I already have all the information and images needed from the previous research session. Let me put together a clear, easy-to-understand guide with pictures now.
🫀 CTG (Cardiotocography) - Easy Guide with Pictures
What is a CTG?
CTG is a machine that records two things at the same time on a paper strip:
- Top line = Fetal Heart Rate (FHR) - measured in beats per minute (bpm)
- Bottom line = Uterine Contractions - pressure of the womb tightening
Two sensors are placed on the mother's belly:
- One over the fetal heart (Doppler ultrasound)
- One at the fundus (to detect contractions)
📊 How to Read a CTG - The 5 Features (DR C BraVaDo)
| Letter | Feature | What to look for |
|---|
| DR | Define Risk | Is it high or low risk? |
| C | Contractions | How many per 10 min? (normal ≤5) |
| Bra | Baseline Rate | Normal = 110-160 bpm |
| Va | Variability | Normal = 5-25 bpm fluctuation |
| D | Decelerations | Any dips? What type? |
| o | Oxytocin/Accelerations | Any heart rate spikes? (good sign) |
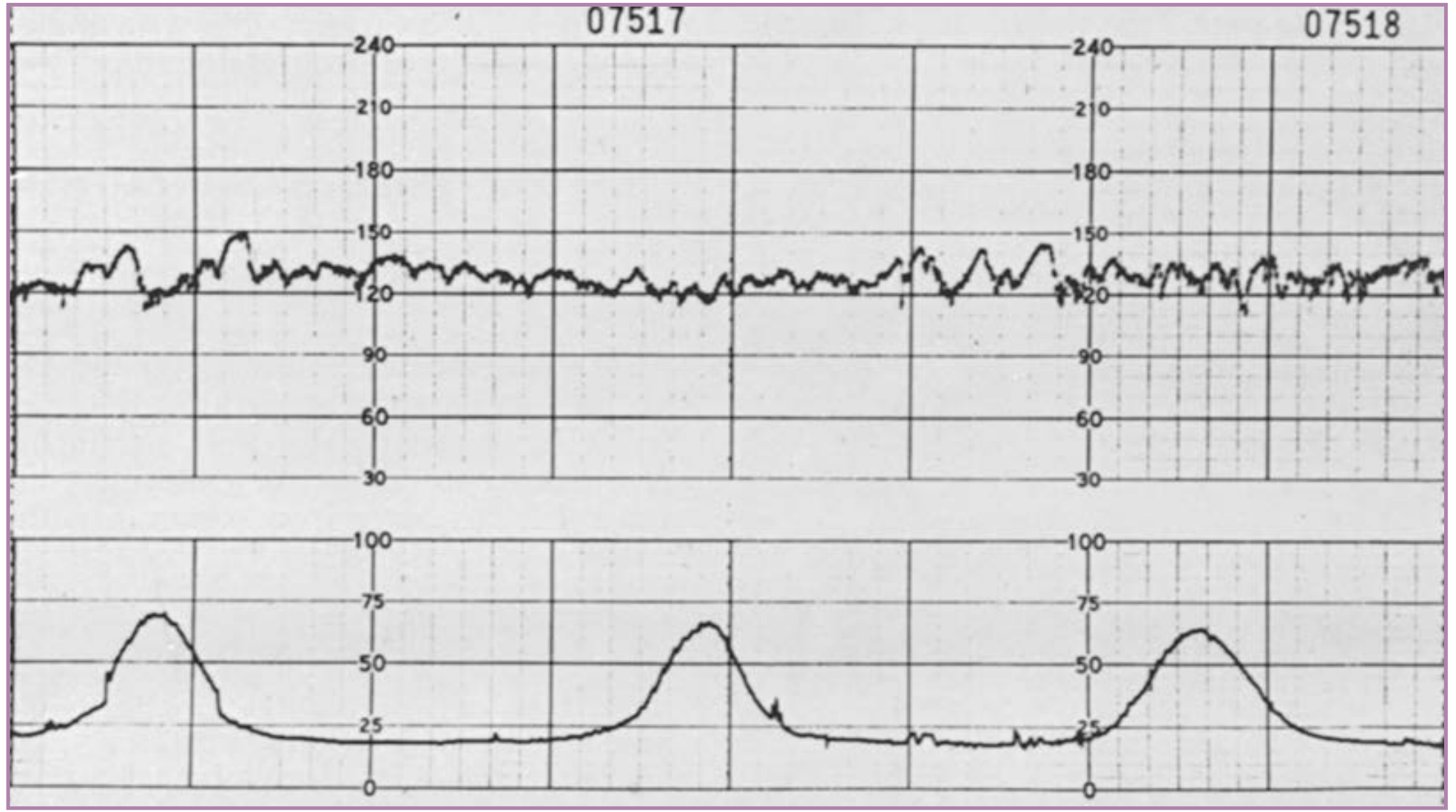
1. BASELINE RATE
The average FHR over 10 minutes, ignoring accelerations and decelerations.
| Finding | Rate | Meaning |
|---|
| Normal | 110-160 bpm | Healthy fetus |
| Tachycardia | >160 bpm | Fever, infection, hypoxia, drugs |
| Bradycardia | <110 bpm | Fetal distress, cord compression, maternal drugs |
2. VARIABILITY
This is how much the heart rate "wiggles" up and down around the baseline. A healthy, awake baby's heart rate should bounce around constantly - it should NOT be a flat line.
| Variability | Range | Meaning |
|---|
| Normal | 5-25 bpm | Healthy CNS + cardiovascular system |
| Reduced | <5 bpm for >40-90 min | Hypoxia, sleep cycle, drugs (opioids, MgSO4) |
| Absent | Flat line | Serious - possible severe hypoxia/acidosis |
| Increased/Saltatory | >25 bpm for >25 min | Acute hypoxia, cord compression |
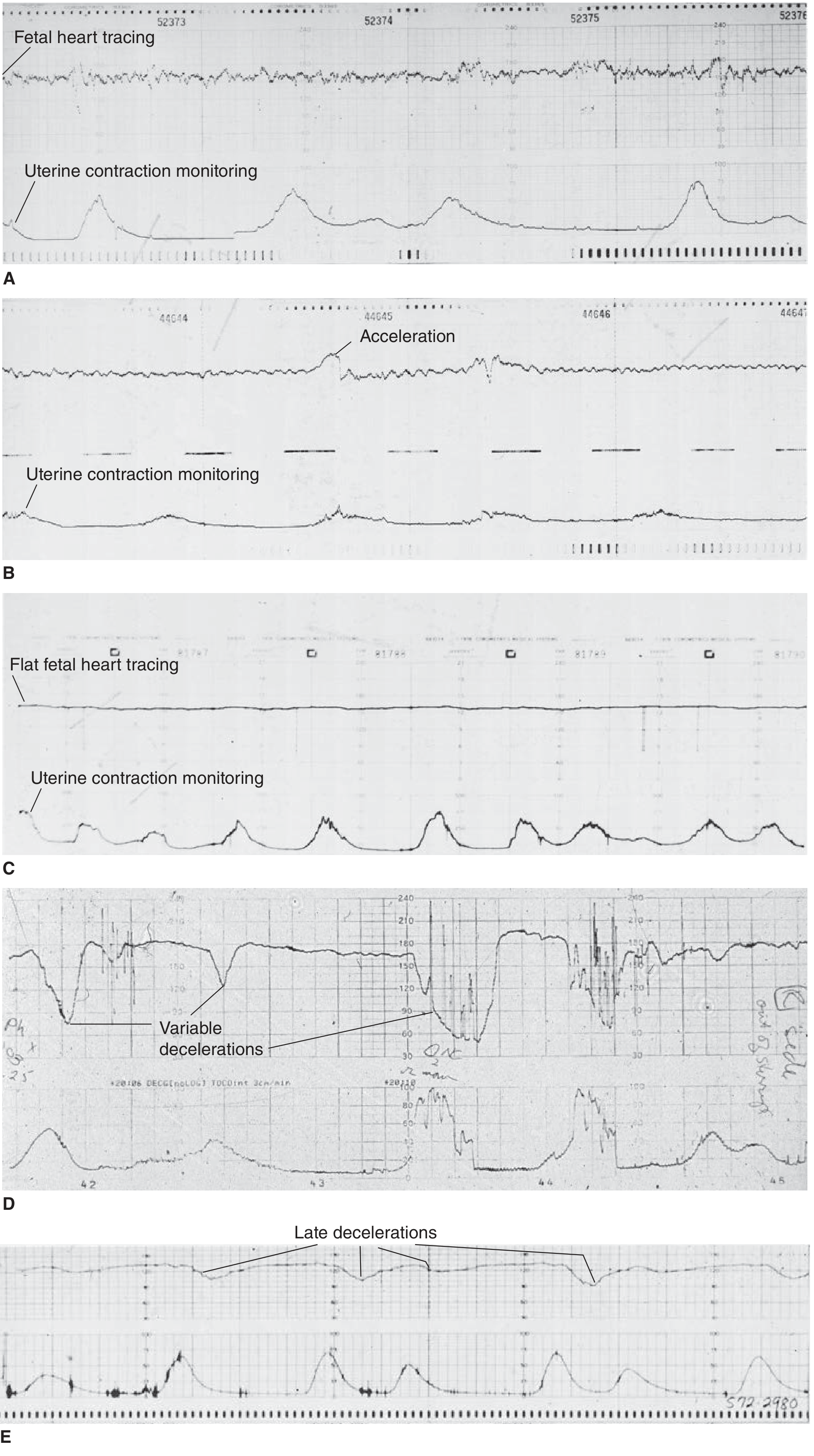
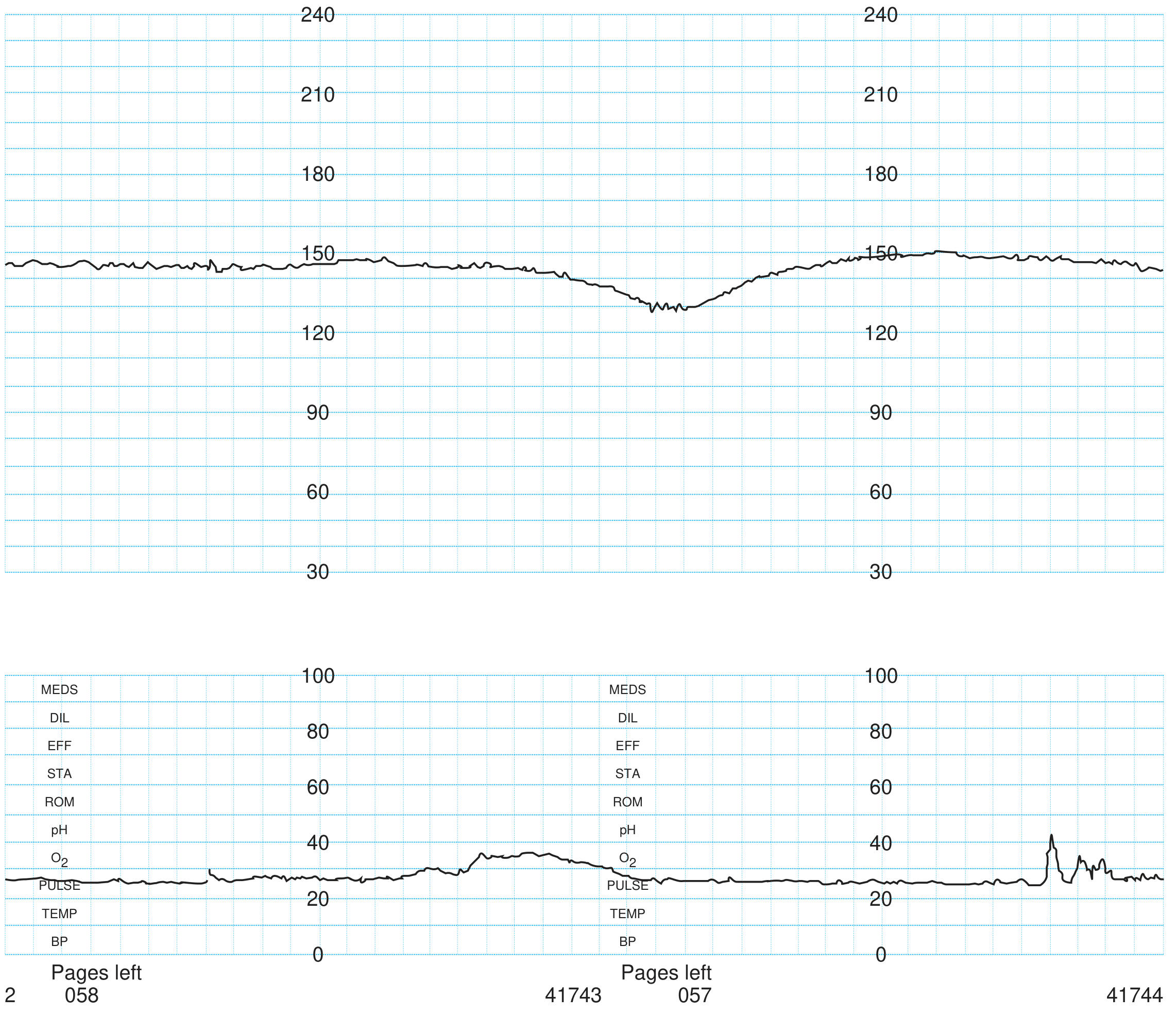
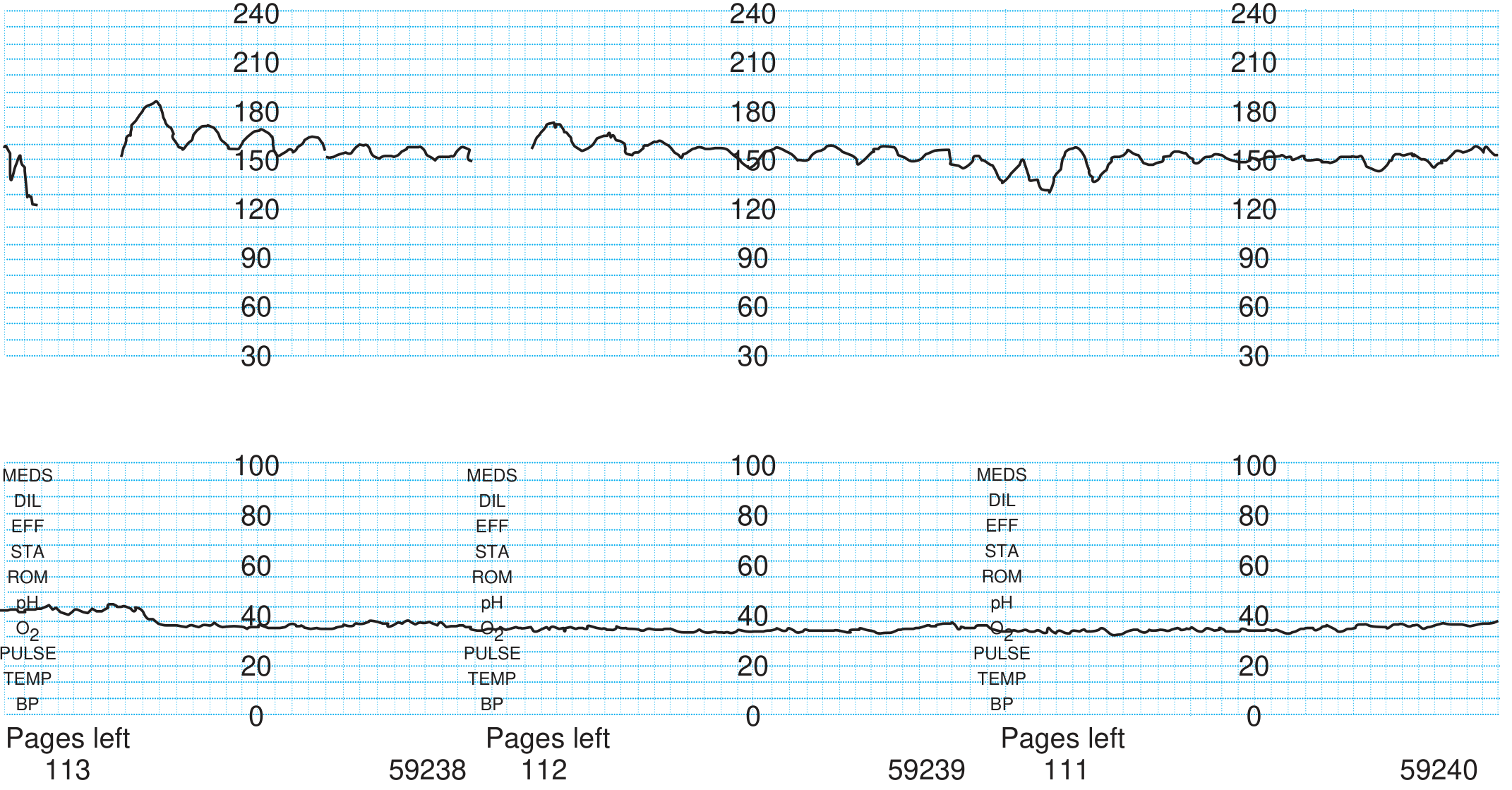
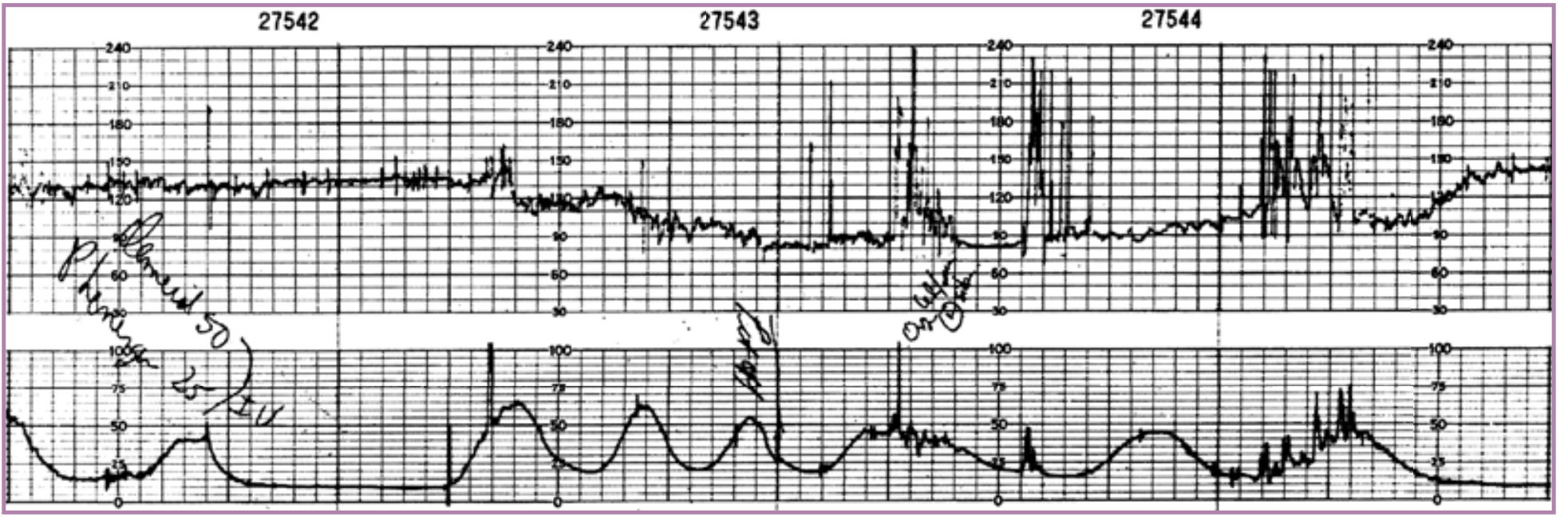
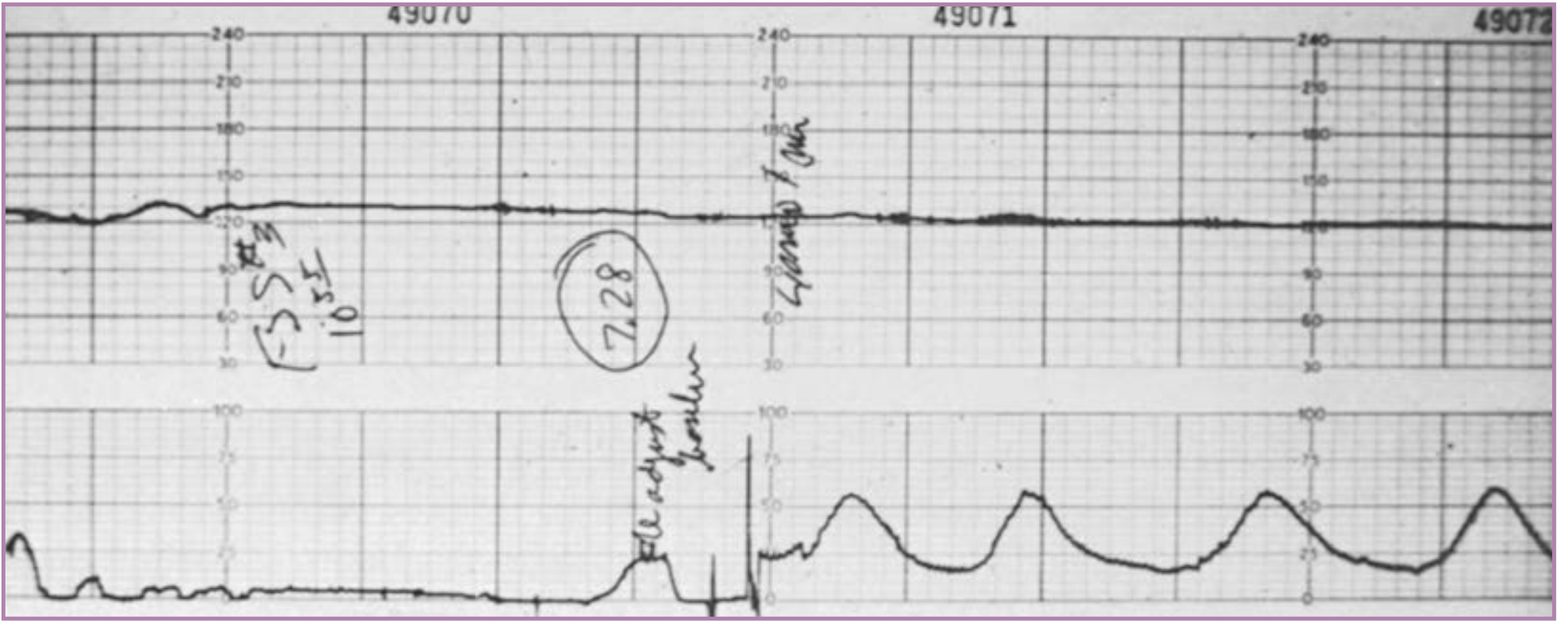
Here is a real CTG tracing showing several patterns - good variability (A, B), flat/absent variability (C), variable decelerations (D), and late decelerations (E):
A = Good variability (normal, reassuring). B = Good variability with accelerations (very reassuring). C = Flat/poor variability - may indicate fetal hypoxia. D = Variable decelerations (cord compression). E = Late decelerations (uteroplacental insufficiency).
3. ACCELERATIONS
Temporary rises in FHR of ≥15 bpm lasting ≥15 seconds.
- Presence = REASSURING - means fetus is not acidotic
- Caused by fetal movement stimulating the sympathetic nervous system
- Form the basis of the Non-Stress Test (NST)
- Reactive NST = at least 2 accelerations in 20-30 minutes
4. DECELERATIONS - The Most Important Part ⚠️
Decelerations = drops in FHR of >15 bpm lasting >15 seconds.
There are 4 types - each with a different cause and significance:
🟢 Type 1: EARLY Decelerations (Benign)
| Feature | Detail |
|---|
| Shape | Gradual, smooth, uniform dip |
| Timing | Mirror the contraction - start and end WITH it |
| Nadir | Coincides with the peak of contraction |
| Cause | Fetal head compression → vagal stimulation |
| Significance | Normal/benign - not pathological |
Think of it as: the baby's head gets squeezed during a contraction, slows the heart briefly, then recovers. No fetal distress.
🔴 Type 2: LATE Decelerations (Most Ominous)
| Feature | Detail |
|---|
| Shape | Gradual, smooth dip |
| Timing | Start AFTER the contraction begins, recover AFTER it ends |
| Nadir | Occurs >30 seconds after peak of contraction |
| Cause | Uteroplacental insufficiency → fetal hypoxia |
| Significance | Pathological - indicates fetal compromise |
Think of it as: the placenta isn't delivering enough oxygen. When the womb contracts, blood flow drops even further, and the heart slows - but only AFTER the contraction.
Causes: maternal hypotension, pre-eclampsia, abruption, postmaturity, IUGR, oxytocin hyperstimulation
🟡 Type 3: VARIABLE Decelerations (Most Common)
| Feature | Detail |
|---|
| Shape | Abrupt, sharp, V-shaped or W-shaped |
| Timing | Variable - no consistent relationship to contractions |
| Onset to nadir | <30 seconds (abrupt) |
| Duration | 15 seconds to <2 minutes |
| Cause | Umbilical cord compression |
| Significance | Isolated = not concerning; Persistent = worrying |
Reassuring "shoulders" = small accelerations just before and after the dip (fetus compensating well)
Atypical/concerning features:
- Drop to <60 bpm
- Duration >60 seconds
- Slow return to baseline
- Loss of variability during the deceleration
- No shoulders
🔴 Type 4: PROLONGED Decelerations
| Feature | Detail |
|---|
| Duration | 2-10 minutes with drop >15 bpm |
| Cause | Cord prolapse, maternal hypotension, uterine rupture, abruption |
| Significance | Always abnormal - requires immediate action |
Drop >10 minutes = new baseline (bradycardia)
5. SINUSOIDAL PATTERN 🚨
A smooth, sine wave-like pattern, ≥10 minutes with:
- Regular oscillations at 2-5 cycles/min
- Amplitude 5-15 bpm
- No accelerations
- No short-term variability
Causes: Severe fetal anaemia (Rh isoimmunization, fetal-maternal haemorrhage), severe hypoxia
This is a MEDICAL EMERGENCY - requires immediate delivery
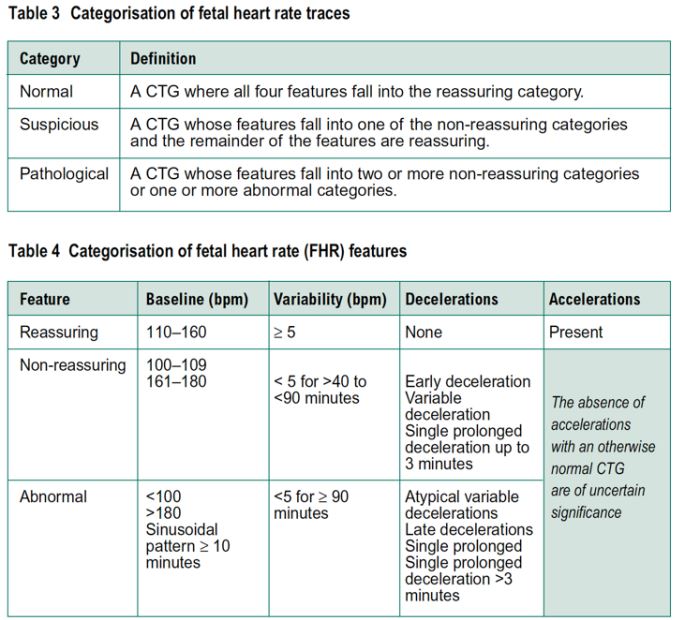
📋 CTG CLASSIFICATION (NICE Guidelines)
| Category | Definition | Action |
|---|
| Normal | ALL features reassuring | Continue monitoring |
| Suspicious | 1 non-reassuring feature (rest reassuring) | Correct reversible causes, closer monitoring |
| Pathological | 2+ non-reassuring OR 1+ abnormal features | Urgent action - consider delivery |
Feature Classification Quick Reference:
| Feature | Reassuring | Non-Reassuring | Abnormal |
|---|
| Baseline | 110-160 bpm | 100-109 or 161-180 | <100 or >180, sinusoidal ≥10 min |
| Variability | 5-25 bpm | <5 for 40-90 min or >25 for 15-25 min | <5 for ≥90 min |
| Decelerations | None | Early; Variable <90 min | Late; Atypical variable; Prolonged >3 min |
| Accelerations | Present | Absent (uncertain significance) | - |
🛠️ Management When CTG is Abnormal
Correct reversible causes first (ALSO mnemonic):
| Letter | Action |
|---|
| A | Assess maternal position (left lateral) |
| L | Lower oxytocin / stop if running |
| S | Stop pushing / maternal effort |
| O | Oxygen (though evidence is mixed) |
Then escalate:
- Suspicious → continue monitoring, repeat VE
- Pathological → consider fetal blood sampling (scalp pH <7.20 = acidosis) or expedite delivery
- Sinusoidal / prolonged bradycardia → emergency caesarean section
🧠 Quick Memory Summary
Normal CTG = "CAVE"
C - Contractions ≤5 per 10 min
A - Accelerations present
V - Variability 5-25 bpm
E - no dEcelerations (or only early ones)
Baseline: 110-160 bpm
Sources: Tintinalli's Emergency Medicine (McGraw-Hill), Mulholland & Greenfield's Surgery, Creasy & Resnik's Maternal-Fetal Medicine, NICE Guidelines 2017 (updated),
ZeroToFinals CTG