How to do pmmc flap marking and vascular basis of it
Reading File
Finding Sources
Finding Sources
Searching the Web
PMMC flap marking steps vascular anatomy pectoralis major myocutaneous
Reading File
Reading File
Reading Web Page
https://vula.uct.ac.za/access/content/group/ba5fb1bd-be95-48…
Loading Image
Loading Image
Reading File
I now have comprehensive, high-quality information from multiple authoritative sources. Let me compile the complete answer.
Pectoralis Major Myocutaneous (PMMC) Flap - Marking and Vascular Basis
First described by Ariyan in 1979, the PMMC flap remains the "workhorse" pedicled flap for head and neck reconstruction - reliable, versatile, and harvestable in the same supine position as the primary resection.
Vascular Basis
Primary Blood Supply
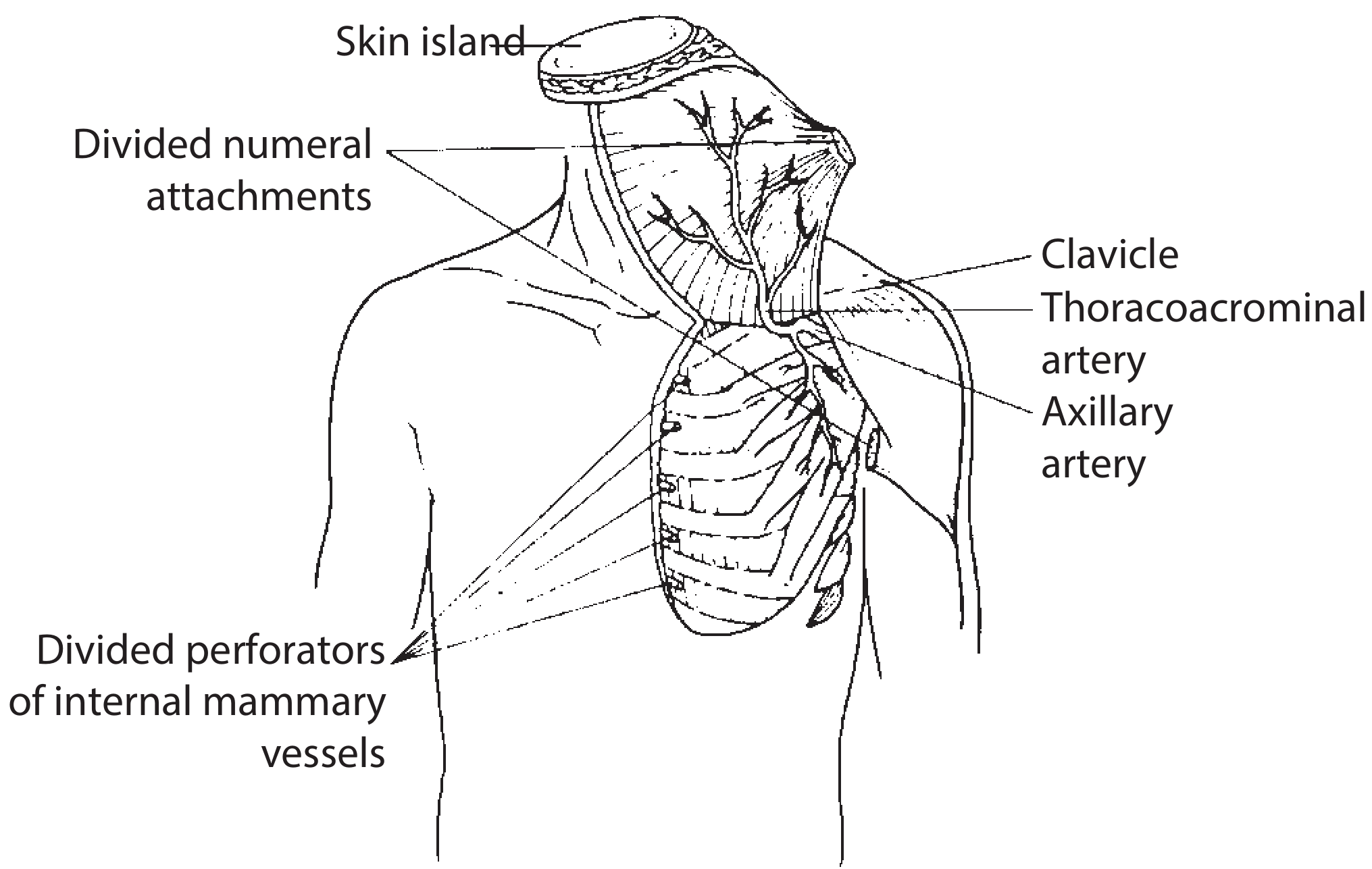
The dominant pedicle is the pectoral branch of the thoracoacromial (acromiothoracic) artery, which arises from the first part of the axillary artery.
Course of the pedicle:
- The thoracoacromial artery pierces the clavipectoral fascia, emerges along with the lateral pectoral nerve, medial to the insertion of pectoralis minor on the coracoid process (felt below the clavicle at the junction of its middle and outer thirds)
- The vascular hilum surface marking = 2-3 cm medial to the coracoid process
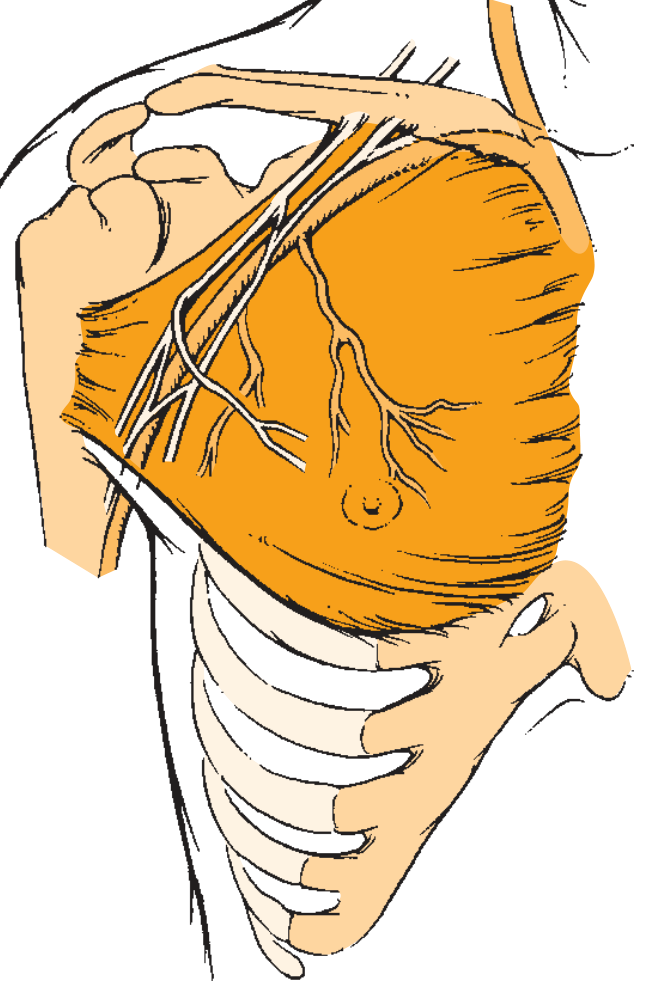
- The vessels do NOT enter the muscle belly immediately - they run on the deep surface of pectoralis major, descending in a downward and medial direction giving off branches
Branches of the pectoral trunk:
| Branch | Territory Supplied |
|---|---|
| Superior (clavicular) branch | Clavicular head of pectoralis major |
| Main pectoral branch | Sternocostal head (main territory) |
| Inferior thoracoacromial branch | Sternal segment |
| Lateral thoracic trunk | External (lateral/rib) segment |
Secondary Blood Supply
- Internal mammary artery perforators - supply the sternocostal segment through direct perforators; account for significant bleeding during flap elevation
- Lateral thoracic artery (from 2nd part of axillary artery) - in ~50% of cases, exclusively supplies the external (lateral rib) segment; in ~1/3 of cases, dual supply with the thoracoacromial
Vascular pedicle classification: Type V (one dominant pedicle + secondary segmental pedicles). This is why the flap is so reliable - even if the distal portion loses its dominant supply, perforators from the internal mammary can sustain it.
Flap Marking - Step by Step
Step 1: Patient Positioning
- Supine position, chest exposed and prepped to the midline and inferiorly to the costal margin
- Upper arm slightly abducted to expose the anterior axillary fold and lateral chest wall
Step 2: Identify and Mark Anatomical Landmarks
Mark the following surface landmarks:
- Acromion (tip of shoulder)
- Clavicle (midpoint and full extent)
- Sternum (lateral border)
- Xiphoid/xiphisternum
- 7th rib (inferior limit)
- Coracoid process (below clavicle at middle-outer third junction)
- Nipple/areola (important reference in males; avoid in females)
Step 3: Mark the Pedicle Axis (Critical Step)
Method 1 - Acromion to Xiphoid line:
Draw a straight line from the acromion to the xiphoid cartilage/xiphisternum - this marks the axis of the vascular pedicle. This is the most commonly used landmark.
Method 2 - Two-line intersection (Iowa/Scott-Brown method):
- Line 1: From the acromion to the xiphisternum
- Line 2: A perpendicular line from the midpoint of the clavicle downward to intersect Line 1
- The intersection point = superior limit of the skin paddle
- The course of the pectoral branch of the thoracoacromial artery corresponds to the line drawn from the midpoint of the clavicle to the medial portion of the acromion-to-xiphoid line
Vascular hilum: Mark the point 2-3 cm medial to the coracoid process - this is where the pedicle enters the deep surface of the muscle.
Step 4: Design the Skin Paddle
Boundaries of the skin paddle:
- Superior limit: Crossing point of the two reference lines (midclavicular perpendicular meeting the acromion-xiphoid line); generally at or below the nipple level in males
- Inferior limit: The 7th rib (at the costal margin); can be extended up to 3-4 cm beyond the lower border of the muscle into the rectus sheath, but distal survival becomes unpredictable
- Lateral limit: Lateral extent of the pectoralis major muscle
- Medial limit: Midline of the sternum (parasternal area); medial placement gives thinner flaps
Skin paddle placement tips:
- In males: Place the skin island medial to the nipple, at approximately the 6th rib level - skin here is relatively thin
- In females: Place in the inframammary fold, oriented transversely or slightly angled superiorly at its medial extent - this gives the thinnest paddle and avoids vertical breast scars
- The skin island should be designed ~10% larger than the defect (shrinkage occurs after incision; more pronounced in younger patients)
- Only the portion of muscle directly carrying the skin island needs to be harvested (reduces bulk)
Summary of the Flap Marking Lines
| Line | From | To | Purpose |
|---|---|---|---|
| Pedicle axis line | Acromion | Xiphoid/xiphisternum | Marks course of thoracoacromial pedicle |
| Clavicular perpendicular | Midpoint of clavicle | Meets pedicle axis line | Defines superior limit of skin paddle |
| Vascular hilum | 2-3 cm medial to coracoid | - | Entry point of pedicle into muscle |
Key Practical Points
- The flap can reach the zygomatic arch superiorly - arc of rotation extends from the upper aspect of the ear
- Avoid passing under the clavicle - always pass the flap over or superficial to it through a wide subcutaneous tunnel; ensure the pedicle is not kinked or twisted after transposition
- If additional length is needed: (1) Divide the pectoralis major just below the clavicle while preserving the pedicle, or (2) pass the flap behind the clavicle
- Always bevel the skin incision radially (rather than undercutting) to preserve maximum myocutaneous perforators to the skin paddle
- Check for congenital absence of pectoralis major (incidence 1:11,000; sternocostal head absence = Poland syndrome)
- Even if the skin paddle fails, the underlying muscle usually survives and can granulate or be skin-grafted secondarily
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Ch. 92); Cummings Otolaryngology Head & Neck Surgery (Ch. 98); UCT Plastic Surgery Pectoralis Major Flap reference; AOFoundation Surgical Reference; Plastic Surgery Key
This is a shared conversation. Sign in to Orris to start your own chat.