
Make answers based on harrison
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
I have all the content from Harrison's 22nd edition. Now I'll compile the comprehensive answer.
Hypertension Treatment Algorithm — Harrison's Principles of Internal Medicine (22nd Ed.)
BP Classification (ACC/AHA, used in Harrison's 22e)
| Category | SBP (mmHg) | DBP (mmHg) |
|---|---|---|
| Normal | < 120 | < 80 |
| Elevated BP | 120–129 | < 80 |
| Stage 1 Hypertension | 130–139 | 80–89 |
| Stage 2 Hypertension | ≥ 140 | ≥ 90 |
Overall Treatment Algorithm (Fig. 288-3)
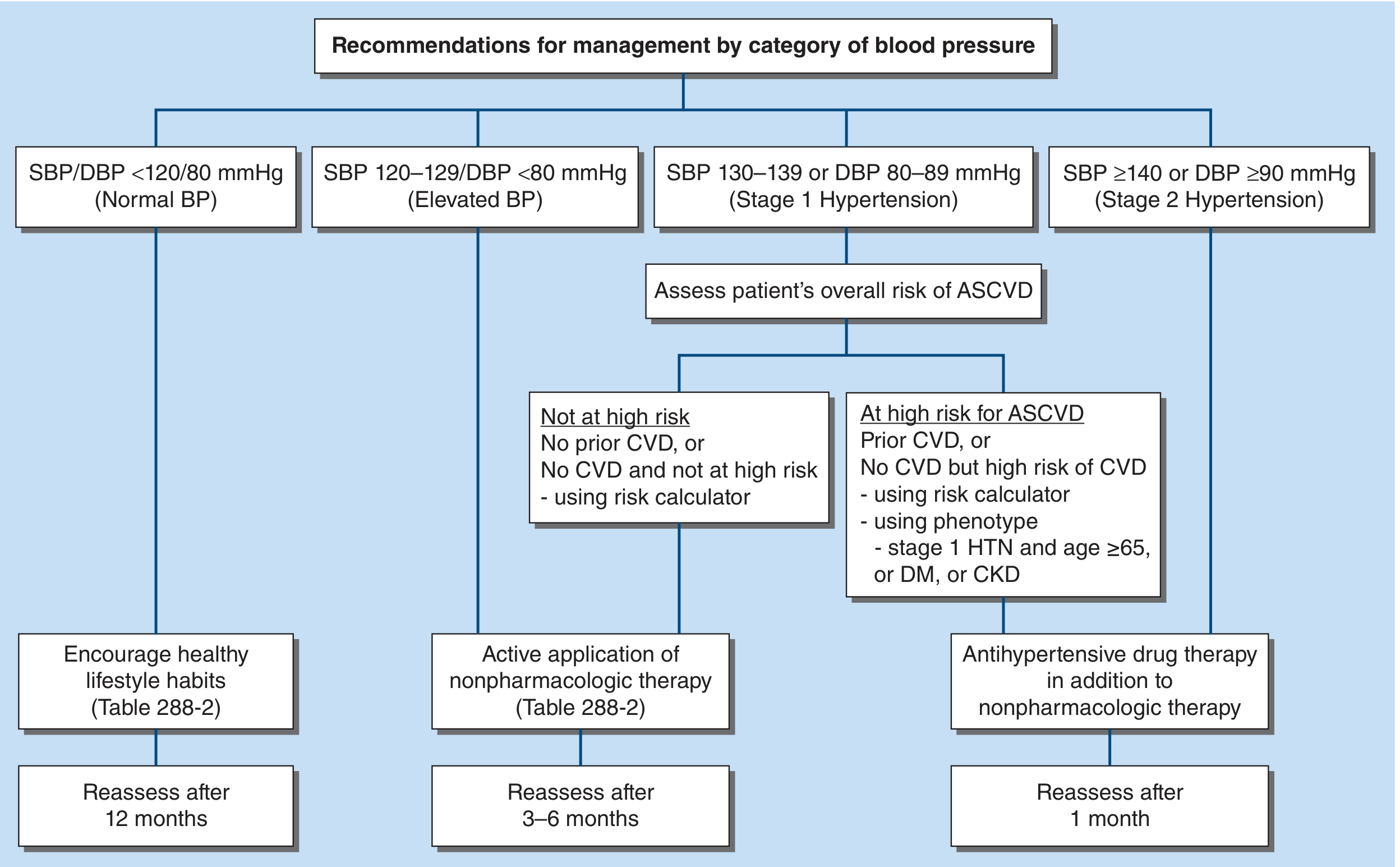
Step-by-Step Management by BP Category
Normal BP (SBP/DBP < 120/80 mmHg)
- Encourage healthy lifestyle habits
- Reassess after 12 months
Elevated BP (SBP 120–129, DBP < 80 mmHg)
- Active nonpharmacologic therapy only
- Reassess after 3–6 months
Stage 1 HTN (SBP 130–139 or DBP 80–89 mmHg)
Assess 10-year ASCVD risk:
| Risk Status | Management |
|---|---|
| Not at high risk (no CVD, 10-yr ASCVD < 10%) | Nonpharmacologic therapy alone × 6 months; add drug if goal not reached |
| At high risk (prior CVD, or ASCVD ≥ 10%, or age ≥ 65, or DM, or CKD) | Drug therapy + nonpharmacologic therapy |
- Reassess after 1 month
Stage 2 HTN (SBP ≥ 140 or DBP ≥ 90 mmHg)
- Always start antihypertensive drug therapy + nonpharmacologic therapy
- Most patients require ≥ 2 drugs — especially non-Hispanic Black adults and all with SBP ≥ 140 mmHg
- Reassess after 1 month
Nonpharmacologic Interventions (Table 288-2)
Harrison's endorses these six evidence-based interventions:
| Intervention | Expected SBP Reduction |
|---|---|
| Weight loss (obese/overweight) | ~5 mmHg per 5 kg lost |
| Heart-healthy diet (DASH) | ~8–11 mmHg |
| Sodium restriction (< 1.5 g/day ideal) | ~5–6 mmHg |
| Increased physical activity | ~4–5 mmHg |
| Alcohol limitation | ~3–4 mmHg |
| Potassium supplementation (diet/pills) | ~4–5 mmHg |
Greater BP reduction is expected when interventions are combined and in patients who already have hypertension. Nonpharmacologic interventions also enhance the effect of antihypertensive medications.
Drug Therapy — First-Step Classes (Fig. 288-4)
Harrison's recommends four first-step drug classes for patients without a compelling indication for beta-blockers:
| Class | Preferred Examples | Key Notes |
|---|---|---|
| Thiazide/thiazide-like diuretics | Chlorthalidone 12.5–25 mg OD, Indapamide 1 mg OD | Chlorthalidone preferred over HCTZ — longer half-life, better nighttime BP control, used in landmark U.S. trials |
| ACE Inhibitors | Lisinopril 10–40 mg, Enalapril 5–40 mg, Ramipril 2.5–20 mg | OD; do NOT combine with ARB; contraindicated in pregnancy |
| ARBs | Losartan, Valsartan, Azilsartan, Candesartan, Olmesartan | Side effects rare; do NOT combine with ACEI; contraindicated in pregnancy |
| CCB (dihydropyridine) | Amlodipine 2.5–10 mg, Felodipine, Nifedipine LA | Primarily vasoactive; peripheral edema ~10% (dose-dependent); amlodipine preferred |
Beta-blockers are classified as "Other Drugs" — not first-line for uncomplicated HTN. In head-to-head RCTs, beta-blockers are inferior to the other four classes, especially for stroke prevention. Use only when there is a compelling indication (HF, post-MI, CAD, arrhythmia).
Evidence Hierarchy Among First-Step Classes
- Meta-analyses identify diuretics as "best in class" for first-step CVD prevention overall
- CCBs are better for stroke prevention but inferior for HF prevention vs. diuretics
- ACEI/ARBs are equivalent and interchangeable; do not use in combination
BP Treatment Targets
| Population | Target |
|---|---|
| Most adults with HTN | SBP/DBP < 130/80 mmHg |
| Community-dwelling adults ≥ 65 years | SBP < 130 mmHg |
| Older adults with high comorbidity burden / limited life expectancy | Clinical judgment + patient preference |
Resistant Hypertension
Definition: SBP/DBP above goal despite ≥ 3 drugs (including a diuretic) at optimal doses, OR requiring ≥ 4 drugs to achieve control.
Management approach:
1. Exclude pseudo-resistance (inaccurate measurement)
2. Obtain out-of-office BP → exclude white coat HTN
3. Assess lifestyle adherence and medication nonadherence
4. Switch to long-acting diuretics (chlorthalidone or indapamide — replace HCTZ)
5. Convert multiple pills → single pill combination
6. Add Mineralocorticoid Receptor Antagonist (MRA):
- Spironolactone (first choice, low cost)
- Eplerenone or Finerenone (if gynecomastia/side effects)
7. If true resistant HTN with office SBP ≥ 160 mmHg:
→ Consider renal denervation (FDA-approved 2023)
Special Populations
| Group | Preferred Approach |
|---|---|
| Diabetes mellitus | ACEI or ARB (especially with microalbuminuria/proteinuria) |
| CKD with proteinuria | ACEI or ARB mandatory |
| Heart failure (HFrEF) | ACEI/ARB + beta-blocker + diuretic + MRA (compelling indication for beta-blocker) |
| Post-MI / CAD | ACEI + beta-blocker |
| Non-Hispanic Black adults | Diuretic or CCB preferred as initial monotherapy (ACEI/ARB less effective as monotherapy in this group); most will require ≥ 2 drugs |
| Pregnancy | Avoid ACEI and ARB (teratogenic); safe options: methyldopa, labetalol, nifedipine |
| Elderly (frail, comorbid) | Individualize; avoid overtreatment; shared decision-making |
| Non-DHP CCB (diltiazem, verapamil) | Rarely used for HTN alone; avoid in HFrEF; caution with bradycardia/heart block |
Improving Hypertension Control
Harrison's emphasizes that traditional one-on-one care is insufficient. Evidence-based strategies include:
- Team-based care (nurses, pharmacists, community health workers with prescribing authority) — average ↓ SBP ~7 mmHg, up to 23 mmHg in optimized models
- Home BP monitoring (HBPM) to complement office measurements
- Single-pill combinations to improve adherence
- Electronic support systems and lifestyle counseling programs
— Harrison's Principles of Internal Medicine, 22nd Edition, Chapter 288: Prevention and Treatment of Primary Hypertension, pp. 2184–2192
This is a shared conversation. Sign in to Orris to start your own chat.