Thromolytic drugs pharmacology detailed
Reading File
Finding Sources
Finding Sources
Searching PubMed
thrombolytic therapy pharmacology fibrinolysis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data. Let me compile the complete detailed pharmacology answer.
Thrombolytic (Fibrinolytic) Drugs - Detailed Pharmacology
1. Overview of the Fibrinolytic System
The fibrinolytic system is the body's mechanism for dissolving unwanted clots. Its central reaction is the conversion of the inactive zymogen plasminogen into the active serine protease plasmin, which then cleaves fibrin into soluble fibrin degradation products (FDPs).
Fibrinolytic System & Regulation:
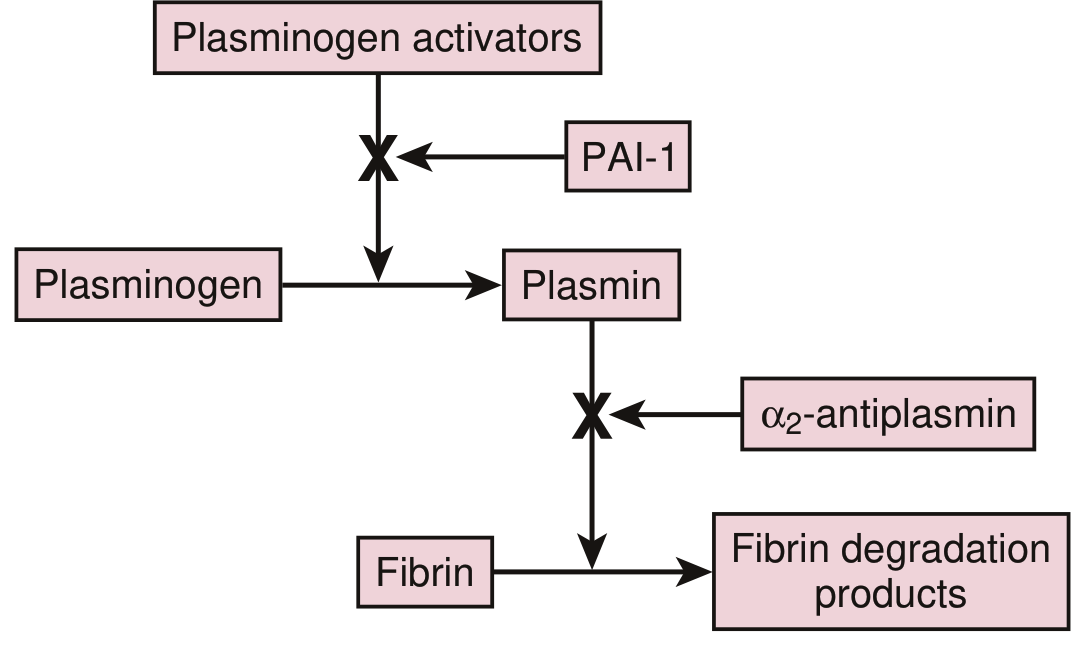
The system is regulated at two levels:
- PAI-1 (Plasminogen Activator Inhibitor-1): Inhibits plasminogen activators (t-PA, u-PA). Synthesized by endothelial cells.
- α₂-Antiplasmin: Rapidly inhibits circulating free plasmin.
Under physiologic conditions, t-PA and plasminogen both bind to fibrin, forming a ternary complex that confines plasmin generation to the clot surface. Plasmin generated at the fibrin surface is protected from α₂-antiplasmin because its kringle domains are occupied by fibrin. This localizes fibrinolysis to the thrombus.
With pharmacologic doses of plasminogen activators, plasmin concentrations can exceed α₂-antiplasmin, producing the systemic lytic state - where free plasmin degrades fibrinogen and coagulation factors V and VIII, raising bleeding risk.
2. Classification of Thrombolytic Agents
| Generation | Agents | Fibrin Specificity |
|---|---|---|
| 1st generation | Streptokinase, Urokinase | Non-specific |
| 2nd generation | Alteplase (t-PA) | Fibrin-specific |
| 3rd generation | Reteplase, Tenecteplase | Fibrin-specific (modified) |
3. Individual Drug Pharmacology
A. Streptokinase (1st Generation)
Source: Produced by β-hemolytic streptococci. Not an enzyme itself.
Mechanism of Action:
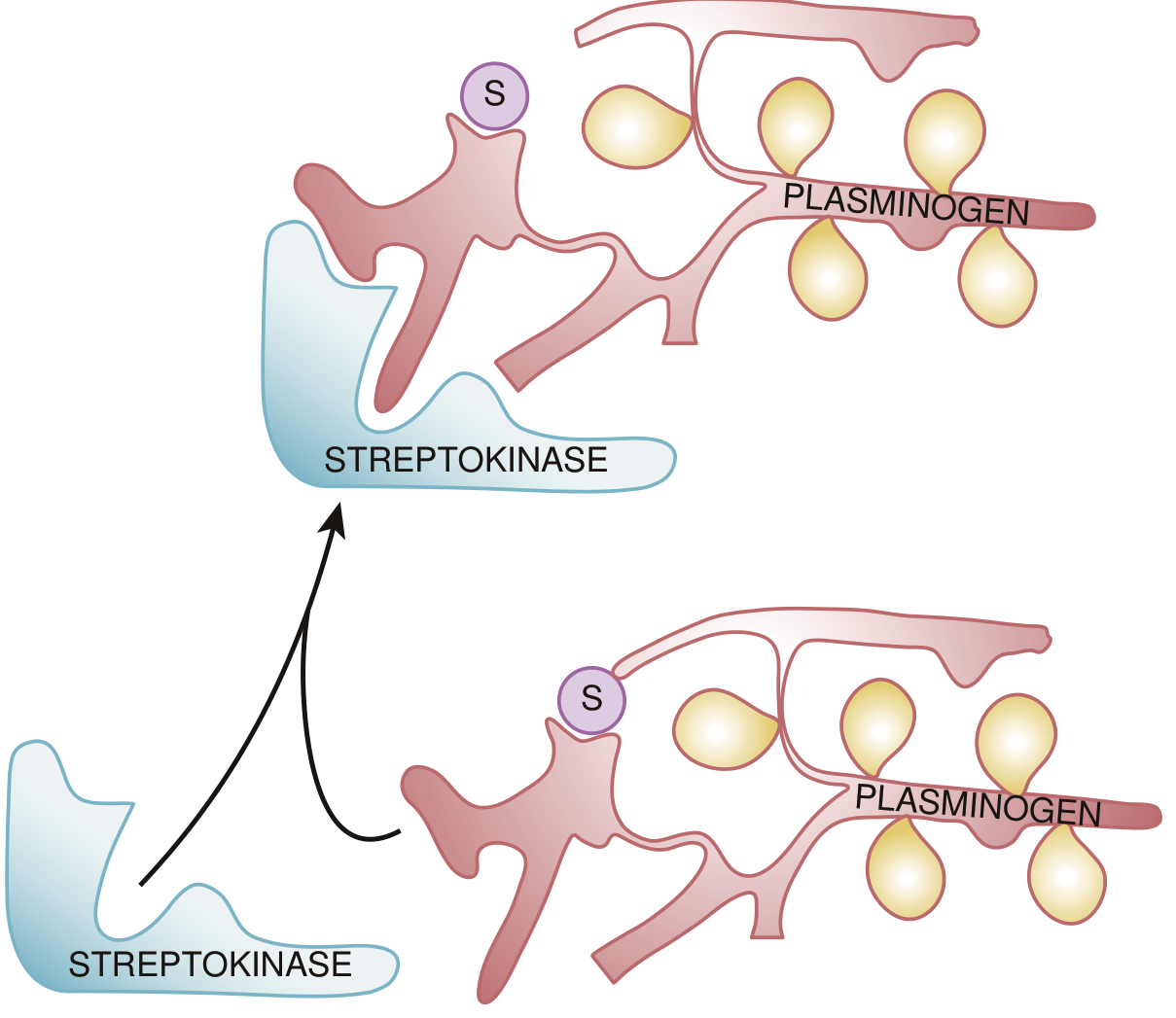
Streptokinase forms a 1:1 stoichiometric complex with plasminogen. This binding induces a conformational change in plasminogen that exposes its active site. The streptokinase-plasminogen complex then acts as an activator of additional free plasminogen molecules, converting them to plasmin. This is unique - streptokinase is not itself an enzyme but an allosteric modifier of human plasminogen.
- Streptokinase has no affinity for fibrin, so it activates both free (circulating) and fibrin-bound plasminogen equally
- This generates so much plasmin that it overwhelms α₂-antiplasmin → systemic lytic state (non-fibrin-specific)
Dosing: IV infusion of 1.5 million units over 30-60 minutes for acute MI.
Adverse Effects:
- Allergic reactions (~5%): rash, fever, chills, rigors; rare anaphylaxis
- Hypotension: plasmin-mediated bradykinin release from kininogen; responds to leg elevation, IV fluids, low-dose dopamine/norepinephrine
- Antibody formation: prior streptococcal infection or prior use → reduced efficacy (cannot repeat within 6-12 months)
- Hemorrhage
Availability: No longer available in the USA; still used in some other countries.
B. Anistreplase (APSAC - Anisoylated Plasminogen Streptokinase Activator Complex)
Mechanism: Streptokinase is combined with equimolar Lys-plasminogen. The active site exposed on this combination is then masked with an anisoyl group. After IV infusion, the anisoyl group is slowly removed by deacylation (t½ ~100 min for deacylation). This gives a longer effective half-life and allows single-bolus dosing.
- Like streptokinase, it is non-fibrin-specific and induces the systemic lytic state
- Shares the same allergic profile and antibody limitations
- No longer available in the USA
C. Urokinase (u-PA, 1st Generation)
Source: Originally isolated from human urine; now recombinant. A serine protease.
Mechanism:
- Urokinase directly converts plasminogen to plasmin without requiring fibrin
- Synthesized as single-chain u-PA (scu-PA), which has minimal enzymatic activity. Plasmin converts it to the active two-chain form
- Two-chain u-PA activates plasminogen in the absence or presence of fibrin → non-fibrin-specific
- Binds u-PA receptor (u-PAR) on cell surfaces for pericellular proteolysis and tissue remodeling
- No antibody formation (not bacterial); lower antigenicity than streptokinase
Uses: Catheter-directed thrombolysis for peripheral/DVT thrombi. No longer available in the USA.
D. Alteplase (rt-PA, 2nd Generation) - Drug of Choice
Nature: Recombinant serine protease. Single-chain polypeptide converted to two-chain form by plasmin (both forms are active).
Structure: Five discrete domains:
- Fibronectin-like finger domain (binds fibrin)
- Epidermal growth factor (EGF) domain
- Two kringle domains (kringle-2 binds fibrin)
- Serine protease domain
Mechanism of Action (Fibrin-Specific):
- In the absence of fibrin, t-PA is a poor plasminogen activator
- When bound to fibrin, its activity increases by at least 3 orders of magnitude (≥1000-fold)
- Fibrin acts as a template that co-localizes t-PA and plasminogen, greatly accelerating their interaction
- As fibrin degrades, more Lys residues are exposed, providing additional binding sites → positive feedback amplification of fibrinolysis
- Plasmin generated on the fibrin surface is protected from α₂-antiplasmin because its kringle domains are occupied
- At therapeutic concentrations (300-3000 ng/mL), some systemic plasminogen activation still occurs
Pharmacokinetics:
- Physiologic t-PA levels: 5-10 ng/mL
- t½: ~5 minutes (very short)
- Clearance: primarily hepatic metabolism
Dosing:
- Acute MI: 15-mg IV bolus → 0.75 mg/kg over 30 min (max 50 mg) → 0.5 mg/kg over 60 min (max 35 mg). Total ≤100 mg.
- Acute ischemic stroke: 0.9 mg/kg IV (max 90 mg), 10% as bolus, remainder over 60 min, within 4.5 hours of symptom onset
- Massive PE: 100 mg over 2 hours
Clinical Indications:
- Acute MI (STEMI) - though mechanical PCI now preferred
- Acute ischemic stroke (within 4.5 h)
- Massive/submassive pulmonary embolism
- Deep vein thrombosis (catheter-directed)
- Peripheral arterial occlusion
Adverse Effects:
- Hemorrhage (major): 2-4% serious bleeding with concurrent heparin; intracranial hemorrhage in ~1% of stroke patients
- Does NOT cause allergic reactions (recombinant human protein)
- No antibody formation
- Does NOT cross the placenta
E. Reteplase (rPA, 3rd Generation)
Nature: Deletion mutant of alteplase lacking the finger domain, EGF domain, and kringle-1 domain.
Advantages over alteplase:
- Longer half-life (~15-18 min) → allows double-bolus dosing (10 U + 10 U, 30 min apart)
- Lower fibrin binding affinity (due to absent finger domain) - this paradoxically may allow better thrombus penetration
- More convenient administration
Efficacy: Similar to alteplase in clinical trials. Similar toxicity profile.
F. Tenecteplase (TNK-tPA, 3rd Generation)
Nature: Mutant of alteplase with three specific amino acid substitutions (T103N, N117Q, KHRR-AAAA). This engineered molecule has:
- Longer half-life (~20-24 min) → allows single-bolus dosing
- Increased fibrin specificity (compared to alteplase)
- Resistance to PAI-1 inhibition (the KHRR→AAAA substitution in the protease domain)
Dosing: Single IV weight-based bolus (30-50 mg based on body weight) for STEMI.
Advantages: Single-bolus ease of administration, PAI-1 resistance. Efficacy and toxicity are comparable to alteplase overall.
Recent evidence: Tenecteplase is increasingly used as an alternative to alteplase in acute ischemic stroke (TNK-tPA), particularly for bridging to thrombectomy (PMID 41599613 - 2025 review).
4. Comparison Table
| Feature | Streptokinase | Urokinase | Alteplase | Reteplase | Tenecteplase |
|---|---|---|---|---|---|
| Source | Streptococci | Human/recombinant | Recombinant | Recombinant | Recombinant |
| Fibrin specificity | Non-specific | Non-specific | High | Moderate | Highest |
| Mechanism | Complex w/ plasminogen | Direct plasminogen activator | Fibrin-bound activation | Fibrin-bound activation | Fibrin-bound activation |
| PAI-1 resistance | No | No | No | No | Yes |
| Half-life | ~30 min | ~15 min | ~5 min | ~15-18 min | ~20-24 min |
| Administration | IV infusion 30-60 min | Infusion | Infusion (weight-based) | Double bolus | Single bolus |
| Allergic reactions | Yes (~5%) | Rare | No | No | No |
| Antibody formation | Yes | No | No | No | No |
| Systemic lytic state | Severe | Moderate | Mild | Mild | Least |
| Available (USA) | No | No | Yes | Yes | Yes |
5. Common Contraindications to Thrombolytic Therapy
Absolute:
- Prior intracranial hemorrhage at any time
- Known structural cerebral vascular lesion (AVM, aneurysm)
- Ischemic stroke within 3 months (except within 4.5 h for alteplase)
- Active internal bleeding (excluding menses)
- Significant closed head or facial trauma within 3 months
- Suspected aortic dissection
- Intracranial neoplasm
Relative:
- History of severe hypertension (BP >180/110 mmHg on presentation)
- Prior ischemic stroke >3 months, dementia, or intracranial pathology
- Traumatic/prolonged CPR (>10 min) or major surgery within 3 weeks
- Recent (within 2-4 wk) internal bleeding
- Non-compressible vascular punctures
- Pregnancy
- Active peptic ulcer
- Current anticoagulant therapy (elevated INR/aPTT)
6. Hemorrhagic Toxicity
All thrombolytics increase bleeding risk via two mechanisms:
- Direct degradation of hemostatic plugs at sites of vascular injury
- Systemic lytic state - plasmin degrades fibrinogen and factors V and VIII
Intracranial hemorrhage is the most feared complication (~1% with alteplase for stroke). This is why mechanical thrombectomy is now preferred over systemic thrombolysis for STEMI and large vessel occlusion strokes where feasible.
7. Management of Thrombolytic-Induced Hemorrhage
If serious bleeding occurs:
- Stop the thrombolytic infusion immediately
- Apply local pressure
- Antifibrinolytics: ε-aminocaproic acid or tranexamic acid (both are lysine analogues that compete for lysine-binding sites on plasminogen/plasmin, blocking fibrin interaction)
- Fresh frozen plasma (FFP) and cryoprecipitate to replace fibrinogen and other depleted factors
- Packed red blood cells as needed
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics (14e); Harrison's Principles of Internal Medicine (22e, 2025); Braunwald's Heart Disease (12e); Lippincott Illustrated Reviews Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.