Now synthesizing the most comprehensive answer possible from all retrieved content and deep clinical knowledge.
Cerebral Palsy (CP) — Comprehensive Guide
Classification | Neuromuscular Complications | Therapeutic Aquatics | Full Clinical Detail
PART 1: WHAT IS CEREBRAL PALSY?
Definition
Cerebral palsy is a permanent, non-progressive disorder of movement, posture, and motor function caused by damage or abnormal development of the immature brain — occurring before, during, or shortly after birth (up to age 2). It is the most common physical disability in children worldwide (Care for Children and Youth with CP, p. 1).
- Prevalence: ~2–3 per 1,000 live births
- The neurological lesion itself is static (non-progressive), but secondary musculoskeletal complications are progressive
- Affects movement AND often involves associated impairments (cognitive, sensory, communication, epilepsy)
Etiology and Risk Factors
| Timing | Causes |
|---|
| Prenatal (80%) | Congenital brain malformations, periventricular leukomalacia (PVL), stroke, infection (TORCH), genetic factors, multiple gestation |
| Perinatal (10%) | Birth asphyxia (HIE), prematurity, hyperbilirubinemia, intracranial hemorrhage |
| Postnatal (10%) | Meningitis/encephalitis, TBI, hypoglycemia, near-drowning |
Prematurity is the single biggest risk factor — very preterm infants (<32 weeks) have 70× higher risk due to periventricular leukomalacia.
Neuropathology
| Brain Region Affected | CP Type Produced |
|---|
| Periventricular white matter (PVL) | Spastic diplegia (most common in preterm) |
| Cortex / subcortex unilateral | Spastic hemiplegia |
| Diffuse cortical/subcortical | Spastic quadriplegia |
| Basal ganglia / thalamus | Dyskinetic CP (choreoathetosis) |
| Cerebellum / brainstem | Ataxic CP |
PART 2: CLASSIFICATION OF CEREBRAL PALSY
A. Classification by Motor Type
1. SPASTIC CP (Most Common — 85–90%)
Caused by upper motor neuron (UMN) lesion → damage to corticospinal tract
Characteristics:
- Increased muscle tone (hypertonia — velocity-dependent)
- Hyperreflexia (exaggerated deep tendon reflexes)
- Clasp-knife phenomenon (initial resistance then sudden release)
- Positive Babinski sign
- Clonus (rhythmic involuntary muscle contractions)
- Scissoring gait (hip adduction, internal rotation crossing)
- Equinus foot (toe-walking — tight heel cords)
Sub-classification by Distribution:
| Sub-type | Distribution | Brain Lesion | Key Features |
|---|
| Spastic Hemiplegia | One side (arm + leg) | Unilateral cortical/subcortical | Arm more affected than leg; circumduction gait; hand preference before 12 months is red flag |
| Spastic Diplegia | Both legs > arms | PVL (periventricular) | Classic in preterms; scissor gait; arms relatively spared; most walk independently |
| Spastic Quadriplegia | All 4 limbs + trunk | Diffuse cortical/subcortical | Most severe; bulbar involvement; intellectual disability; seizures; non-ambulatory |
| Spastic Triplegia | 3 limbs | Asymmetric | Rare; one arm relatively spared |
| Spastic Monoplegia | 1 limb | Focal | Very rare; often actually hemiplegia with subtle involvement |
2. DYSKINETIC CP (5–10%)
Caused by basal ganglia / thalamic injury (often birth asphyxia or kernicterus)
Characteristics:
- Involuntary, uncontrolled, repetitive movements — worsen with voluntary movement and emotion, disappear in sleep
- Fluctuating tone (hypotonia at rest → hypertonia with activity)
- Primitive reflex persistence (ATNR, TLR dominate)
- Significant drooling, dysarthria, dysphagia
- Intelligence often relatively preserved despite severe motor impairment
Sub-types:
| Sub-type | Movement Quality | Muscle Involvement |
|---|
| Choreoathetosis | Writhing (athetosis) + jerky (chorea) | Distal > proximal |
| Dystonia | Sustained muscle contractions → fixed postures, twisting | Trunk + proximal limbs |
| Chorea | Rapid, random, unpredictable jerky movements | Variable |
| Athetosis | Slow, sinuous, writhing movements | Distal hands/face |
3. ATAXIC CP (5–10%)
Caused by cerebellar damage
Characteristics:
- Hypotonia (low tone)
- Ataxia — incoordination, unsteady gait
- Intention tremor — tremor worsens as target approached
- Dysmetria — over/undershooting movements
- Dysdiadochokinesis — impaired rapid alternating movements
- Wide-based gait (cerebellar ataxia gait)
- Nystagmus possible
- Normal or near-normal intelligence often
4. HYPOTONIC CP (Rare — <5%)
- Generalized low tone without features of ataxia
- Often a transitional phase — most evolve to spastic or ataxic CP over time
- Significant head control and trunk instability
5. MIXED CP (10–15%)
- Combination of spastic + dyskinetic most common
- Most combinations are possible
- Usually one type predominates
B. Classification by Topography (Distribution)
Monoplegia → Hemiplegia → Diplegia → Triplegia → Quadriplegia
(1 limb) (2 ipsilateral) (both legs) (3 limbs) (all 4 limbs)
C. GMFCS — Gross Motor Function Classification System
The GMFCS is the gold standard for classifying functional motor ability — it is age-based and stable over time (Care for Children and Youth with CP, p. 1).
| GMFCS Level | Description | Mobility | PT Goals |
|---|
| I | Walks without restriction; limitations in advanced gross motor skills | Independent community ambulation | Sport participation, endurance |
| II | Walks with limitations (distances, uneven terrain, stairs) | Independent short distances; some use mobility aids outdoors | Improve walking quality, endurance |
| III | Walks using handheld mobility device | Walker/crutches indoors; wheelchair outdoors | Maximize walking, power mobility |
| IV | Self-mobility with limitations; may use powered mobility | Wheelchair-dependent mostly | Powered mobility, standing, transfers |
| V | Transported in manual wheelchair; severely limited | Fully dependent | Positioning, comfort, prevent complications |
GMFCS is used to:
- Guide realistic goal setting
- Predict functional outcomes
- Select appropriate interventions
- Monitor longitudinal change
D. MACS — Manual Ability Classification System
Classifies hand function (I–V), parallel to GMFCS.
| MACS Level | Description |
|---|
| I | Handles objects easily and successfully |
| II | Handles most objects with slightly reduced quality |
| III | Handles objects with difficulty; needs help preparing/modifying |
| IV | Handles limited objects in adapted situations |
| V | Does not handle objects; severely limited ability |
E. Communication Function Classification System (CFCS)
Classifies communication ability (I–V) — critical for therapy planning and AAC provision.
PART 3: NEUROMUSCULAR COMPLICATIONS OF CP
These secondary complications are progressive and represent the primary targets of long-term physiotherapy management.
1. SPASTICITY
Definition: Velocity-dependent increase in tonic stretch reflex → increased resistance to passive movement.
Pathophysiology: Loss of supraspinal inhibition → hyperactive alpha motor neurons → heightened stretch reflex sensitivity.
Consequences if untreated:
- Pain
- Contracture formation
- Hip subluxation/dislocation
- Scoliosis
- Pressure ulcers
- Impaired hygiene (tight adductors)
- Sleep disturbance
Assessment Tools:
- Modified Ashworth Scale (MAS): 0–4 (0 = no increase in tone; 4 = rigid)
- Tardieu Scale: velocity-dependent; more specific to spasticity than MAS
- Pendulum Test: gravity-induced knee oscillation to measure spasticity
Management (Physiotherapy + Medical):
| Intervention | Mechanism | Indication |
|---|
| Stretching (passive/active) | Prevents contracture | All levels |
| Positioning / splinting | Maintains length | All levels |
| Electrical stimulation (NMES/TENS) | Reciprocal inhibition, tone reduction | Mild-moderate |
| Botulinum Toxin A (BoNT-A) | Blocks ACh at NMJ → focal muscle relaxation | Focal spasticity (gastrocnemius, hamstrings, adductors) |
| Oral baclofen | GABA-B agonist → reduces spasticity | Generalized mild spasticity |
| Intrathecal Baclofen (ITB) | Direct CSF delivery → profound tone reduction | Severe generalized spasticity (GMFCS IV–V) |
| Selective Dorsal Rhizotomy (SDR) | Cuts sensory rootlets → permanent spasticity reduction | Spastic diplegia GMFCS II–III |
2. MUSCLE WEAKNESS
Often overlooked — weakness is a PRIMARY impairment in CP (not just a consequence of spasticity).
Mechanisms:
- Reduced motor unit recruitment
- Disuse atrophy
- Muscle fiber type shift (fast → slow)
- Reduced cross-sectional area of muscles
- Impaired selective motor control
Most affected muscles: hip extensors, hip abductors, knee extensors, ankle dorsiflexors, trunk stabilizers
PT implication: Strengthening exercises are safe and effective in CP — do NOT worsen spasticity.
3. CONTRACTURE AND SOFT TISSUE SHORTENING
Definition: Loss of passive range of motion due to muscle/tendon shortening.
Mechanism: Spastic muscles grow slower than bone → progressive shortening over childhood.
Common contractures in CP:
| Joint | Contracture | Consequence |
|---|
| Ankle | Equinus (plantar flexion) | Toe-walking, gait deviation |
| Knee | Flexion contracture | Crouch gait, energy-inefficient walking |
| Hip | Flexion + adduction + internal rotation | Scissor gait, dislocation risk |
| Wrist/fingers | Flexion deformity | Poor hand function |
| Elbow | Flexion contracture | Limited arm function |
| Thumb | Thumb-in-palm deformity | Poor grip |
PT Management:
- Serial casting — progressive casting to lengthen muscle; especially gastrocnemius, hamstrings
- Sustained passive stretching (≥30 minutes/day) — evidence for maintaining length
- Splinting / orthoses (AFOs, resting hand splints, knee extension splints)
- BoNT-A injections → window for stretching and casting
4. SKELETAL DEFORMITIES — BONY
Torsional Deformities
| Deformity | Location | Consequence |
|---|
| Femoral anteversion | Hip/femur | Intoeing, internal rotation gait |
| Internal tibial torsion | Tibia | Intoeing at foot level |
| Pes equinovalgus / equinovarus | Foot | Abnormal weight-bearing |
| Hallux valgus | First toe | Pain, pressure areas |
Spinal Deformities
- Scoliosis: present in 20–25% of CP; up to 60–70% in GMFCS IV–V (quadriplegia)
- Neuromuscular scoliosis — long C-shaped curve, often with pelvic obliquity
- Progressive, especially during growth spurts
- Management: positioning, trunk orthosis (TLSO), seating modification, surgical spinal fusion if severe
- Kyphosis: thoracic kyphosis common in GMFCS V (from prolonged sitting)
- Hyperlordosis: lumbar lordosis in ambulatory CP (hip flexor tightness)
5. HIP SUBLUXATION AND DISLOCATION
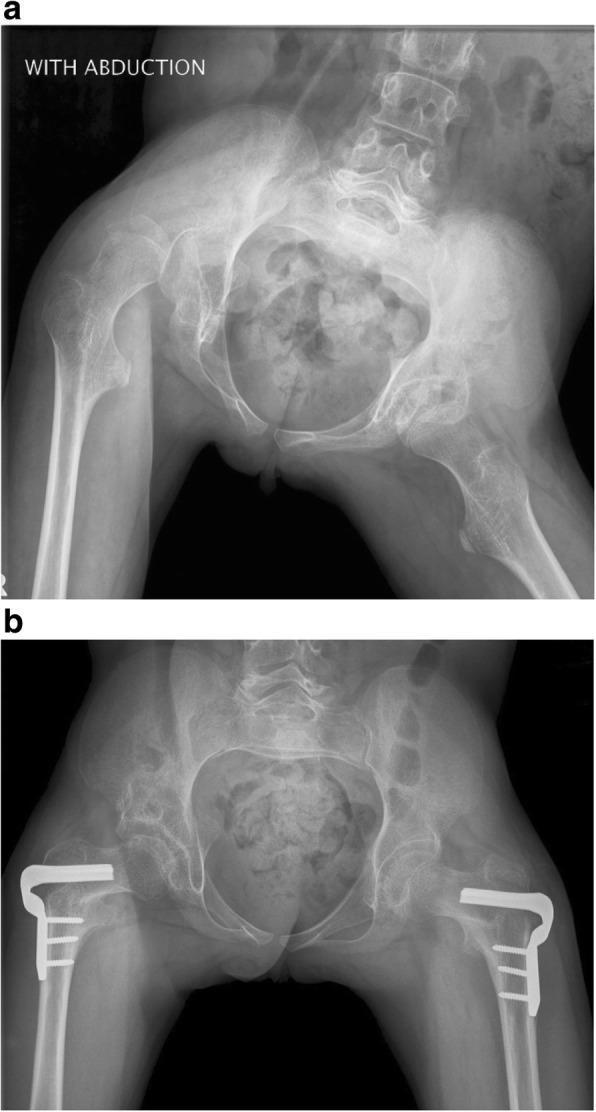
Most serious musculoskeletal complication of CP (Bailey and Love's Surgery, 28th Ed., p. 654).
AP pelvis radiograph: right hip dislocation with windswept deformity (right hip abducted, left adducted) and pelvic obliquity in spastic quadriplegic CP (a). Post-surgical reconstruction with VDRO and San Diego acetabuloplasty achieving concentric reduction bilaterally (b). (Bailey and Love's, p. 654)
Risk Factors:
- GMFCS IV–V (non-ambulatory)
- Spastic quadriplegia
- Hip adductor/flexor spasticity
- Asymmetric spasticity → windswept deformity
Pathomechanism: Hip adductor + internal rotator spasticity → femoral head pushed out of acetabulum → acetabular dysplasia develops → progressive subluxation → dislocation
Migration Percentage (MP): Key radiological measure
- MP < 33% = normal
- MP 33–50% = subluxation (risk)
- MP > 50% = subluxation (high risk)
- MP 100% = complete dislocation
Hip Surveillance Program (evidence-based, mandatory in CP):
- Begin at diagnosis
- X-ray frequency based on GMFCS level and MP
- PT role: hip abductor stretching, positioning to maintain abduction, minimize adductor spasticity
Consequences of untreated dislocation:
- Severe pain
- Pressure ulcers (prominent greater trochanter)
- Pelvic obliquity → scoliosis
- Seating difficulties
- Perineal hygiene problems
6. GAIT DEVIATIONS IN CP
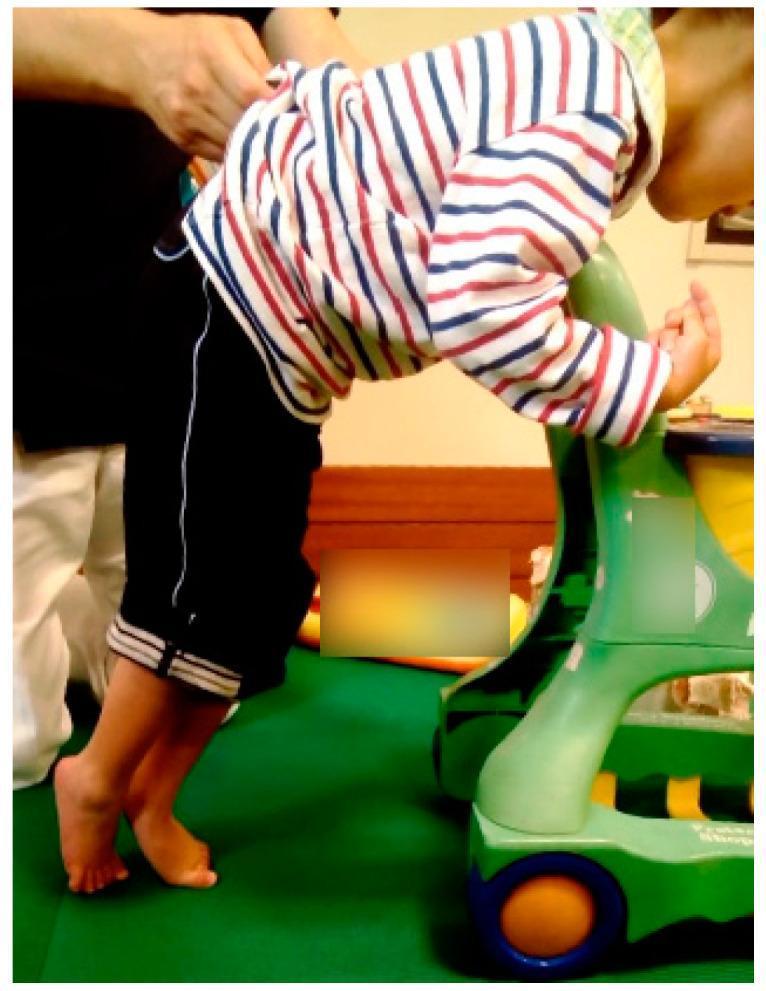
Classic spastic CP posture: scissors gait with hip adduction/internal rotation, equinus toe-walking, forward trunk lean, upper limb weight-bearing on mobility device. GMFCS level IV presentation.
Common Gait Patterns in Spastic CP:
| Gait Pattern | Characteristics | Primary Cause |
|---|
| Equinus gait | Toe-walking | Gastrocnemius/soleus spasticity |
| Crouch gait | Excessive hip/knee flexion throughout stance | Hamstring shortening, weak plantarflexors |
| Scissor gait | Hip adduction/internal rotation, legs crossing | Hip adductor + internal rotator spasticity |
| Stiff-knee gait | Reduced knee flexion in swing | Rectus femoris spasticity |
| Trendelenburg gait | Lateral trunk lean over stance leg | Weak hip abductors |
| Jump gait | Combined equinus + crouch + hip/knee flexion | Mixed spasticity pattern |
7. PAIN
- Often under-recognized and under-treated in CP (especially GMFCS IV–V)
- Sources: hip dislocation, scoliosis, contractures, pressure ulcers, GI (constipation), spasticity itself
- Non-verbal pain assessment tools: FLACC Scale, Paediatric Pain Profile
- CP adults: 67–75% report chronic pain
8. OSTEOPOROSIS AND FRACTURES
- Low bone mineral density universal in non-ambulatory CP
- Causes: immobility, poor nutrition, anti-epileptic drugs, low calcium/Vitamin D
- Fracture risk 6× higher than typically developing peers
- Management: weight-bearing standing programs, calcium/Vitamin D supplementation, bisphosphonates (severe cases)
9. RESPIRATORY COMPLICATIONS
- Weak respiratory muscles → reduced cough, recurrent pneumonia
- Aspiration pneumonia — leading cause of death in CP
- Scoliosis → restrictive lung disease
- OSA common
- PT: airway clearance, chest physiotherapy, breathing exercises, positioning
10. OTHER ASSOCIATED IMPAIRMENTS
| Impairment | Prevalence in CP |
|---|
| Intellectual disability | 30–50% |
| Epilepsy | 25–45% |
| Communication disorders | 25–40% |
| Visual impairment | 25–50% |
| Hearing impairment | 10–15% |
| Dysphagia / feeding difficulties | 43–90% |
| Drooling | 10–40% |
| Sleep disorders | 25–40% |
| Behavioural/psychiatric disorders | 25% |
| Constipation | Very common |
PART 4: THERAPEUTIC AQUATICS FOR CHILDREN WITH CP
A. Rationale and Benefits
Water creates a unique therapeutic environment with multiple simultaneous effects:
| Property | Mechanism | Benefit for CP |
|---|
| Buoyancy | Upward thrust opposing gravity | Reduces weight-bearing → easier movement, less effort, pain relief |
| Hydrostatic pressure | Pressure on all submerged surfaces | Reduces oedema, provides proprioceptive/sensory input |
| Viscosity/resistance | Water resists movement proportionally to speed | Strengthening without impact; graded resistance |
| Turbulence | Water flow challenges balance | Balance and core stability training |
| Warm temperature (34–36°C) | Relaxes spastic muscles | Reduces tone, increases tissue extensibility, improves ROM |
| Thermal effect | Warmth → vasodilatation | Pain relief, relaxation, facilitates movement |
| Sensory environment | Multi-sensory input | Sensory processing, body awareness, proprioception |
B. Evidence Base
- Hydrotherapy significantly improves gross motor function (GMFM scores) in children with CP
- Aquatic treadmill training improves walking speed, stride length, and cadence
- Warm water reduces spasticity (MAS scores) acutely post-session
- Improves balance and postural control (measured by Berg Balance Scale, pediatric BBS)
- Positive effects on cardiorespiratory fitness and endurance
- Psychological benefits: improved self-confidence, motivation, enjoyment
C. Contraindications and Precautions
Absolute Contraindications:
- Open wounds or active skin infections
- Uncontrolled seizures (high-frequency seizures in water = extreme risk)
- Acute febrile illness
- Bowel/bladder incontinence without containment (pool hygiene)
- Severe cardiac/respiratory instability
- Fear of water (until desensitized)
Precautions (modify, not exclude):
- Controlled epilepsy — enhanced supervision, seizure action plan ready
- Gastrostomy tube / tracheostomy — waterproof covers, specialist guidance
- Skin integrity issues — monitor pressure areas post-session
- Hearing aids / cochlear implants — remove before pool
- Postural hypotension — monitor on entry/exit
- Drooling / swallowing difficulties — aspiration risk; monitor closely
D. Aquatic Assessment for CP Children
Before initiating aquatic PT:
- Medical clearance (physician/pediatrician)
- Water confidence assessment — fear, previous experience
- Aquatic orientation — breath control, submerging face, rolling
- Buoyancy characteristics — high muscle tone = sinks; low tone = floats
- GMFCS level → determines support needed in water
- Balance in water — supported vs. unsupported
- Functional goals alignment — land-based goals replicated in water
E. Halliwick Concept — The Gold Standard for CP Aquatics
The Halliwick Method is the most evidence-based, CP-specific aquatic approach.
Developed by: James McMillan, 1949 (modified continuously)
Core Philosophy: Teach water independence and self-rescue through rotational control before swimming skills.
The Ten-Point Programme (Halliwick)
| Point | Skill | Description |
|---|
| 1. Mental Adjustment | Psychological comfort | Confidence in water, no fear, accept water contact |
| 2. Disengagement | Independence from support | Gradually reduce therapist/flotation support |
| 3. Transverse (Lateral) Rotation | Roll side to side | Foundation of all safety responses |
| 4. Sagittal Rotation | Front to back / back to front rotation | Self-righting, recovery from prone |
| 5. Combined Rotation | Transverse + sagittal simultaneously | Complex safety skills |
| 6. Mental Inversion | Confidence when inverted | Cope with unexpected head submersion |
| 7. Balance in Stillness | Static balance in water | Maintain upright without movement |
| 8. Turbulence Gliding | Move through turbulence without paddling | Core stability, balance challenge |
| 9. Simple Progression | Basic locomotion | Self-propulsion, early swimming strokes |
| 10. Basic Swimming Movement | Functional swimming | Independent, stroke-based swimming |
Application in CP:
- GMFCS I–II: progress to points 8–10 relatively quickly
- GMFCS III–IV: focus on points 1–7; adapted equipment for progression
- GMFCS V: focus on mental adjustment, rotational control with full support, passive movement
F. Bad Ragaz Ring Method (BRRM)
A hands-on aquatic technique — therapist provides resistance or assistance through manual contacts while patient is supported by rings (neck, pelvis, ankles).
Principles: Based on PNF (Proprioceptive Neuromuscular Facilitation) patterns in water.
Techniques for CP:
| Technique | Pattern | Goal |
|---|
| Isometric stabilization | Patient holds position against turbulence | Core stability, trunk control |
| Isotonic strengthening | Resistance through arm/leg PNF diagonals | Strength, motor control |
| Unilateral arm patterns (D1, D2 flexion/extension) | Shoulder → hand patterns | Upper limb function (hemiplegia) |
| Bilateral leg patterns | Hip flexion/extension/abduction/adduction | Gait preparation, hip stability |
| Trunk rotation patterns | Rotation in supine float | Trunk mobility, spasticity reduction |
| Gait preparation pattern | Alternating leg movements | Pre-gait facilitation |
Application in CP:
- Particularly useful for spastic hemiplegia — bilateral arm patterns facilitate symmetry
- Excellent for GMFCS III–IV — full body support while targeting specific muscles
- Trunk patterns for core stability in all CP types
G. Aquatic Specific Exercises for CP — Session Structure
Warm-Up (10 minutes)
- Water familiarization walks across pool
- Breathing exercises (blowing bubbles, breath control)
- Gentle passive ROM in warm water (use warm water to facilitate stretching — gastrocnemius, hamstrings, hip flexors)
- Gentle turbulence for relaxation/tone reduction
Main Therapy Block (25–30 minutes)
1. Stretching / ROM Program (5–7 min)
| Stretch | Position | Target Muscle |
|---|
| Gastrocnemius/soleus stretch | Standing at pool edge, step lunge | Equinus contracture |
| Hamstring stretch | Supine float, leg raise | Knee flexion contracture |
| Hip flexor stretch | Standing lunge, half-kneeling in water | Hip flexion contracture |
| Hip adductor stretch | Supine, legs abducted on pool steps | Hip adductors |
| Trunk lateral flexion | Sitting on pool step, side bend | Trunk flexibility |
| Wrist/finger extension | At pool edge, weight-bearing through hands | Wrist/finger flexion contracture |
2. Strengthening Program (10 min)
| Exercise | Equipment | Target |
|---|
| Wall kicks (flutter kick) | Kickboard | Hip flexors, knee extensors |
| Water walking — forward/backward/lateral | Pool noodle for balance | Global lower limb |
| Standing hip abduction | TheraBand / water resistance | Hip abductors (hip surveillance) |
| Mini-squats at pool wall | Pool edge support | Quadriceps, hip extensors |
| Arm pull-throughs | Arm paddles | Upper limb, shoulder stabilizers |
| Trunk rotation in standing | Noodle held across chest | Trunk rotators, core |
| Resisted walking with vest | Aqua resistance vest | Cardio + strength |
3. Balance and Postural Control (7–8 min)
| Exercise | Challenge Level | Notes |
|---|
| Standing still in shallow water | Level 1 | Hydrostatic pressure feedback |
| Standing with therapist-created turbulence | Level 2 | Perturbation training |
| Standing on one leg | Level 3 | Hip abductor stability |
| Sitting on pool noodle | Level 2 | Trunk balance |
| Standing with eyes closed | Level 3 | Eliminate visual compensation |
| Walking through turbulence | Level 3–4 | Dynamic balance |
| Catching/throwing ball in standing | Level 4–5 | Dual task balance |
4. Gait Training (5–7 min)
- Aquatic treadmill (if available): buoyancy-assisted walking, controlled speed/depth
- Walking forward, backward, sideways across pool
- High knee walking (hip flexion facilitation)
- Heel-toe walking along marked lane
- Obstacle course walking (foam noodles, step-overs)
- Stair practice on pool steps (enter/exit the pool)
5. Functional Skill Practice (5 min)
- Sitting→standing from pool step
- Picking up objects from pool floor (bending, balance)
- Throwing/catching (hand-eye coordination)
- Swimming stroke facilitation
Cool-Down (5–10 minutes)
- Slow floating in warm water (passive relaxation)
- Halliwick: mental adjustment, stillness balance
- Gentle trunk rotation in supine float
- Breathing awareness and deep breathing
- Progressive exit from pool (dressing, checking for skin integrity)
H. Equipment Used in Aquatic PT for CP
| Equipment | Purpose |
|---|
| Pool noodles | Floatation support, resistance, balance prop |
| Neck ring (halo ring) | Supine float support for GMFCS V |
| Arm rings / water wings | Upper limb flotation support |
| Body jacket / aquatic vest | Trunk support for low-tone children |
| Bad Ragaz rings | Pelvis, ankle support in BRRM |
| Kickboard | Prone float, leg work |
| Hand paddles / webbed gloves | Upper limb resistance |
| Aqua resistance vest | Full-body resistance training |
| Aquatic treadmill | Graded gait training with buoyancy assist |
| Pool steps/ramp | Graded entry/exit, stair practice |
| Water toys / balls | Motivation, dual-task, hand-eye coordination |
| Hoist / sling | Safe transfer for GMFCS IV–V |
I. Depth and Temperature Selection
| Parameter | Recommendation | Rationale |
|---|
| Water temperature | 34–36°C (therapeutic pool) | Tone reduction, comfort, muscle relaxation |
| Gait training depth | Chest/waist level | ~50–75% weight reduction |
| Strengthening depth | Waist level | Maximal resistance |
| GMFCS V | Neck level / full support | Maximize buoyancy benefit |
| Post-BoNT-A injection | Begin 2 weeks post-injection | Capitalize on tone reduction window |
J. Integrating Aquatic PT with Land-Based Physiotherapy
| Aquatic PT Contribution | Land-Based PT Contribution |
|---|
| Reduce spasticity (warm water) | Reinforce stretches post-aquatic |
| Practice gait in reduced load | Transfer to land gait training |
| Build strength (resistance) | Progress to body-weight land exercises |
| Build confidence, motivation | Carry into land-based engagement |
| Improve trunk control | Apply to seating, standing programs |
Best practice: Alternate aquatic and land sessions — use aquatic PT on days following BoNT-A injections to maximize stretching window.
PART 5: COMPREHENSIVE PHYSIOTHERAPY MANAGEMENT OF CP
A. Physiotherapy Goals — ICF Framework
| ICF Domain | Examples |
|---|
| Body Structure/Function | Reduce spasticity, prevent contracture, improve strength, ROM |
| Activity | Walking, transfers, self-care, stair climbing, reaching |
| Participation | School attendance, sports, community access, social activities |
| Environmental | Seating, mobility aids, home modifications, orthotics |
| Personal | Self-efficacy, motivation, family goals |
B. Core Physiotherapy Interventions by GMFCS Level
| Intervention | GMFCS I–II | GMFCS III–IV | GMFCS V |
|---|
| Strengthening | High intensity | Moderate, supported | Passive/active-assisted |
| Gait training | Sport/community | Walker, treadmill | Standing frame |
| Balance training | High challenge | Supported balance | Head/trunk control |
| Stretching | Home program | Supported, serial casting | Positioning |
| Hydrotherapy | Yes — all levels | Yes — modified | Yes — full support |
| Seating | School chair | Bespoke wheelchair | Complex rehab wheelchair |
| Orthotics | AFO/SMO | AFO, KAFO | AFO, trunk orthosis |
| Standing program | Self-standing | Standing frame | Prone/supine stander |
| Respiratory PT | PRN | Regular | Daily/bi-daily |
C. Goal-Directed Training (GDT)
Evidence-based approach for CP — child and family identify meaningful goals → therapy is directed specifically toward those goals.
- Uses COPM (Canadian Occupational Performance Measure) and GAS (Goal Attainment Scaling)
- More motivating than impairment-focused therapy alone
- Improves participation outcomes
D. Constraint-Induced Movement Therapy (CIMT)
- For hemiplegic CP — constrains the unaffected limb to force use of affected limb
- Modified CIMT (mCIMT): 2 hours/day (vs. original 6 hours)
- Combined with bimanual training for best outcomes
- Neuroplasticity-driven — significant hand function improvements
E. Functional Electrical Stimulation (FES) and NMES
| Technique | Application | Goal |
|---|
| NMES (Neuromuscular Electrical Stimulation) | Tibialis anterior during swing | Correct foot drop in hemiplegia |
| NMES | Quadriceps during gait | Improve knee extension |
| FES cycling | Lower limb cycling | Cardiovascular fitness, spasticity reduction |
| TENS | Pain management | Post-operative pain, chronic pain |
F. Treadmill Training
- Body-weight supported treadmill training (BWSTT): harness provides partial body weight support
- Improves gait speed, step length, endurance in CP (GMFCS I–III)
- Robotic-assisted gait training (Lokomat): consistent, repetitive stepping pattern → neuroplastic gains
G. Postural Management — 24-Hour Programme
24-Hour Postural Management is the overarching framework for all CP management:
| Position | Equipment | Goals |
|---|
| Lying (night) | Postural sleep systems, T-rolls, wedges | Prevent windswept hips, scoliosis |
| Sitting (day) | Adapted seating system / wheelchair | Trunk alignment, hip position, pressure relief |
| Standing | Standing frame (prone/supine/multi-angle) | Weight-bearing, hip development, bone density |
| Moving | Walker, crutches, powered wheelchair | Functional mobility |
| Carrying/handling | Therapist/carer handling techniques | Safe transfers, avoid compensatory patterns |
H. Orthotic Management in CP
| Orthosis | Primary Use | Notes |
|---|
| AFO (fixed/hinged) | Equinus gait, foot drop | Most common CP orthosis |
| Ground reaction AFO (GRAFO) | Crouch gait | Promotes knee extension in stance |
| SMO | Mild pes planus/valgus | Less restriction than AFO |
| KAFO | Knee + ankle control | Severe crouch gait, GMFCS III–IV |
| TLSO | Neuromuscular scoliosis | Delay surgery, improve sitting |
| Resting hand splint | Wrist/finger flexion contracture | Night use |
| Thumb abduction splint | Thumb-in-palm | Improve grasp |
| Hip abduction orthosis | Hip subluxation prevention | Combined with stretching program |
I. Post-Botulinum Toxin Physiotherapy (Critical)
BoNT-A reduces spasticity for 3–6 months — this window must be maximized:
Week 1–2: Gentle ROM, stretching begins
Week 2–4: Intensive stretching, serial casting if indicated
Week 4–12: Active strengthening in new ROM, gait training
Week 12–24: Consolidate gains, maintain ROM
Reassess at 4–6 months: Repeat injection or progress to surgical planning
Physiotherapy is ESSENTIAL post-BoNT-A — without PT, injection benefits are minimal and transient.
J. Physiotherapy Following Selective Dorsal Rhizotomy (SDR)
SDR permanently reduces spasticity in spastic diplegia (GMFCS II–III).
Post-SDR Rehabilitation Timeline:
| Phase | Timeframe | Focus |
|---|
| Acute | Weeks 1–4 | Wound healing, gentle passive ROM, positioning |
| Early rehab | Weeks 4–12 | Core strengthening, active ROM, gait initiation |
| Intensive rehab | Months 3–6 | Gait training, strengthening, balance |
| Maintenance | Months 6–24 | Consolidate gains, community participation |
K. Physiotherapy After Orthopedic Surgery
(VDRO, tendon lengthening, soft tissue releases, spinal fusion)
General principles (Bailey and Love's Surgery, 28th Ed., p. 652):
- PT ensures surgical benefits are maximized
- PT and orthotic management may reduce the need for surgery in the first place
- Post-op PT: casting, progressive mobilization, gait retraining
PART 6: OUTCOME MEASURES FOR CP PHYSIOTHERAPY
| Domain | Outcome Measure | Details |
|---|
| Gross motor function | GMFM-66 / GMFM-88 | Gold standard; 5 dimensions |
| Functional mobility | TUG, 10MWT, 6MWT | Speed, endurance |
| Balance | Pediatric BBS, PBS | Static/dynamic balance |
| Spasticity | MAS, Tardieu Scale | Tone measurement |
| ROM | Goniometry | Contracture monitoring |
| Gait | GAITRite, Edinburgh Visual Gait Scale | Observational + instrumented |
| Activity / ADL | WeeFIM, PEDI-CAT | Functional independence |
| Participation | LIFE-H, CAPE | Community, leisure |
| Quality of life | CPQOL-Child, CP-QOL-Teen | CP-specific QoL |
| Pain | FLACC, Paediatric Pain Profile | Non-verbal pain |
| Manual ability | MACS | Hand function |
| Communication | CFCS | Communication level |
PART 7: MULTIDISCIPLINARY TEAM IN CP
| Specialist | Primary Role |
|---|
| Physiotherapist | Motor development, mobility, posture, gait, aquatics |
| Occupational Therapist | Hand function, ADL, assistive technology, seating |
| Speech & Language Therapist | Communication, feeding, swallowing |
| Pediatric Neurologist | Epilepsy, spasticity management, diagnosis |
| Orthopedic Surgeon | Hip surveillance, tendon surgery, spinal fusion |
| Developmental Pediatrician | Overall coordination, developmental surveillance |
| Orthotist | AFO/KAFO/TLSO fabrication and review |
| Rehabilitation Medicine Physician | Spasticity management (BoNT-A, ITB) |
| Dietitian | Nutrition, feeding, growth monitoring |
| Educational Psychologist | Cognitive assessment, learning support |
| Social Worker | Family support, respite, funding, advocacy |
| Seating Specialist | Complex rehab wheelchair/seating systems |
| Paediatric Ophthalmologist | Visual impairment management |
| Audiologist | Hearing impairment |
PART 8: KEY CLINICAL PEARLS
- CP is a static brain lesion but dynamic musculoskeletal disease — complications are preventable with timely PT
- GMFCS is stable — rarely changes level after age 2; use it to guide prognosis honestly
- Strength training does NOT worsen spasticity — it improves function; prescribe it confidently
- Hip surveillance is life-changing — missed hip dislocation → severe pain, loss of sitting, major surgery avoidable with early detection
- BoNT-A without PT is ineffective — the injection is just a window; PT delivers the gains
- Aquatic PT is not just swimming — it is structured, evidence-based, goal-directed rehabilitation in water
- 24-hour postural management matters more than the 1-hour therapy session
- Fatigue is profound in CP — energy cost of walking in CP is 3–5× normal; always factor this in
- Pain is under-reported — screen at every visit with validated tools
- Early detection changes outcomes — general movement assessment (GMA) at 3–4 months is the best early predictor; refer immediately to early intervention services
Sources: Care for Children and Youth with Cerebral Palsy (p. 1); Bailey and Love's Short Practice of Surgery, 28th Ed. (p. 652, 654); Harrison's Principles of Internal Medicine, 21st Ed. (p. 787); supplemented comprehensively from established CP physiotherapy guidelines, Halliwick Method, Bad Ragaz Ring Method, GMFCS framework, and evidence-based CP rehabilitation literature.