Suprapatellar imil nail
Reading File
Finding Sources
Finding Sources
Searching the Web
suprapatellar intramedullary nail tibial fracture technique
Reading File
Reading File
Searching PubMed
suprapatellar tibial intramedullary nailing
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information. Here is a detailed, well-sourced overview of the suprapatellar intramedullary (IM) nail for tibial fractures.
Suprapatellar Intramedullary Nail (Tibial Nailing)
What It Is
The suprapatellar (SP) approach for tibial IM nailing is an alternative nail insertion technique where the incision is made above the patella through the quadriceps tendon, and nailing is performed with the knee in a semi-extended position (15-20° of flexion). This contrasts with the traditional infrapatellar approach, where the knee is hyperflexed and access is through or beside the patellar tendon.
Indications
SP nailing is applicable to most diaphyseal and metadiaphyseal tibial fractures. It is particularly advantageous for:
- Proximal tibia fractures - where achieving an ideal starting point is obstructed in infrapatellar approaches by the patella
- Distal tibia fractures - evidence shows improved sagittal alignment
- Obese patients - the semi-extended position makes imaging and nailing mechanically easier
- Fractures where malalignment is high risk (e.g., where blocking screws alone may be insufficient)
Relative caution applies to high-grade open fractures (Gustilo III), as the approach enters the knee joint, raising concern for septic arthritis.
- Rockwood and Green's Fractures in Adults, 10th ed., p. 3192
Surgical Technique
Positioning
- Patient supine on radiolucent table
- Knee supported in ~15-20° of flexion (semi-extended) on a foam/radiolucent triangle placed under the proximal tibia (NOT under the knee or distal femur) to allow slight anterior shift of the tibia relative to the trochlea and the suprapatellar cannula

Intraoperative setup: knee in semi-extended position, foam support under the proximal tibia, guidewire inserted through suprapatellar incision.
Incision & Entry
- Midline incision starting at the superior pole of the patella, extending 5 cm proximally
- The quadriceps tendon is split longitudinally
- The knee joint is entered from above (suprapatellar pouch)
- Specialized protective trocars/cannulas are used to protect the patellofemoral articular cartilage from guidewires, reamers, and the nail
Starting Point
The ideal nail entry point is the same regardless of approach: just medial to the lateral tibial spine on a true AP view.
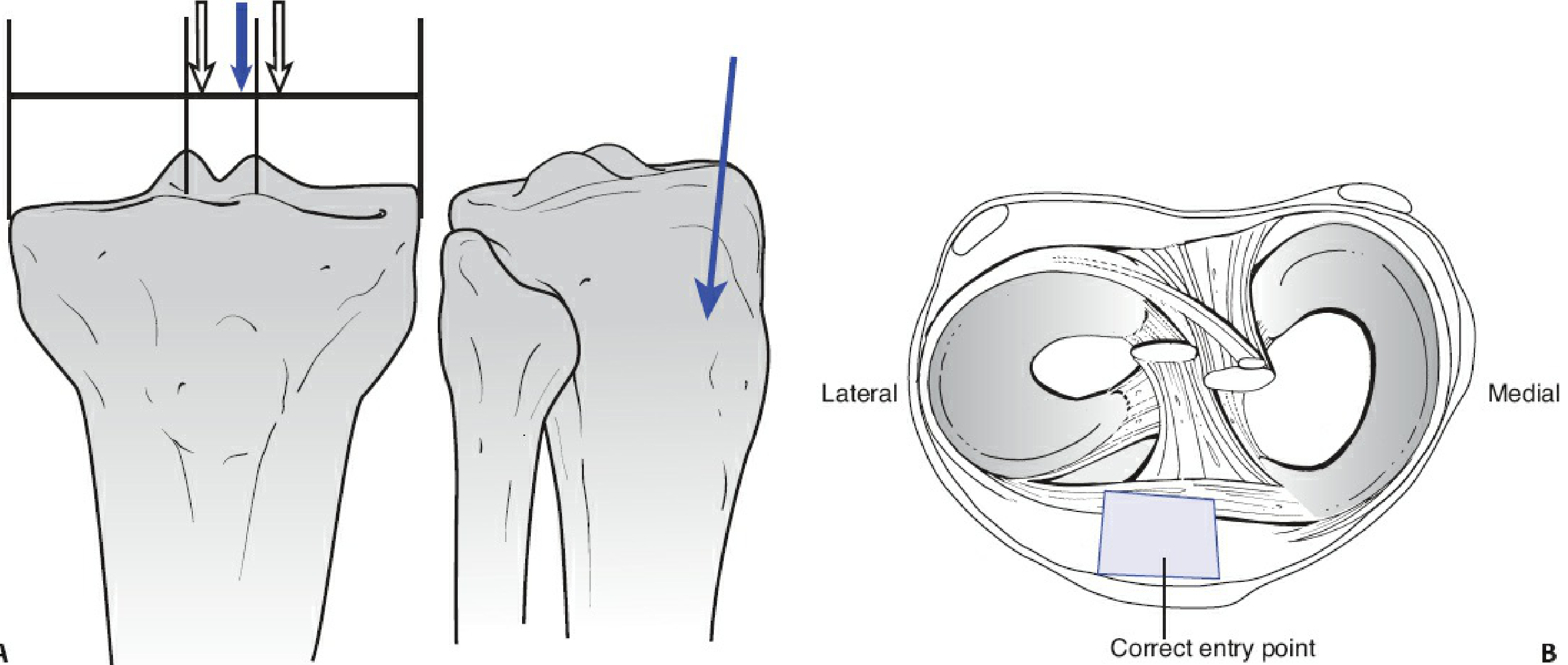
Correct starting point is medial to the lateral tibial spine (AP), and anterior to important intra-articular structures (cross-section).
Critical: Use a true AP radiograph (fibula bisected by the lateral tibial cortex at the joint) to confirm starting point - rotation can shift the apparent position by up to 15 mm.
Starting Wire Trajectory
- Coronal plane (AP): In line with the long axis of the tibia
- Sagittal plane (lateral): Parallel to the anterior tibial cortex
- A parallel wire guide ("Gatling gun") is helpful for SP nailing since knee flexion is limited - this helps achieve proper sagittal angle
- Alternatively, remove the cannula temporarily while positioning the wire, then carefully replace before reaming
Reaming and Nail Insertion
- Entry reamer opens a path through the proximal tibial metaphysis through the cannula (protecting the joint)
- Sequential reaming to appropriate diameter
- Nail inserted in standard fashion
- Locking screws:
- Diaphyseal/proximal fractures: Typically 2 distal screws (single may suffice for length-stable patterns); at least 3 proximal screws for proximal patterns
- Distal fractures: Minimum 3 distal screws, including AP and/or oblique orientation for rotational stability
Advantages Over Infrapatellar Approach
| Advantage | Explanation |
|---|---|
| Easier starting point | Patella does not obstruct ideal wire trajectory |
| Improved proximal fracture alignment | Extensor mechanism less deforming force in semi-extended position |
| Improved distal fracture alignment | Studies show lower malalignment rates |
| Better fluoroscopic imaging | Easier AP/lateral views with the leg flat |
| Shorter operative time | Less positioning adjustment needed |
| Easier fracture reduction | Leg supported on table neutralizes gravity and muscular deforming forces |
Pitfalls and How to Avoid Them
| Pitfall | Prevention |
|---|---|
| Proximal varus (SP-specific) | Too lateral a start = nail pushed medially. Use correct medial-to-lateral-spine start point |
| Apex anterior / procurvatum | Starting wire angled too posterior. Use Gatling gun guide; parallel anterior cortex on lateral view |
| Malalignment in proximal fractures | Reduce fracture before reaming; use blocking screws; do not rely on nail to reduce |
| Patellofemoral chondral injury | Use protective cannula/trocar throughout; never ream without cannula in place |
| Knee joint contamination (open fractures) | Consider infrapatellar approach for high-grade open injuries |
- Rockwood and Green's Fractures in Adults, 10th ed., p. 3219-3220
Proximal Fracture Malalignment - Key Point
The SP approach was specifically created to address the high malreduction rates (reported 55-85%) seen in proximal tibial fractures with infrapatellar nailing. In the SP approach:
- The patella does not block the ideal starting path
- The semi-extended position reduces pull from the extensor mechanism
- Blocking (Poller) screws can still be added for additional control
However, no approach is foolproof - careful attention to start point and angle is required regardless.
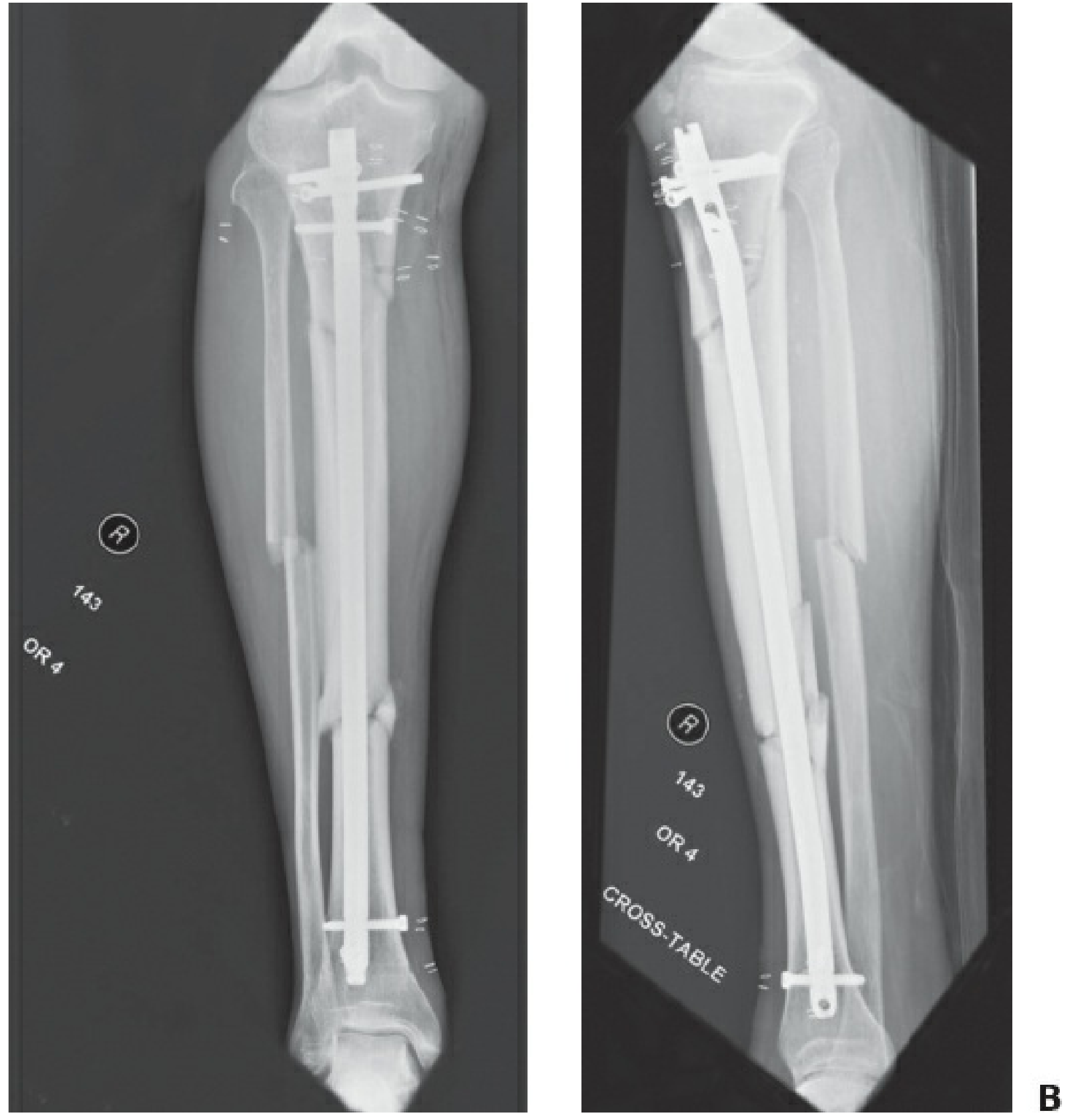
Post-op AP and lateral radiographs of a segmental tibia fracture fixed via suprapatellar approach - note well-aligned nail.
Knee Pain After Nailing
Anterior knee pain is common after tibial IM nailing (19-73% of patients, all approaches). Current evidence does not support a reproducible difference in knee pain rates between infrapatellar and suprapatellar nailing. Earlier studies suggesting SP had less knee pain were not confirmed in larger, appropriately powered trials. The etiology is multifactorial.
- Rockwood and Green's, p. 3228
Recent Evidence (2024-2025)
Three recent meta-analyses are relevant:
- Lu K et al. (2024) - Systematic review comparing suprapatellar, parapatellar, and infrapatellar tibial nailing. [PMID: 39325161] (Arch Orthop Trauma Surg)
- Hu J & Huang X (2025) - Meta-analysis of RCTs comparing suprapatellar vs. infrapatellar nailing; found suprapatellar had shorter operative time and improved functional (Lysholm) scores. [PMID: 41034881] (BMC Musculoskelet Disord)
- Xu H et al. (2025) - Systematic review comparing IMN vs. MIPO for proximal tibial fractures. [PMID: 40671027] (J Orthop Surg Res)
Summary
The suprapatellar IM nail is the preferred approach when:
- Nailing proximal or distal tibia fractures where alignment is at risk
- Fluoroscopic access is difficult with the standard hyperflexed position
- You want to minimize deforming forces during nailing
The technique requires a specialized cannula system, proper patient positioning (semi-extended, foam under proximal tibia), a correct starting point medial to the lateral tibial spine, and careful attention to wire trajectory in both planes. Outcomes and knee pain rates are comparable to infrapatellar techniques in most modern studies.
TKR
Asking for Preferences
Finding Sources
Searching the Web
total knee replacement surgical technique implants 2025
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from Campbell's and Miller's. Here is a detailed, well-organized overview of TKR surgical technique and implants.
Total Knee Replacement (TKR) - Surgical Technique & Implants
Indications for Surgery
- Debilitating pain affecting activities of daily living
- Pain not controlled by conservative measures
- Medical fitness for surgery
- No active infection anywhere in the body
- Miller's Review of Orthopaedics, 9th ed., p. 473
Preoperative Planning
Radiographs Required
- Standing bilateral AP views of both knees
- Extension and flexion lateral views
- Sunrise (Merchant) view for patellofemoral assessment
- Standing full-length AP (hip to ankle) when bony angular deformity is present, or extreme height (<60 in / <152 cm or >75 in / >190 cm)
Radiographic Analysis Goals
- Determine femoral and tibial end cuts
- Locate femoral canal entry site
- Identify bone defects and joint subluxation
- Identify ligament stretch-out (order revision system if varus thrust is present)
- Anticipate ligament releases and degree of constraint needed
Surgical Approach
The standard approach is a medial parapatellar arthrotomy:
- Midline skin incision
- Medial arthrotomy from the quadriceps tendon, around the medial side of the patella, to the tibial tubercle
- Patella everted or subluxed laterally
- Extrasynovial fat pad may be partially excised for exposure
Alternative approaches include midvastus, subvastus, and lateral parapatellar (for valgus knees).
Alignment Philosophy
Mechanical Alignment (Most Common)
The goal is a neutral mechanical limb line (Mikulicz line) - a straight line from the center of the femoral head through the center of the knee to the center of the ankle.
Femoral Cuts
- The anatomic axis of femur (AAF) is defined by the medullary canal
- An intramedullary guide rod is inserted to define this axis
- The valgus cut angle (typically 4-7 degrees) is set into the cutting jig
- This angle = AAF - MAF (mechanical axis of femur)
- Distal femoral cut is made perpendicular to the mechanical axis (MAF)
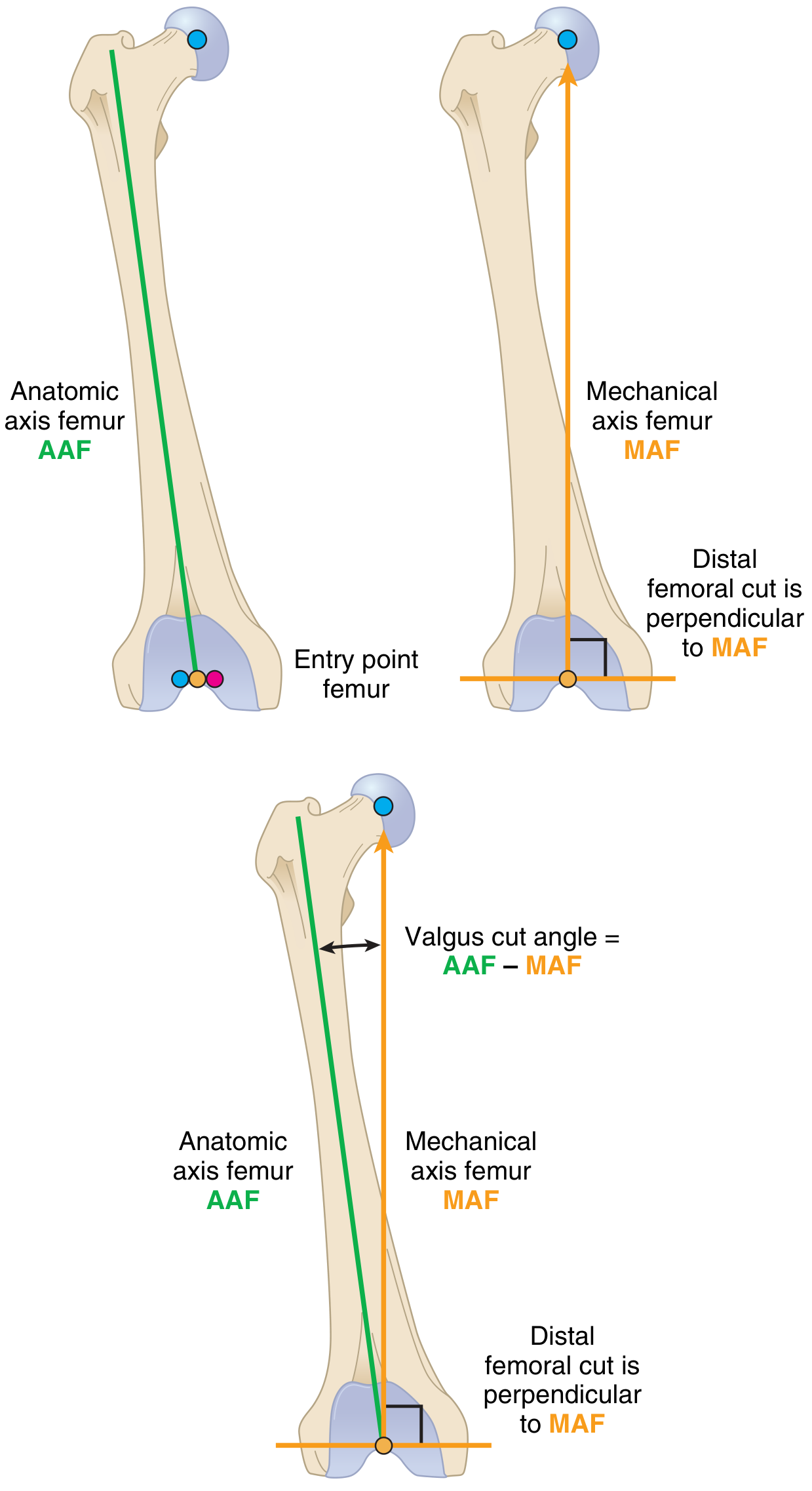
The distal femoral cut is made perpendicular to MAF. The valgus cut angle compensates for the natural offset between the anatomic and mechanical axes.
Tibial Cuts
- The anatomic axis of tibia (AAT) bisects the tibial medullary canal
- Both intramedullary and extramedullary cutting jigs are acceptable
- Proximal tibial cut is made perpendicular to the mechanical axis of the tibia (MAT)
- Tibial slope (posterior slope of ~3-7 degrees) is built into most cutting jigs
Alternative Alignment Philosophies
- Kinematic alignment - cuts made to restore native joint line orientation rather than creating a neutral mechanical axis
- Restricted kinematic alignment - compromise between mechanical and kinematic approaches
Precision Alignment Technologies
| Technology | Description |
|---|---|
| Patient-specific instrumentation (PSI) | Preop CT generates custom cutting jigs; no medullary guides needed. AAOS: no superior outcomes vs. conventional |
| Digital navigation | Real-time digitized model from intraoperative landmark registration |
| Robotics | Computer model + robotic arm guides surgeon's bone cuts. No difference in outcomes per AAOS |
| Digital pressure sensors | Trial tibial implants measure compartment pressures in real-time for gap balancing |
Bone Cuts (Sequence)
- Distal femoral cut - perpendicular to MAF at valgus cut angle (4-7°)
- Proximal tibial cut - perpendicular to MAT, with posterior slope
- Anterior femoral cut - parallel to anterior femoral cortex
- Posterior femoral cut and chamfer cuts - define flexion gap
- Patellar cut (if resurfacing) - minimum residual patellar thickness 13 mm (below this = fracture risk)
Gap Balancing ("Balancing the Gaps")
The goal is a symmetric rectangular flexion gap = symmetric rectangular extension gap.
Extension Gap
Determined by: distal femoral cut + proximal tibial cut
Flexion Gap
Determined by: posterior femoral cut + proximal tibial cut
Coronal Plane - Ligament Releases for Varus Knee (Medial Tightness)
| Structure | Release | Effect |
|---|---|---|
| Deep MCL / posteromedial capsule | Subperiosteal off tibia | Extension + flexion balancing |
| Semimembranosus | Off tibia | Extension tightness |
| Posterior capsule | Off tibia | Extension contracture |
Coronal Plane - Ligament Releases for Valgus Knee (Lateral Tightness)
| Structure | Notes |
|---|---|
| IT band (pie-crust or Z-lengthening) | Extension tightness |
| Posterolateral capsule | Extension tightness |
| Popliteus tendon | Tight in flexion only - release off anterior lateral epicondyle |
| LCL | Released last - affects both extension and flexion |
Implant Types
1. Cruciate-Retaining (CR)
- PCL retained - provides femoral rollback
- Flatter tibial polyethylene surface
- Requires ability to balance the PCL (within ~1-2 mm)
- Better tolerated when joint line is preserved (sensitive to joint line elevation)
- Technically more demanding; if PCL balance is inadequate, can convert to PS intraoperatively
2. Posterior-Stabilized (PS) - "Cruciate-Substituting"
- PCL excised; cam-and-post mechanism substitutes for PCL function
- Post on tibial insert engages femoral box in flexion to drive rollback
- Box cutout on femoral component removes additional bone
- Tolerates mild joint line elevation better than CR
- Patellar clunk syndrome - fibrous tissue catches in femoral box; reduced with longer trochlear groove designs
- Easier to balance in severe varus/PCL-deficient cases
3. Varus-Valgus Constrained (CCK - Constrained Condylar Knee)
- Enlarged tibial post + deeper femoral box - resists varus/valgus forces
- Does not control hyperextension/recurvatum
- Used for: instability, severe valgus with MCL insufficiency, failed primary TKA
- Typically requires intramedullary stems (cemented or press-fit)
- 10-year survivorship ~97.6% in primary use for complex cases
4. Hinged Prostheses
- Maximum constraint - for massive bone loss, failed prior revisions, tumor resection
- Higher complication rates than other designs
5. Mobile-Bearing / Rotating Platform
- Tibial bearing can rotate relative to tibial tray
- Theoretical advantage: reduced polyethylene stress and potential longer wear
- Often used with CCK designs to dissipate higher torque loads
AAOS 4-Star Evidence Statements (Implant Design)
- No difference in outcomes between PS and CR designs
- No difference with all-polyethylene vs. modular tibial component
- No difference in pain or function with or without patellar resurfacing
- Similar outcomes with cemented vs. cementless tibial fixation
Fixation: Cement vs. Cementless
| Feature | Cemented | Cementless |
|---|---|---|
| Gold standard | Yes - most widely used | Growing use in younger patients |
| Fixation | Polymethylmethacrylate (PMMA) | Porous ingrowth surfaces (HA-coated, titanium) |
| Tibial outcomes | Comparable per AAOS | Comparable per AAOS |
Patellar Tracking & Resurfacing
Patellar tracking is affected by:
- Q angle (tibial tubercle - trochlear groove distance; TT-TG)
- Femoral component rotation (must be parallel to epicondylar axis / Whiteside's line)
- Tibial component rotation (tibial tubercle as reference)
- Joint line level
"No Thumb" Test (Lateral Patellar Tracking)
At 90° of flexion, release all retractors - the patella should track centrally without lateral subluxation. If it subluxes, lateral retinacular release may be needed.
Patellar Resurfacing
- Minimum remaining bone = 13 mm
- Risk of osteonecrosis if lateral superior genicular artery transected during lateral release
- Blood supply mainly from inferomedial geniculate artery (disrupted with medial arthrotomy)
Perioperative Pearls
Blood Loss Management
- Tranexamic acid (TXA) - IV or topical both effective; reduces blood loss and transfusion; safe in high-risk patients (prior DVT/PE, AF, coronary stents); contraindicated in seizure disorder
- Tourniquet use: reduces intraoperative blood loss but increases short-term postoperative pain; no difference in functional outcomes
Antibiotic Prophylaxis
- Cefazolin is best (24 hr max); good bone penetration
- Non-cefazolin alternatives (vancomycin, clindamycin) have higher infection rates
- 97% of patients with stated penicillin allergy are cefazolin-tolerant on testing
Pain Management (AAOS/AAHKS Strong Recommendations)
- IV/oral acetaminophen: safe, does not increase complications
- NSAIDs (oral preop/early postop) and IV ketorolac: reduce pain and opioid use
- Pregabalin (but not gabapentin): reduces opioid consumption
- Adductor canal block (ACB) + iPACK block = best combination for perioperative analgesia and early ambulation (superior to femoral nerve block for preserving quad strength)
- Periarticular injection (PAB) by surgeon: additive to ACB and iPACK
Intraoperative Complications
| Complication | Cause / Note |
|---|---|
| Peroneal nerve palsy | Most common with valgus + flexion contracture, or aberrant posterolateral retractor placement crushing nerve against fibular neck. Treat: flex knee, remove compression. Resolves in most within 3 months |
| Lateral superior genicular artery transection | During lateral retinacular release - increases patellar osteonecrosis risk |
| Femoral notching | Anterior femoral cut extends ≥3 mm below anterior cortex - increases supracondylar fracture risk; use bypass stem in weak bone; avoid manipulation |
| Arterial injury | Popliteal artery at risk during posterior capsule work - rare but catastrophic |
Key Design Differences: CR vs. PS Summary
| Feature | CR | PS |
|---|---|---|
| PCL | Retained | Sacrificed |
| Tibial polyethylene | Flatter | Central post |
| Femoral component | No box | Cam box cutout |
| Joint line sensitivity | High | Moderate |
| Varus/PCL-deficient cases | Difficult | Preferred |
| Patellar clunk risk | No | Yes (reduced with modern designs) |
Sources: Miller's Review of Orthopaedics, 9th ed., pp. 473-485; Campbell's Operative Orthopaedics, 15th ed. 2026, pp. 491-494.
ANTERO MEDIAL OSTEOARTHRITIS
Finding Sources
Searching the Web
anteromedial osteoarthritis knee unicompartmental arthroplasty
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
anteromedial osteoarthritis knee unicompartmental arthroplasty
Reading File
Searching the Web
anteromedial osteoarthritis knee Goodfellow White definition ACL intact Oxford UKA criteria
Reading Web Page
https://musculoskeletalkey.com/unicondylar-knee-replacements…
Finding Sources
Reading Web Page
https://www.grupocaneva.com/wp-content/uploads/2021/09/Oxfor…
Searching the Web
anteromedial osteoarthritis knee White Goodfellow 1991 pathology lateral compartment preserved posterior cartilage intact
Excellent - I now have comprehensive material. Here is a detailed, well-structured overview.
Anteromedial Osteoarthritis (AMOA) of the Knee
Definition & Historical Origin
Anteromedial osteoarthritis (AMOA) was first formally described and named by White, Ludkowski, and Goodfellow (1991) from the Nuffield Orthopaedic Centre, Oxford (J Bone Joint Surg Br, PMID: 2071640). It describes a distinct clinicopathological subtype of knee OA characterized by:
"Medial compartment full-thickness cartilage and bone erosion centered anteriorly on the tibial plateau, with posterior cartilage preserved, an intact ACL, and functional MCL - producing a correctable varus deformity."
It is the primary indication for the Oxford Unicompartmental Knee Arthroplasty (UKA).
Pathology - The AMOA Lesion
The hallmark is the anteromedial distribution of wear:
| Location | Finding |
|---|---|
| Anteromedial tibial plateau | Full-thickness cartilage and bone erosion |
| Posterior medial tibial plateau | Cartilage preserved (key diagnostic feature) |
| Medial femoral condyle | Corresponding anterior/central erosion on inferior surface |
| Lateral compartment | Intact full-thickness cartilage |
| ACL | Functionally intact |
| MCL | Functionally intact (not structurally shortened) |
On the excised tibial plateau at surgery, this is seen as erosion of the central and anterior portions with cartilage surviving posteriorly - the direct macroscopic confirmation of AMOA.
Why Does AMOA Occur? - The ACL Mechanism
The intact ACL is the defining structural basis of this pattern.
- The ACL prevents forward tibial subluxation during gait
- Because the tibia cannot slide forward, contact forces remain in the anterior and central zone of the medial compartment during the mid-stance / extension phase of gait
- The posterior cartilage is never loaded heavily - so it is preserved
- The lateral compartment is similarly unloaded in the coronal plane (the MCL remains at normal tension in flexion)
When the ACL fails, tibial contact shifts posteriorly:
- The wear pattern extends to the posterior plateau
- Fixed varus deformity develops (unlike the correctable varus of AMOA)
- Lateral compartment degeneration supervenes
- The disease is no longer AMOA - and UKA becomes inappropriate
This is why radiographic assessment of the lateral X-ray is central to diagnosis: an intact ACL produces anterior wear; a deficient ACL produces posterior subluxation and posterior wear.
Clinical Features
- Medial knee pain, worse on loading
- Varus deformity in extension - from bone and cartilage loss medially
- Correctable varus - when knee is flexed to 90°, MCL is tensioned by preserved posterior cartilage, restoring near-normal alignment
- No fixed varus (fixed varus = posterior disease = ACL insufficiency)
- Preserved range of motion - flexion usually >110°
- Fixed flexion deformity <15° typically
Radiological Assessment (Oxford Criteria for UKA)
Three key radiographic views form the diagnostic decision aid:
1. Weight-Bearing AP (or Rosenberg PA 20° flexion view)
- Demonstrates medial bone-on-bone contact (or bone loss)
- Full-thickness medial compartment loss
2. True Lateral View (Femoral Condyles Overlapping)
- Assesses ACL integrity indirectly
- ACL intact = tibial plateau centered under femur, posterior cartilage rim preserved
- ACL deficient = posterior tibial erosion and anterior subluxation of tibia under femur
3. Valgus Stress View (20° Flexion)
- Full-thickness lateral cartilage must be confirmed (lateral joint space opens to normal)
- Confirms correctable varus - if varus corrects to neutral, MCL and soft tissues are functionally intact
- If lateral compartment narrows = lateral disease - UKA contraindicated
Patient Selection for Medial UKA (Oxford Criteria)
Positive Selection Criteria (All Must Be Met)
- ACL and PCL functionally intact
- Cartilage/bone erosion limited to anterior and middle medial compartment; posterior medial and lateral compartment have normal cartilage
- MCL not structurally shortened (varus deformity correctable)
- Patellofemoral joint damage limited to medial facets (lateral PFJ intact)
- Fixed flexion deformity <15 degrees
- Flexion to ≥110 degrees (under anesthesia)
- Pain causing functional limitation
- Patient compliance
Features That Do NOT Preclude Oxford UKA
- Isolated medial pain is not required - anterior knee pain does not compromise outcome
- Age, weight, activity level - not exclusion criteria per Oxford data
- Chondrocalcinosis (cartilage calcification on X-ray)
- Lateral marginal osteophytes
- Medial tibial subluxation (corrects once ACL-intact UKA is implanted)
- Full-thickness cartilage loss on non-weight-bearing medial side of lateral femoral condyle
Absolute Contraindications
- Inflammatory arthritis (RA, etc.)
- ACL-deficient knee with clinical instability / posterior tibial erosion
- Fixed varus deformity (posterior disease)
- Lateral compartment full-thickness cartilage loss
- Lateral PFJ subluxation or significant lateral patellar damage
- Severe flexion contracture >15°
Treatment Options
Conservative Management (Early / Moderate Disease)
- Weight loss, physiotherapy, activity modification
- Analgesics, NSAIDs
- Intra-articular corticosteroids (avoid within 2 weeks of planned surgery)
- Bracing (valgus unloading brace)
- High tibial osteotomy (HTO) - for younger patients with varus AMOA and intact ACL, corrects mechanical axis
Surgical Management
1. Medial Unicompartmental Knee Arthroplasty (UKA) - Treatment of Choice for AMOA
- Resurfaces only the medial compartment
- Preserves ACL, PCL, MCL, lateral compartment, patellofemoral joint
- Most commonly used implant: Oxford Phase 3 (mobile-bearing)
Advantages over TKA in AMOA:
- Preserves proprioception and more natural kinematics
- Faster recovery, shorter hospital stay
- Less blood loss
- Better functional scores (Oxford Knee Score, WOMAC, Forgotten Joint Score)
- Patients feel the knee is "more normal"
- Day-of-surgery / outpatient procedure feasible
Oxford UKA Survival:
- 98% at 10 years (Oxford series)
- 93% at 15 years (independent series)
- Average polyethylene wear rate of 0.03 mm/year (mobile bearing)
2. Total Knee Arthroplasty (TKA)
- Indicated when criteria for UKA not met, or patient/surgeon preference
- NICE (UK) stipulates patients with AMOA should be offered a choice of UKA or TKA
- Functional outcomes comparable to UKA in most studies, but UKA superior in patient-reported outcomes in many series (higher Oxford Knee Score, better Forgotten Joint Score)
3. High Tibial Osteotomy (HTO)
- Considered in younger patients (<60 years) with:
- Varus AMOA
- Intact ACL
- Good lateral compartment
- High physical demands
- Shifts mechanical axis from medial to lateral, reducing medial compartment load
Oxford UKA Surgical Technique (Key Steps)
- Approach: Minimal medial parapatellar incision (minimally invasive)
- ACL check: Hook the ACL arthroscopically/directly to confirm integrity before proceeding
- Osteophyte removal: All osteophytes removed from medial compartment to unmask true ligament lengths
- Tibial cut:
- Vertical tibial cut medial to ACL origin (blade angled toward femoral head)
- Horizontal tibial cut perpendicular to tibial axis with appropriate slope
- Femoral preparation: Spherical mill used to create curved femoral surface (matching Oxford femoral component's spherical shape)
- Sizing: Excised tibial plateau used as template to select tibial size
- Trialing: Gap and stability checked in flexion and extension
- Implantation: Tibial component, mobile polyethylene bearing, femoral component cemented into position
- Intraoperative check: Bearing should move freely and not dislocate; knee should be stable and balanced
The excised tibial plateau confirms AMOA at surgery - eroded anteriorly, preserved cartilage posteriorly.
ACL-Deficient Knee and UKA
- Oxford group have used UKA in clinically stable ACL-deficient patients with selected outcomes
- Fixed-bearing UKA is more commonly used in ACL-deficient cases (less risk of bearing dislocation without posterior constraint)
- Clinically unstable ACL-deficient knee = TKA preferred (altered kinematics risk disease progression)
- ACL-deficiency severity correlates with worse outcomes in fixed-bearing UKA (PMID: 40050997)
Summary: AMOA vs. TKA/UKA Decision at a Glance
| Feature | Favors UKA | Favors TKA |
|---|---|---|
| ACL status | Intact | Deficient / unstable |
| Wear pattern | Anteromedial only | Posterior / lateral / tricompartmental |
| Varus | Correctable | Fixed |
| Lateral compartment | Full-thickness intact | Any loss |
| PFJ | Medial facet only affected | Lateral subluxation / severe damage |
| Flexion | >110° | <110° |
| Flexion contracture | <15° | >15° |
| Inflammatory arthritis | No | No (affects all types) |
Key reference: White SH, Ludkowski PF, Goodfellow JW. "Anteromedial osteoarthritis of the knee." J Bone Joint Surg Br. 1991;73(4):582-6. PMID: 2071640
Oxford UKA Surgical Technique Manual (Zimmerbiomet/Oxford Phase 3)
Campbell's Operative Orthopaedics, 15th Ed. 2026 - Unicompartmental Knee Arthroplasty
This is a shared conversation. Sign in to Orris to start your own chat.