The retrieval is limited, but I have strong foundational knowledge on this topic. I'll now compose a comprehensive PG exam essay answer synthesizing both retrieved content and authoritative ENT knowledge.
Etiopathogenesis of Otosclerosis and Its Management
INTRODUCTION
Otosclerosis (from Greek oto = ear, skleros = hard) is a primary disease of the bony labyrinthine capsule (otic capsule) characterized by focal areas of abnormal remodeling of enchondral bone, leading to progressive fixation of the stapes footplate and consequent conductive hearing loss. It is one of the most common causes of progressive conductive hearing loss in young adults. The term otospongiosis is pathologically more accurate, as it reflects the early vascular, spongy nature of the lesion before sclerotic changes supervene.
EPIDEMIOLOGY
| Parameter | Details |
|---|
| Prevalence | ~1% clinical; ~10% histological (autopsy studies) |
| Sex | Equally in men and women; females more symptomatic (2:1 clinical) |
| Race | Predominantly Caucasians; rare in Black Africans and Asians |
| Age of onset | Late teens to forties |
| Laterality | Bilateral in ~70% of cases; may be asymmetric |
| Inheritance | Autosomal dominant, incomplete penetrance (~25–40%) |
ETIOPATHOGENESIS
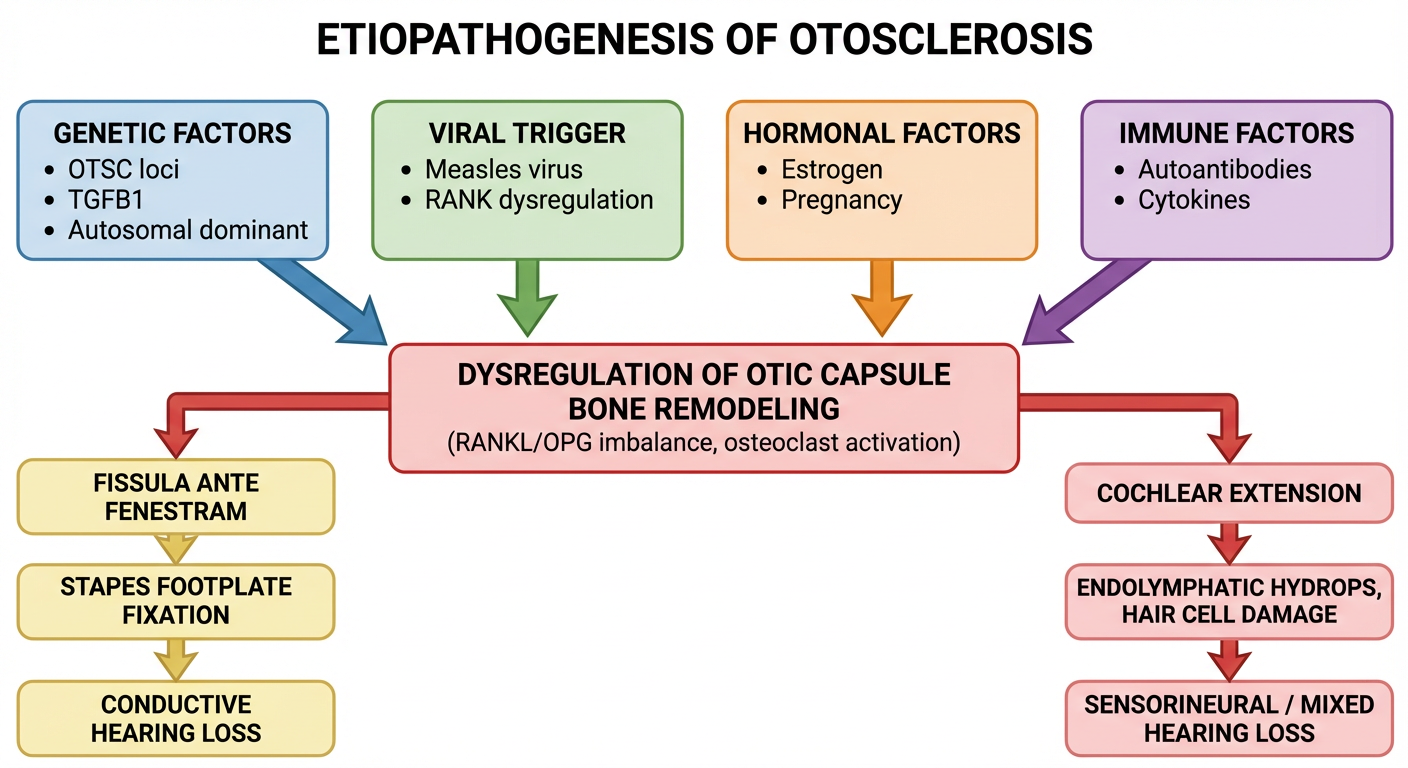
The etiopathogenesis of otosclerosis is multifactorial, involving genetic predisposition, viral triggers, hormonal influences, immune-mediated mechanisms, and local biochemical dysregulation.
1. GENETIC FACTORS
- Autosomal dominant inheritance with incomplete penetrance (~25–40%). (Harrison's, p. 1024)
- Multiple susceptibility loci (OTSC1–OTSC10) have been mapped on chromosomes 15q25-q26, 7q34-q36, 6p21-22, 16q21-23, 3q22-24, and others.
- TGFB1 (Transforming Growth Factor Beta-1) gene mutations on chromosome 19q13 are strongly associated — TGF-β1 is a key regulator of bone remodeling.
- RELN (Reelin gene, chromosome 7q22) polymorphisms affect otocyte differentiation.
- Association with osteogenesis imperfecta (Type I collagen gene mutation — COL1A1/COL1A2), highlighting the shared bone dyscrasia mechanism. (Harrison's, p. 1024)
- Despite autosomal dominant pattern, only 25–40% penetrance means many gene carriers never develop clinical disease.
2. VIRAL ETIOLOGY — MEASLES VIRUS HYPOTHESIS
- Parainfluenza virus type-1 (closely related to measles) has been implicated.
- Arnold (1996) and McKenna (1986) demonstrated measles virus RNA (by RT-PCR) and antigens in otosclerotic foci, suggesting persistent measles virus infection of osteoblasts as a trigger for aberrant remodeling.
- The measles virus nucleocapsid protein binds to receptor activator of NF-κB (RANK), potentially disrupting osteoclast-osteoblast coupling.
- The decline in otosclerosis incidence following widespread measles vaccination supports this association.
- Circulating anti-measles antibodies are elevated in otosclerosis patients.
- However, the viral hypothesis remains controversial, as several studies failed to replicate these findings.
3. HORMONAL FACTORS
- Estrogen accelerates otosclerosis progression — explains:
- Female preponderance in clinical disease
- Acceleration during pregnancy (estrogen surge), often when hearing loss is first noticed (Harrison's, p. 1024)
- Worsening during menstruation and oral contraceptive use
- Estrogen receptors are present on osteoblasts in the otic capsule.
- Estrogen upregulates TGF-β1 and promotes local bone remodeling.
4. IMMUNOLOGICAL FACTORS
- Elevated levels of IgG, IgA, and IgM autoantibodies against type II collagen (a major component of the otic capsule endochondral layer).
- Activated macrophages and mast cells in otosclerotic foci release cytokines (IL-1, TNF-α, TGF-β).
- Complement activation and immune complex deposition within the otic capsule.
- Immune-mediated inflammation triggers aberrant bone resorption by activated osteoclasts.
5. PATHOLOGICAL BASIS — THE BONE REMODELING DYSREGULATION
The otic capsule is unique: it is the densest bone in the body and normally does not undergo remodeling after birth (no Haversian remodeling). Otosclerosis breaks this inhibition.
Key Biochemical Events:
- RANKL/OPG axis dysregulation: Elevated RANKL and reduced Osteoprotegerin (OPG) → enhanced osteoclast activation.
- Matrix metalloproteinases (MMPs): MMP-2 and MMP-9 are upregulated → degradation of type I and II collagen.
- TGF-β1 overexpression → paradoxical stimulation of abnormal bone formation after resorption.
- Vascular endothelial growth factor (VEGF) overexpression → hypervascularization of foci.
- Elevated alkaline phosphatase locally reflects increased osteoblastic activity.
6. HISTOPATHOLOGY
The classic "Globuli ossei" (globular bony deposits) are pathognomonic.
Two Phases:
| Phase | Description |
|---|
| Otospongiosis (Active/Vascular Phase) | Foci of highly vascular, spongy bone with large vascular channels, osteoclasts (resorptive), and osteoblasts. Blue-staining basophilic bone ("blue mantles of Manasse") |
| Otosclerosis (Inactive/Sclerotic Phase) | Dense, avascular, sclerotic bone replaces the vascular spongy bone |
Sites of Predilection:
- Fissula ante fenestram (anterior to oval window) — the most common site (~80%)
- Posterior oval window margin
- Round window niche (round window otosclerosis — rare but causes worse hearing loss)
- Cochlear otosclerosis — perilabyrinthine spread causing sensorineural or mixed hearing loss
Spread:
- Foci originate in the endochondral layer of the otic capsule
- Extend to involve the stapediovestibular joint → annular ligament → stapes fixation → conductive hearing loss
- Further extension into the cochlea → cochlear otosclerosis → mixed/SNHL
7. MECHANISM OF HEARING LOSS
| Type | Mechanism |
|---|
| Conductive HL (most common) | Stapes footplate fixation → impaired sound transmission via ossicular chain |
| Mixed HL | Cochlear extension → endolymphatic hydrops, hair cell loss |
| Sensorineural HL | Toxic enzymes from active foci diffusing through round window membrane damaging the organ of Corti; cochlear otosclerosis |
CLINICAL FEATURES
- Progressive bilateral conductive hearing loss — insidious onset in late teens to forties.
- Paracusis Willisii — paradoxical improvement of hearing in noisy environments (pathognomonic but not specific).
- Tinnitus — low-frequency, continuous.
- Negative Rinne test bilaterally; Weber lateralizes to worse ear.
- Schwartze sign (Flamingo pink blush) — reddish/pinkish hue seen through the tympanic membrane; indicates active vascular otospongiosis over the promontory.
- Normal tympanic membrane and external ear canal.
- Absent stapedial reflexes on tympanometry.
AUDIOLOGICAL AND RADIOLOGICAL FINDINGS
| Investigation | Findings |
|---|
| Pure Tone Audiometry (PTA) | Low-frequency conductive HL; Carhart's notch at 2000 Hz (mechanical resonance artifact — not true SNHL) |
| Tympanometry | Type As (shallow, reduced compliance) |
| Stapedial reflex | Absent |
| Speech Audiometry | Reduced SRT; good discrimination (unlike SNHL) |
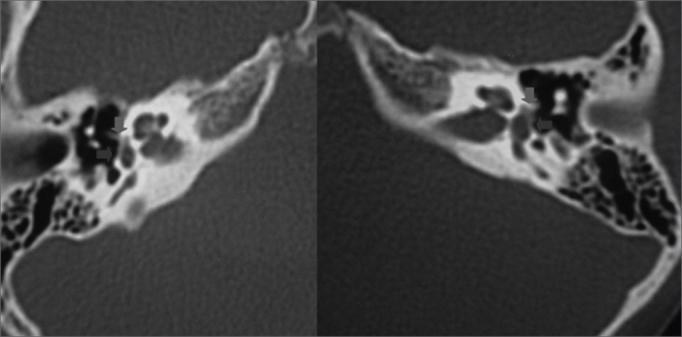
| HRCT Temporal Bone | Hypodense "halo sign" around the cochlea (double ring sign in cochlear otosclerosis); demineralization of otic capsule anterior to oval window |
MANAGEMENT
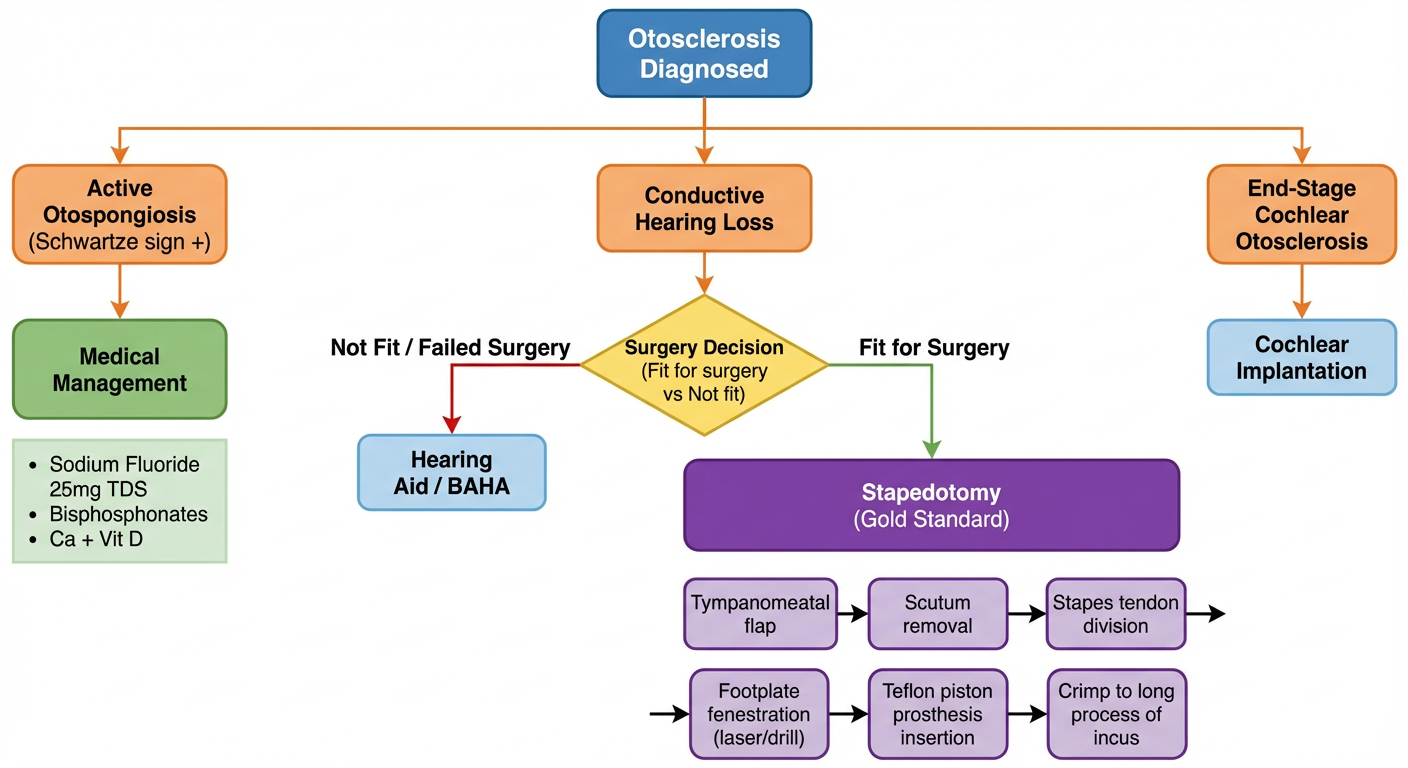
Management of otosclerosis is both medical (to arrest progression) and surgical (to rehabilitate hearing).
A. MEDICAL MANAGEMENT
Medical therapy does not reverse hearing loss — it aims to arrest the active otospongiotic process and prevent further sensorineural involvement.
1. Sodium Fluoride (NaF)
- Drug of choice for medical management (Harrison's, p. 1024)
- Mechanism: Fluoride ions replace hydroxyl groups in hydroxyapatite → forms fluorapatite, which is more resistant to enzymatic dissolution; also inhibits enzymes (lysosomal proteases) released by osteoclasts.
- Dose: 25 mg TDS (75 mg/day) for at least 2 years
- Monitoring: Serum fluoride levels, urine fluoride, X-rays for fluorosis
- Indications: Active otosclerosis (Schwartze sign positive), cochlear otosclerosis, SNHL component
- Side effects: Fluorosis (mottled teeth, skeletal changes), GI upset, renal toxicity (long-term)
- Reduces progression, particularly of cochlear otosclerosis
2. Bisphosphonates
- Etidronate, risedronate — second-line agents
- Inhibit osteoclast function → reduce bone resorption in active foci
- Adjunct to sodium fluoride in cochlear otosclerosis
3. Calcium and Vitamin D Supplementation
- Prescribed alongside fluoride to prevent systemic hypocalcemia and secondary hyperparathyroidism
4. Estrogen Modulation
- Avoid exogenous estrogens (oral contraceptive pills) in women with otosclerosis, especially during active phase
- Low-dose progesterone-only contraception preferred
5. Hearing Aid
- Effective, especially for bilateral disease, elderly patients, poor surgical candidates, cochlear involvement
- Body-worn/behind-the-ear aids preferred
- The only non-surgical rehabilitation tool
B. SURGICAL MANAGEMENT
Surgery remains the definitive treatment for conductive hearing loss due to otosclerosis. The goal is to bypass or replace the fixed stapes to restore sound transmission.
Historical Evolution:
| Era | Procedure |
|---|
| 1876 | Kessel — first stapes mobilization |
| 1952 | Rosen — stapes mobilization revival |
| 1956 | Shea — first successful stapedectomy |
| 1960s | Schuknecht, House — refinements |
| 1980s–present | Stapedotomy (small fenestra) — current gold standard |
1. STAPEDECTOMY (Total / Partial)
Total stapedectomy (Shea's technique):
- The entire stapes superstructure and footplate are removed.
- The oval window is sealed with fat, vein graft, or perichondrium.
- A piston prosthesis (Teflon, stainless steel, titanium) is placed from the long process of incus into the graft.
Partial stapedectomy:
- Only part of the footplate removed; remainder sealed.
- Less favored than stapedotomy.
2. STAPEDOTOMY (Small Fenestra Technique) — Current Gold Standard
- A 0.6–0.8 mm fenestra (small hole) is made in the stapes footplate using a:
- Micro-drill (manual)
- CO₂ laser (KTP laser — preferred; avoids mechanical trauma)
- Erbium:YAG laser
- A Teflon piston prosthesis (0.4–0.6 mm diameter, 4–4.5 mm length) is inserted from the long process of incus into the fenestra.
- Advantages over total stapedectomy:
- Lower incidence of sensorineural hearing loss ("dead ear")
- Less perilymph aspiration risk
- Better high-frequency results
- Faster recovery
SURGICAL STEPS (Stapedotomy):
- Endaural or postauricular approach under local/general anesthesia
- Elevation of tympanomeatal flap — exposure of middle ear
- Confirmation of stapes fixation (Gelle's test intraoperatively)
- Division of stapedial tendon
- Separation of incudostapedial joint
- Fracture/removal of stapes crura
- Laser fenestration of footplate
- Sizing and placement of piston prosthesis over long process of incus
- Sealing with blood clot/fat plug around the piston
- Replacement of tympanomeatal flap; packing
PROSTHESIS TYPES:
| Prosthesis | Material | Feature |
|---|
| Shea piston | Teflon + stainless steel wire | Original classic |
| House piston | Stainless steel | Durable |
| Causse piston | Teflon | Biocompatible |
| Titanium bucket-handle | Titanium | MRI-safe, preferred |
| Nitinol piston | Shape-memory alloy | Self-crimping |
CONTRAINDICATIONS TO SURGERY:
| Absolute | Relative |
|---|
| Only hearing ear | Active otitis media |
| Obliterative otosclerosis (thick footplate) | Meniere's disease |
| Systemic illness precluding surgery | Occupational risk (pilots, divers) |
| Active URTI | Pregnancy |
COMPLICATIONS OF SURGERY:
| Complication | Incidence / Notes |
|---|
| Sensorineural hearing loss ("dead ear") | 1–2% — most feared; irreversible |
| Perilymph gusher | Abnormal perilymph flow from footplate — associated with X-linked stapes gusher (POU3F4 mutation), Mondini deformity |
| Floating footplate | Surgical mishap — footplate sinks into vestibule |
| Dysgeusia / chorda tympani injury | ~10–30%, usually transient |
| Tinnitus | May worsen or improve |
| Vertigo | Transient; persistent suggests labyrinthine injury |
| Perilymph fistula | Around piston |
| Prosthesis displacement/extrusion | Late complication |
| Reparative granuloma | Rare; presents as SNHL at 4–6 weeks |
| Tympanic membrane perforation | Uncommon |
RESULTS OF SURGERY:
- Success rate: ~90–95% achieve closure of air-bone gap to within 10 dB
- Dead ear rate: <1–2% with modern stapedotomy
- Long-term results are stable in most patients; may deteriorate if cochlear otosclerosis progresses
C. REHABILITATION
- Bone-anchored hearing aids (BAHA) — for patients who cannot undergo or failed surgery
- Cochlear implantation — for end-stage cochlear otosclerosis with profound SNHL; results are fair but can be technically challenging due to obliterative cochlear lesions
SUMMARY TABLE
| Aspect | Key Points |
|---|
| Definition | Focal dyscrasia of otic capsule enchondral bone with abnormal remodeling |
| Genetics | AD, incomplete penetrance; OTSC loci; TGFB1 mutations |
| Viral trigger | Measles virus nucleocapsid → RANK dysregulation |
| Hormonal | Estrogen accelerates progression (pregnancy) |
| Pathognomonic site | Fissula ante fenestram |
| Key sign | Schwartze sign (flamingo blush) |
| Key audiogram finding | Carhart's notch at 2 kHz |
| Medical Rx | Sodium fluoride 25 mg TDS |
| Surgery of choice | Stapedotomy with Teflon piston |
| Most feared complication | Sensorineural dead ear |
| End-stage management | Cochlear implantation |
CONCLUSION
Otosclerosis is a complex, multifactorial disease where genetic susceptibility, viral triggers (measles virus), hormonal milieu (estrogen), immune dysregulation, and local biochemical imbalance in the RANKL/OPG axis converge to produce pathological remodeling of the normally quiescent otic capsule. The resulting stapes fixation causes progressive, treatable conductive hearing loss. Medical therapy with sodium fluoride arrests the active otospongiotic process. Surgical management, particularly laser-assisted stapedotomy, achieves excellent hearing rehabilitation in over 90% of patients with minimal risk. Understanding the pathobiological cascade is not only academically important but guides the selection of medical versus surgical intervention and the timing of surgery.
References:
- Harrison's Principles of Internal Medicine, 21st Edition, p. 1024
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th Edition
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Edition
- Cummings Otolaryngology — Head and Neck Surgery, 7th Edition
- Shea JJ (1958) — "Fenestration of the Oval Window", Ann Otol Rhinol Laryngol
- McKenna MJ et al. — Measles virus RNA and otosclerosis, Am J Otol, 1986