Acute coronary syndromes
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute coronary syndrome" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive, well-structured response. Let me compile it.
Acute Coronary Syndromes (ACS)
Definition and Classification
Acute coronary syndrome describes the clinical continuum of myocardial ischemia and infarction caused by acute disruption of coronary blood flow. It is divided into three entities based on ECG findings and cardiac biomarkers:
| Entity | ST elevation | Troponin | Mechanism |
|---|---|---|---|
| Unstable Angina (UA) | No | Negative | Subtotal occlusion; ischemia without necrosis |
| NSTEMI | No | Positive | Subtotal occlusion; myonecrosis confirmed |
| STEMI | Yes (>20 min) | Positive | Total occlusion; transmural infarction |
UA and NSTEMI together are called NSTE-ACS because both lack persistent ST elevation. - Goldman-Cecil Medicine, p. 638
Epidemiology
- ~1.2 million hospitalizations annually in the United States for ACS
- ~2/3 are NSTE-ACS
-
50% of NSTE-ACS patients are older than 65 years; nearly half are women
- Risk is higher with atherosclerosis risk factors, peripheral vascular disease, and chronic inflammatory conditions (rheumatoid arthritis, psoriasis, SLE, chronic infection)
Pathobiology
Type 1 vs. Type 2 MI
- Type 1 MI: Rupture or erosion of an atherosclerotic plaque → platelet aggregation → thrombus → reduced/absent coronary flow (the vast majority of ACS)
- Type 2 MI: Oxygen supply-demand mismatch without plaque rupture - caused by severe hypotension, anemia, hypoxemia, tachycardia, hypertension, or thyrotoxicosis. Treatment targets the underlying cause.
Plaque Rupture - The Central Event
Plaque rupture underlies almost all Type 1 ACS. The key steps are:
- Lipid deposition and inflammation: Oxidized LDL accumulates in the arterial wall, recruiting macrophages and T-lymphocytes to the plaque border
- Fibrous cap degradation: Inflammatory cells secrete cytokines (TNF, IL-1, IFN-γ) that inhibit collagen synthesis, and enzymes (matrix metalloproteinases, cathepsins) that degrade collagen and elastin - thinning and weakening the fibrous cap
- Mechanical vulnerability: Thin fibrous caps and sites of low shear stress (vessel bifurcations) have reduced nitric oxide and prostacyclin production, more lipid/inflammatory cell accumulation, and greater cap thinning
- Systemic inflammation: The widespread nature is evidenced by angioscopy showing plaque ulceration at multiple sites simultaneously, and by the higher ACS risk in patients with gingivitis, psoriasis, SLE, and RA
- Neovascularization: Angiogenic peptides (VEGF, FGF, placental growth factor) promote intraplaque vessel growth, contributing to plaque hemorrhage and destabilization
Thrombus Formation
After plaque rupture:
- Circulating platelets adhere to exposed subendothelial proteins and become activated
- Platelets change from discoid to stellate shape (increasing surface area), then release thromboxane, serotonin, ADP, vWF, and fibrinogen from intracellular granules
- Focal vasoconstriction and recruitment of more platelets follows
- GP IIb/IIIa receptors increase on the platelet surface; fibrinogen bridges adjacent platelets → platelet plug
- Thrombin is generated → activates more platelets and converts fibrinogen to fibrin → fibrin-rich thrombus
- Subtotal occlusion = UA/NSTEMI; total occlusion = STEMI (unless collaterals are present)
- Goldman-Cecil Medicine, p. 640
Special Mechanisms
- Prinzmetal (variant) angina: Focal coronary vasospasm from endothelial dysfunction
- Drug-induced: Cocaine, methamphetamines, chemotherapeutic agents, serotonin receptor agonist "triptans" - increase demand and/or cause vasospasm
- Spontaneous coronary artery dissection (SCAD): Most common in peripartum women and vasculitis patients
Clinical Manifestations
Symptoms
- Classic: retrosternal pressure, squeezing, or heaviness - may radiate to the left arm, neck, or jaw
- May be intermittent/recurrent or persistent
- Accompanying diaphoresis, dyspnea, nausea
Atypical Presentations (especially in elderly and women)
- In patients >85 years, chest pain is present in only ~50% with STEMI
- Older patients and women more often present with: dyspnea, syncope, diaphoresis, shoulder/back pain, abdominal pain, weakness, fatigue, or delirium
- One-third of women >65 years with AMI present with abdominal pain alone
- Delayed presentations with acute heart failure (~50% of STEMI in those >85 years) - Rosen's Emergency Medicine
Diagnosis
ECG (should be interpreted within 10 minutes of arrival)
- STEMI: Persistent ST elevation >20 minutes → prompt reperfusion
- NSTE-ACS: ST depression or transient ST elevation + T wave changes in up to 50%
- A normal ECG does not exclude ACS - ~5% of ACS patients discharged from the ED have a normal initial ECG
- Left circumflex territory ischemia may be missed on standard 12-lead; use posterior leads V7-V9 or right-sided leads
- Deep (>2 mm) symmetrical anterior T-wave inversion suggests significant left main or proximal LAD stenosis
- Serial ECGs at 15-30 minute intervals during the first hour
Serum Biomarkers
- High-sensitivity troponin (hs-cTn) is the gold standard - can detect myonecrosis within 2 hours of symptom onset
- The 0h/1h algorithm (ESC 2020) uses the absolute value at 0h and the change (Δ) at 1 hour to rapidly rule in or rule out NSTEMI
NSTE-ACS Triage Algorithm (ESC 2020)
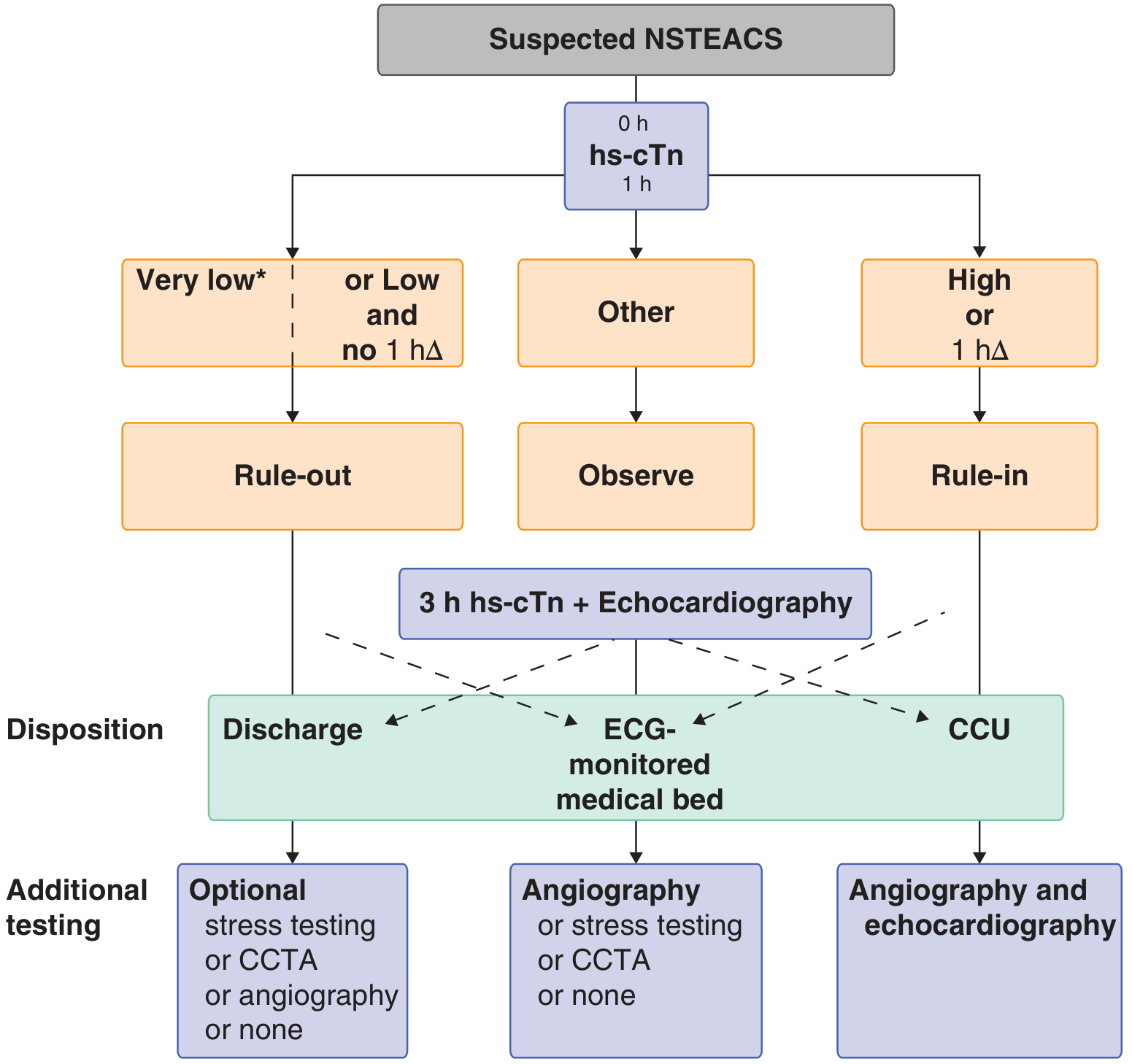
- Rule-out: hs-cTn very low at 0h, OR low at 0h with no significant 1h rise → discharge with optional stress test/CCTA
- Observe: Intermediate values → repeat at 3h + echocardiography → ECG-monitored bed
- Rule-in: High hs-cTn at 0h OR significant 1h rise → CCU admission + angiography + echocardiography
Coronary Angiography Findings in NSTE-ACS
- Left main disease: ~15%
- 3-vessel disease: 30-35%
- 2-vessel disease: 20-30%
- 1-vessel disease: 20-30%
- No significant stenosis: ~15% (consider INOCA, vasospasm, SCAD)
- Key: 2/3 of culprit lesions had <50% stenosis on prior imaging - previously "non-significant"
Risk Stratification
Two validated algorithms guide treatment intensity:
| Score | Variables | Use |
|---|---|---|
| TIMI (0-7) | Age ≥65, ≥3 CAD risk factors, known stenosis >50%, ST deviation, ≥2 anginal events in 24h, ASA use in 7d, elevated markers | Simple bedside tool |
| GRACE | Age, HR, SBP, creatinine, Killip class, cardiac arrest, ST deviation, elevated markers | More accurate for mortality prediction |
Both balance the risk of ischemic events against the risk of bleeding from aggressive therapy.
Management
General Initial Measures
- Continuous ECG monitoring, IV access, oxygen only if SpO₂ <90%
- Aspirin 162-325 mg chewed immediately
- Sublingual nitroglycerin for ongoing chest pain (avoid if hypotension or right ventricular MI)
- Morphine for refractory pain (use cautiously - can mask symptoms and delay P2Y12 absorption)
Antithrombotic Therapy
Antiplatelet agents (dual antiplatelet therapy - DAPT):
- Aspirin (irreversibly inhibits COX-1/thromboxane A2): loading 162-325 mg, then 75-100 mg daily
- P2Y12 inhibitors (block ADP-mediated platelet activation via GP IIb/IIIa):
- Clopidogrel (prodrug, requires CYP2C19 activation) - 300-600 mg load, 75 mg daily
- Ticagrelor (reversible, faster onset) - 180 mg load, 90 mg twice daily (preferred in most guidelines)
- Prasugrel (irreversible, potent) - 60 mg load, 10 mg daily; avoid in prior stroke/TIA or age >75
Anticoagulants:
- Unfractionated heparin (UFH): weight-based IV infusion; preferred when PCI likely (reversible with protamine)
- Low-molecular-weight heparin (enoxaparin): 1 mg/kg SC twice daily; non-inferior to UFH in most settings
- Fondaparinux: 2.5 mg SC daily; preferred when PCI not planned (lower bleeding risk)
- Bivalirudin: direct thrombin inhibitor; used as alternative during PCI
GP IIb/IIIa inhibitors (abciximab, eptifibatide, tirofiban): for high-risk NSTEMI/PCI; block the final common pathway of platelet aggregation
Invasive vs. Conservative Strategy
- Early invasive approach (angiography within 24-72h) is recommended for high-risk NSTE-ACS (elevated troponin, dynamic ECG changes, GRACE score >140, refractory symptoms, hemodynamic instability)
- Conservative approach: acceptable for low-risk patients without recurrent symptoms
- AHA guidelines specify no absolute age limit for revascularization - elderly patients, including octogenarians, benefit from early invasive strategy (After Eighty Study)
- Revascularization options: PCI (preferred for single or double vessel disease) or CABG (preferred for left main, triple vessel disease, or diabetes)
Medical Therapy
| Drug class | Mechanism | Role in ACS |
|---|---|---|
| Beta-blockers | Reduce HR and contractility → lower O₂ demand | Start within 24h if no contraindication; continue long-term post-MI |
| ACE inhibitors/ARBs | Prevent adverse LV remodeling | Start early, especially if EF <40%, hypertension, or diabetes |
| Statins (high-intensity) | LDL lowering + plaque stabilization | Start immediately regardless of baseline LDL |
| Nitrates | Vasodilate coronary arteries | Symptom relief; no mortality benefit |
| Aldosterone antagonists | Reduce remodeling | Add if EF <40% + HF or diabetes, and no renal/K⁺ contraindication |
STEMI-Specific: Reperfusion
- Primary PCI is the preferred reperfusion strategy if door-to-balloon time can be achieved within 90 minutes (or 120 min if transfer required)
- Fibrinolysis (tenecteplase, alteplase, streptokinase): if PCI is unavailable within 120 minutes; administer within 12h of symptom onset
- Absolute contraindications to fibrinolysis: prior hemorrhagic stroke, ischemic stroke within 3 months, intracranial neoplasm, active internal bleeding, suspected aortic dissection
Complications
| Complication | Timing | Notes |
|---|---|---|
| Ventricular fibrillation | Early (first 24-48h) | Immediate defibrillation |
| Cardiogenic shock | Hours-days | Requires inotropes, IABP, or LVAD; urgent revascularization |
| Acute heart failure | Hours-days | Especially in elderly and large infarcts |
| Mechanical complications | 3-7 days | Free wall rupture, VSD, papillary muscle rupture (mitral regurgitation) |
| Pericarditis (Dressler's) | Weeks-months | Autoimmune; treat with aspirin/NSAIDs/colchicine |
| LV thrombus | Days-weeks | Anticoagulate if detected |
Secondary Prevention
- DAPT for 12 months post-ACS (then aspirin alone long-term)
- High-intensity statin (atorvastatin 40-80 mg or rosuvastatin 20-40 mg) - target LDL <55 mg/dL per ESC or <70 mg/dL per ACC/AHA
- Beta-blocker: continue for at least 1 year; debate ongoing for patients with preserved EF (a recent 2025 meta-analysis suggests uncertain benefit in post-MI patients without reduced EF or HF)
- ACE inhibitor/ARB indefinitely if EF reduced
- Lifestyle: smoking cessation, cardiac rehabilitation, diet, exercise
- A 2025 Lancet meta-analysis (PMID 40902613) found that clopidogrel was non-inferior to aspirin for secondary prevention of coronary artery disease in individual patient data analysis - suggesting aspirin's role as the default long-term agent may be revisited
Sources: Goldman-Cecil Medicine (International Edition, pp. 637-641), Rosen's Emergency Medicine, 2020 ESC Guidelines for NSTE-ACS management (adapted in Goldman-Cecil Figure 57-2).
This is a shared conversation. Sign in to Orris to start your own chat.