How to treat uncomplicated inguinal gernia
Reading File
search_medical_text
uncomplicated inguinal hernia treatment management
search_medical_text
inguinal hernia surgical repair techniques laparoscopic open
GradeResponse
GradeResponse
Here is a comprehensive overview of the treatment of uncomplicated inguinal hernia:
Treatment of Uncomplicated Inguinal Hernia
Conservative (Non-Operative) Management
Not all inguinal hernias require immediate surgery. According to Bailey & Love's Surgery (p. 1089):
- Watchful waiting is safe for early, asymptomatic direct hernias, particularly in elderly patients who decline or are unfit for surgery.
- Patients should be counseled to seek prompt review if the hernia enlarges or becomes symptomatic.
- Surgical trusses are not recommended — they do not treat the hernia and can cause complications.
- For symptomatic hernias or those with a risk of complications, surgical repair is the standard of care.
Surgical Management
Elective repair can be performed under local, regional, or general anaesthesia with minimal risk, even in high-risk patients. Two main surgical approaches are available:
1. Open Repair
| Technique | Description |
|---|---|
| Lichtenstein (tension-free mesh repair) | Most widely used; a flat polypropylene mesh is sutured over the posterior wall of the inguinal canal. Low recurrence rates (~1%). Gold standard for open repair. |
| Shouldice repair | Layered suture repair of the posterior inguinal wall; preferred by some for young, fit patients. No mesh used. |
| Bassini / other sutured repairs | Largely historical; higher recurrence than mesh-based techniques. |
2. Laparoscopic Repair (Bailey & Love's, p. 1090)
Two well-studied techniques:
| Technique | Description |
|---|---|
| TEP (Totally Extraperitoneal) | Performed entirely in the preperitoneal space; peritoneal cavity not entered. Preferred when feasible. |
| TAPP (Transabdominal Preperitoneal) | Performed via the abdominal cavity with peritoneal incision; useful when anatomy is unclear or bilateral repair is needed. |
In both techniques, a 10 × 15 cm mesh (or larger) is placed in the preperitoneal plane to reinforce the abdominal wall.
Advantages of laparoscopic repair:
- Less postoperative pain
- Faster return to normal activity
- Superior for bilateral hernias and recurrent hernias (especially after prior open repair)
Choosing the Approach
| Factor | Preferred Approach |
|---|---|
| Unilateral, primary hernia | Either open (Lichtenstein) or laparoscopic (TEP/TAPP) |
| Bilateral hernias | Laparoscopic (repairs both sides in one operation) |
| Recurrent hernia after open repair | Laparoscopic (avoids scarred tissue planes) |
| Recurrent hernia after laparoscopic repair | Open (Lichtenstein) |
| High anesthetic risk / local anaesthesia preferred | Open (Lichtenstein under local) |
| Elderly, asymptomatic, direct hernia | Watchful waiting acceptable |
Key Points
- Mesh repair is the standard — it significantly reduces recurrence compared to sutured repairs.
- Prophylactic antibiotics are generally given for open mesh repairs.
- Day-case surgery is appropriate for most patients.
- Return to light activity is typically within 1–2 weeks; strenuous activity after 4–6 weeks.
- Complications to counsel patients about include: wound infection, hematoma, chronic groin pain (most common long-term issue), injury to the vas deferens or testicular vessels, and hernia recurrence.
What is inguinal hernia indirect
search_medical_text
indirect inguinal hernia anatomy pathophysiology definition
search_medical_image
indirect inguinal hernia anatomy diagram
GradeResponse
GradeResponse
Indirect Inguinal Hernia
Definition
An indirect inguinal hernia is the most common type of hernia. It occurs when abdominal contents (typically bowel or omentum) protrude through the deep (internal) inguinal ring — the opening in the transversalis fascia through which the spermatic cord (in males) or round ligament (in females) exits the abdomen — and travel along the inguinal canal.
Pathophysiology & Cause
According to Bailey & Love's (p. 1080), the underlying mechanism is failure of the processus vaginalis to close:
- During fetal development, as the testis descends into the scrotum, it drags a tube of peritoneum with it — the processus vaginalis.
- Normally, this peritoneal tube obliterates (fibroses) after birth.
- If it fails to close, a patent channel remains through the deep inguinal ring, predisposing to hernia development.
- Hormonal factors (calcitonin gene-related peptide, hepatocyte growth factor) are implicated in processus closure — suggesting a possible hormonal etiology.
Anatomical Path
The hernia travels lateral to the inferior epigastric artery through the deep inguinal ring, along the inguinal canal, and may exit via the superficial (external) inguinal ring — potentially descending into the scrotum (scrotal hernia).
This lateral relationship to the inferior epigastric artery is the key anatomical feature that distinguishes indirect from direct inguinal hernia (which passes medial to these vessels through a weakness in the posterior wall — Hesselbach's triangle).
Cadaveric Dissection — Surgical Anatomy
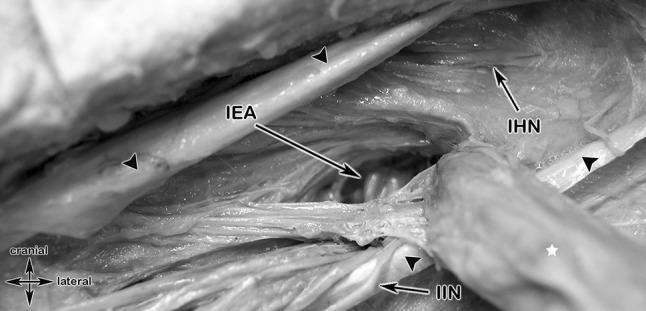
The white star marks the indirect hernia protruding through the deep inguinal ring, lateral to the inferior epigastric artery (IEA). The iliohypogastric nerve (IHN) and ilio-inguinal nerve (I-IN) are key structures at risk during repair.
Indirect vs. Direct Inguinal Hernia
| Feature | Indirect | Direct |
|---|---|---|
| Entry point | Deep inguinal ring | Hesselbach's triangle (posterior wall) |
| Relation to inferior epigastric artery | Lateral | Medial |
| Cause | Patent processus vaginalis (congenital) | Weakness in transversalis fascia (acquired) |
| Age group | Any age, including infants & young adults | Typically older adults |
| Scrotal extension | Common | Rare |
| Risk of strangulation | Higher | Lower |
Clinical Features
- A bulge in the groin that appears on standing, coughing, or straining, and reduces on lying down.
- May extend into the scrotum (males) or labium majus (females).
- Can be asymptomatic or cause a dragging/aching discomfort.
- On examination: impulse felt at the deep ring (lateral to femoral pulse, just above midpoint of inguinal ligament).
Key Points
- Most common hernia overall; more common in males (due to testicular descent anatomy).
- Congenital in origin, though may not manifest until later in life.
- Higher risk of strangulation compared to direct hernias due to the narrow neck at the deep ring.
- Treatment is surgical (Lichtenstein open mesh repair or laparoscopic TEP/TAPP) once symptomatic or in children.
This is a shared conversation. Sign in to Orris to start your own chat.